The coronavirus continues to exert a disproportionate impact on the nation’s minority communities, which suffer from high levels of poverty and the health issues that go along with it. As the most important health insurer for people with low incomes, Medicaid is on the forefront of COVID-19 testing and treatment. Seventy percent of all Medicaid beneficiaries are enrolled in comprehensive care plans offered by managed care organizations (MCOs); how these plans perform is central to the accessibility, timeliness, and quality of COVID-19 care.
In May, the Centers for Medicare and Medicaid Services (CMS) issued an informational bulletin describing actions states could take to strengthen managed care. The bulletin discusses state Medicaid options for improving payment and care delivery and identifies certain options particularly relevant during the pandemic: temporarily increasing monthly capitation payments to reflect unforeseen costs; increasing provider fees to better reflect added pandemic response costs; and “retainer” payments to network providers that deliver personal care and habilitation services, such as personal attendants or speech therapy, to keep these providers afloat as the pandemic causes a precipitous decline in use of care.
States also are enacting reforms designed to bring MCO contracts into compliance with new federal requirements under the Families First Coronavirus Response Act (FFCRA). Enacted in March, FFCRA makes important changes in federal Medicaid policy for the duration of the declared public health emergency related to the pandemic. First, FFCRA requires states to cover COVID diagnostic testing and testing-related services without cost-sharing. Second, FFCRA ties a 6.2-percentage-point increase in federal Medicaid funding for states and the District of Columbia to their agreements to maintain eligibility at January 1, 2020, levels, guarantee continuous eligibility for beneficiaries enrolled as of January 1 or any time during the emergency period, maintain premiums charged at no more than January 1 levels, and waive any cost-sharing that otherwise would be required for COVID testing or treatment.
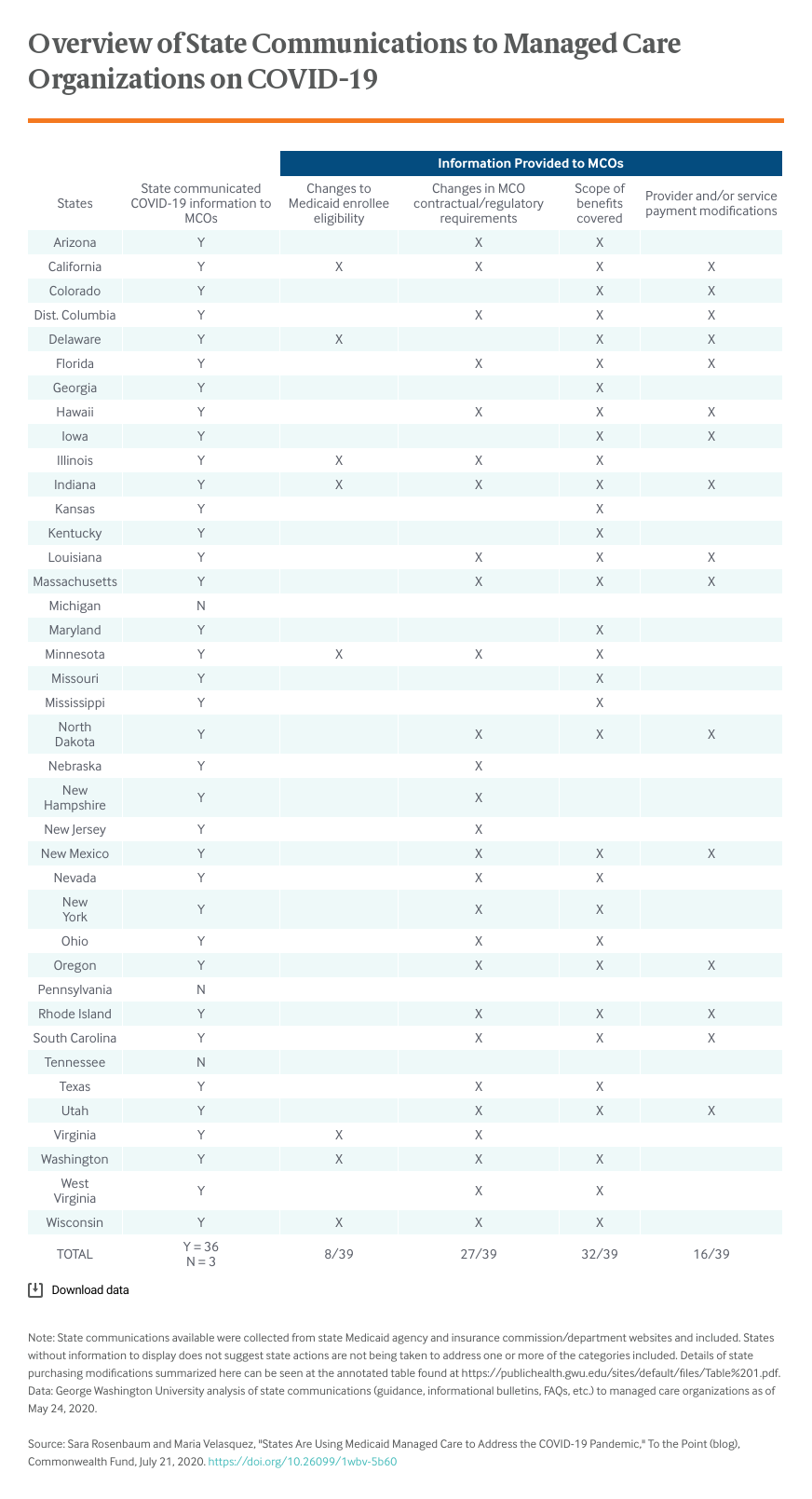
The accompanying table shows the range of activities undertaken by the end of May in the 38 states and the District of Columbia that were using comprehensive managed care plans to administer some or all of their programs. These include activities that reflect state Medicaid options, such as adjusting general payment or care principles, as well as changes made in direct response to the FFCRA reforms. As the pandemic continues, it is likely states that have not already done so will implement formal changes to managed care policies and operations.
As of the end of May, nearly all states using comprehensive managed care already had initiated one or more changes; three states (California, Illinois, and Indiana) had adopted changes across all four categories (changes to eligibility, changes in MCO contractual or regulatory requirements, scope of benefits covered, and provider payment modifications). Multiple states have sought to ease access to care and reduce provider burden in various ways: simplifying provider enrollment and credentialing to encourage network enrollment by out-of-state providers, simplifying plans’ procedures to streamline the review process when prior authorization is required, giving providers additional time to request payment, creating COVID-19 call centers, and in at least one case (Oregon) by expressly requiring culturally and linguistically appropriate outreach.
Medicaid managed care will continue to play a central role throughout the pandemic. Given the nature of the public health threat, it will be important to consider the following issues:
- Given the serious shortage of testing sites, will states require MCOs to treat all testing sites in their service areas as in-network providers or, instead, will states pay independent sites on a fee-for-service basis, similar to insurer payment for out-of-network care?
- In light of the disproportionate health risks faced by the Medicaid population, will more states either encourage or require special outreach efforts to encourage access to testing?
- For especially vulnerable populations, such as children and adults with serious and chronic health conditions or severe disabilities, will the state require special outreach, testing, and care management activities?
- How will states adjust capitation and provider payment rules to reflect the added costs of adapting plan operations and care to pandemic conditions?
- Will states develop standards for measuring the quality of care or the timeliness of care response, and will health outcome metrics be a focus of measurement?
- Given the enormous implications of living conditions for COVID vulnerability, how might states use managed care to integrate health care and social services?
- If and when a vaccine becomes available, what coverage, access, network, and payment protocols will states put in place to ensure access to immunizations in the most rapid and appropriate way?