Our Scorecard ranks every state’s health care system based on how well it provides high-quality, accessible, and equitable health care. Read the report to see health care rankings by state.
Restoring Access to Maternity Care in Rural America
Toplines
Nearly half of rural U.S. counties are maternity care deserts where lack of access to obstetric care contributes to rising maternal death rates.
Across the country, regional partnerships are rebuilding access to maternity care in efforts to improve outcomes for pregnant and parenting people in rural communities.
Toplines
Nearly half of rural U.S. counties are maternity care deserts where lack of access to obstetric care contributes to rising maternal death rates.
Across the country, regional partnerships are rebuilding access to maternity care in efforts to improve outcomes for pregnant and parenting people in rural communities.
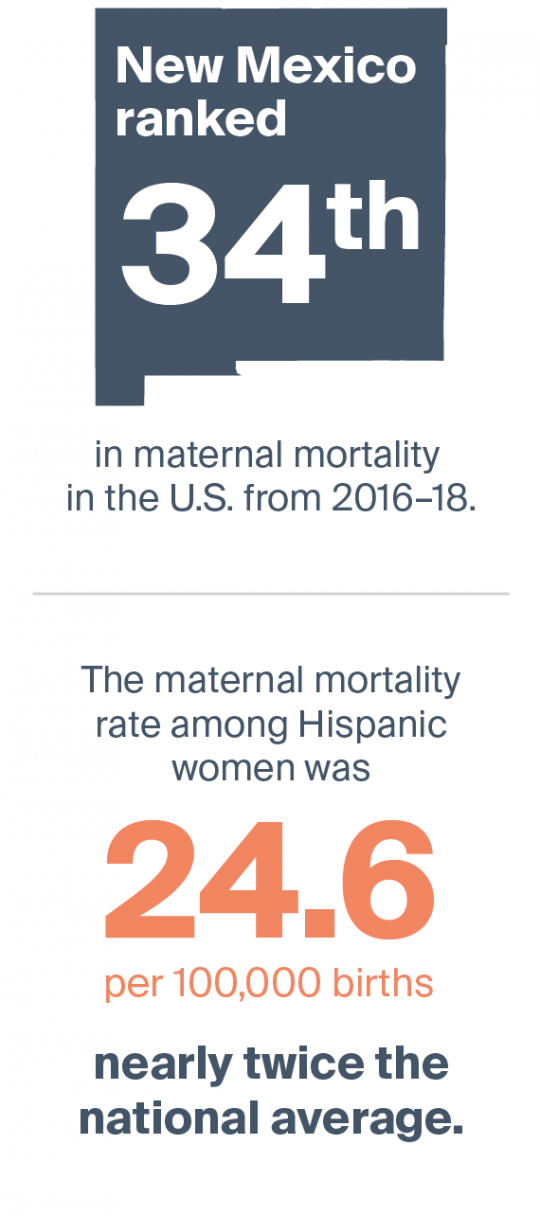
In New Mexico, one of three people who die during pregnancy and the weeks after childbirth are killed in car accidents. While some may have been driving to the grocery store, others in this largely rural state were likely driving hundreds of miles over mountainous roads and in bad driving conditions to seek medical care. Driving long distances for care and other scenarios — like giving birth in ambulances or forgoing prenatal and postpartum services — are playing out across rural communities across the country as obstetric (OB) facilities or whole hospitals close and people travel farther for maternity care. As of 2014, more than half of rural counties in the U.S. were considered maternity care deserts, with no hospital-based obstetric services; worsening access has contributed to increases in maternal mortality and morbidities among rural residents, particularly Black women.
In this issue of Transforming Care, we profile regional partnerships that aim to bolster access to maternity care in rural communities. Many use versions of the hub-and-spoke model in which obstetricians and maternal-fetal medicine specialists in urban health care organizations (the “hubs”) provide education and support to rural maternity providers (the “spokes”), who are much more likely to be family medicine physicians or nurse practitioners than obstetricians. Many also leverage remote monitoring systems to keep a closer eye on high-risk people between medical visits and field navigators to connect pregnant and parenting people to social and other supports.
Experts in the field see such efforts as first steps in rebuilding access to maternity care across the country — steps that are necessary but not sufficient to tackle maternal outcomes that are the worst among wealthy nations and relate to poverty, racism, and sexism as well as health system dysfunction. “Negative pregnancy outcomes are rising, preterm labor rates are too high, maternal mortality is too high. And probably the most embarrassing aspect of maternity care is the postpartum period. That’s the forgotten period,” says Sina Haeri, M.D., vice president of women’s health and chief of maternal-fetal medicine at Access Physicians, a large provider of telematernity and other telemedicine specialty services. “When you look at the totality of maternity health, you have to admit that it’s a flawed system.”
Creating Networks of Maternity Providers
In response to worsening access to maternity services in rural areas, the federal Office of Rural Health Policy created the RMOMS (Rural Maternity and Obstetrics Management Strategies) grant program in 2019. The goal is to encourage a range of health care providers — primary care clinicians, obstetricians, and maternal-fetal medicine specialists as well as mental health clinicians, home visiting staff, and others — to form regional networks that can fill gaps in the maternity care continuum. So far, six groups in Minnesota, Missouri, Montana, New Mexico, Texas, and West Virginia have received $21 million in funding. The participants are using similar strategies to build rural providers’ capacity, help patients navigate services, and implement telehealth to connect people across distances. Crucially, the grantees must involve their state Medicaid agencies in an effort to make their work sustainable beyond the four-year grant period. Medicaid programs cover half of all rural births.
New Mexico: Creating a Continuum of Maternity Care Providers
In New Mexico, RMOMS participants formed a collaborative, Rural OB Access and Maternal Services (ROAMS), that is working to expand access to care in five mountainous, sparsely populated counties spanning 10,000 square miles in the northeastern part of the state.1 More than half of the residents of this region are Hispanic and a third live below 150 percent of the federal poverty level. Before this work began, three of the five counties were maternity care deserts.
A key strategy is to open satellite OB clinics in rural areas. Two such clinics have opened in the past year. Open one or two afternoons a month, the clinics are housed in community health centers and staffed by medical assistants and/or nurse practitioners who perform in-person prenatal or postpartum checkups. Then, patients meet via videoconference with OB providers in the nearest labor-and-delivery hospital. During the visits, the clinics and hospitals share ultrasound images, vital signs, and other information. The hospital providers bill for their services, while the satellite clinics are supported by the grant.
For pregnant people who have higher-risk conditions such as diabetes or hypertension, OBs can prescribe a telehealth kit, which includes a tablet with embedded devices that monitor and report blood pressure, weight, oxygen level, glucose level, and fetal heart rates. Grant funds are available to help them purchase internet service and learn to use these devices. Leaders hope the telehealth kits will make people feel more involved in their care. “There’s a fear among some providers that if a mom has a home telehealth kit, she’ll never come in for her appointment,” says Colleen Durocher, ROAMS executive director. “Yet the research that we’ve seen is showing the opposite, that moms who use the telehealth tools become more engaged.”
Grant funds are also supporting the work of three family navigators who work in the satellite clinics and hospitals to screen patients for unmet medical and social needs and connect them to services. The navigators follow the Pathways Community HUB model, which gives navigators responsibility for helping people reach goals (e.g., finding health insurance or having enough food) and pays them for achieving certain milestones. “There are a lot of places that give moms a referral, but this is about making the referral stick,” says Durocher. “If mom needs help with transportation, we’ll arrange that. If mom needs help gathering the documents to enroll in insurance or other benefits, the navigator can go to her house and help her do that.”
Using the Pathways model is a part of grantees’ efforts to make this work sustainable. In some regions, Medicaid managed care plans, departments of health, and other entities pay for Pathways services. Grantees are also lobbying the state to help pay for transportation so that more pregnant people can have safe, reliable rides to medical appointments.
Missouri: Letting People Know Help Is Available
RMOMS grantees in Missouri are building a network of maternity services in what’s known as the Bootheel, six counties in the southeastern part of the state that are home to many soybean, rice, and cotton farms, but few OB providers. Two major hospitals stopped offering obstetric services in recent years, and infant and maternal outcomes have long been the worst in the state. To help health care providers understand the challenges families face accessing maternal care across a large geographic area, leaders of the collaborative, known as the Bootheel Perinatal Network, are creating a virtual video tour of the region. “We have a lot of migrant workers who are making minimum wage or less, who are often a hidden population,” says Barbara Gleason, M.S.N., RMOMS project director at Saint Francis Healthcare System in Cape Girardeau. “There’s a lot of agriculture, but there may not be good access to food. Many people don’t have cars.”
As in New Mexico, a key strategy is to encourage people to take advantage of help that is available. Early findings suggest only 5 percent of people with high-risk pregnancies are taking part in a home visiting programs. “Some people get really nervous, thinking they have to clean their house,” Gleason says. “We’re working to help them understand home visitors are there to help educate, support, and empower them.”
In addition to screening for depression during and after pregnancy using the Edinburgh Postnatal Depression Scale, RMOMS participants are using PRAPARE, a screening tool that promulgates a standardized approach for assessing people’s social circumstances, including their assets and needs. In a pilot involving 80 patients who’ve visited Saint Francis Healthcare for a maternal-fetal medicine consult, finding safe housing, having reliable transportation, and paying utility bills have emerged as the greatest needs. RMOMS grant funding is being used to hire a new staff member based at Saint Francis. Known as a system care coordinator, the staffer will provide education and resources to pregnant people; make connections across programs; and use survey results to identify gaps in services.
Members of the Bootheel collaborative are also educating emergency department clinicians and paramedics on how to handle obstetric emergencies, including deliveries in ambulances. Participants complete online modules then go through hands-on simulations. Grantees are setting up a satellite OB clinic in a county health department, where a sonographer and nurse will partner with hospital-based OBs or other specialists.
In Missouri, members of the Bootheel Perinatal Network are educating paramedics how to handle emergency situations that may arise during pregnancy, including deliveries in ambulances.
Both ROAMS and the Bootheel Perinatal Network are leveraging telemedicine to bridge the divide between rural maternity care providers and urban specialists. Having support from specialists can help providers in rural communities feel less isolated and gain comfort in handling patients with more complicated conditions. Across the U.S., interest in telematernity platforms and virtual visits has increased as a means of protecting patients and providers during the pandemic — drawing attention from payers and venture capitalists. But use of these tools is more established in rural communities that innovated out of necessity and turned to philanthropy and Medicaid programs for support.
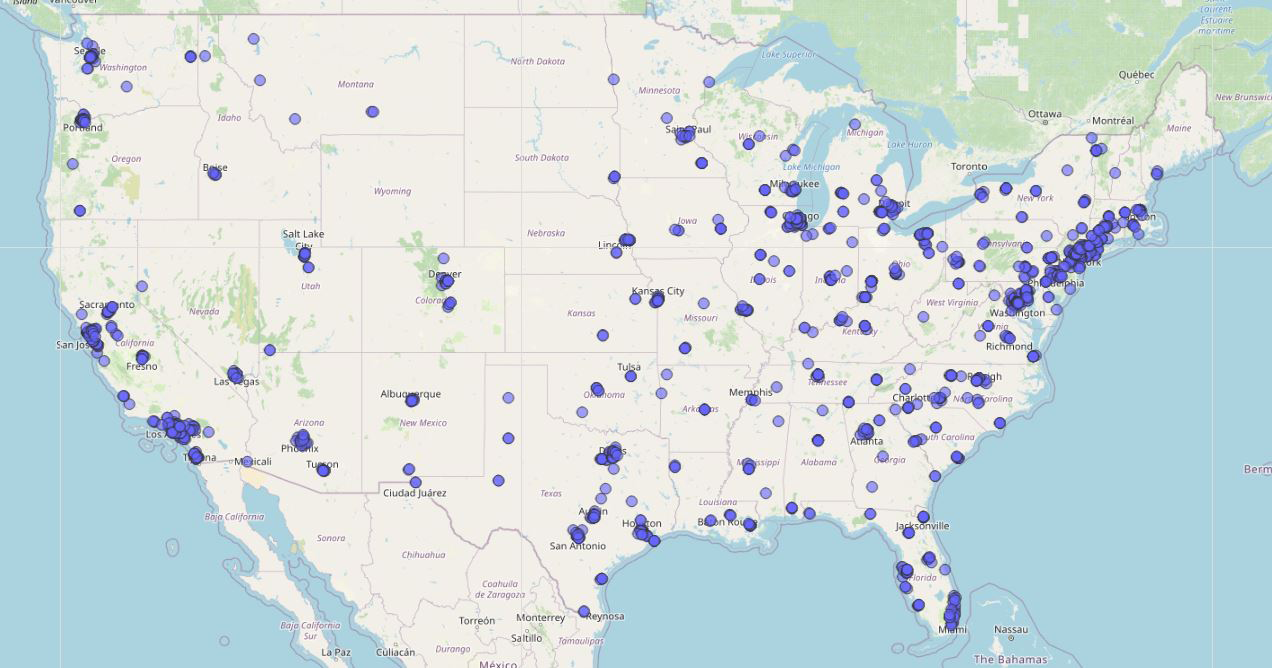
The U.S. has 1,800 maternal-fetal medicine specialists; most practice in urban areas. Several telehealth companies have been founded to extend services to rural areas. One is Access Physicians, which provides acute care subspecialty telemedicine services, including maternal-fetal telemedicine, to over 250 critical access hospitals. Image courtesy of Sina Haeri, M.D., vice president of women and children's health and chief of maternal-fetal medicine at Access Physicians.
High-Risk Pregnancy Telemedicine Programs
One of the earliest maternity telemedicine programs was created in 2003 by theUniversity of Arkansas for Medical Sciences (UAMS) and the state’s Medicaid agency in an effort to improve care for people with high-risk pregnancies. These include people who’ve had prior complications, such as preterm labor; those carrying two or more babies; and those who have conditions such as high blood pressure, diabetes, or obesity that can complicate pregnancy.
As part of the program, maternal-fetal medicine specialists from UAMS provide video consultations, genetic counseling, and real-time, interactive ultrasounds to patients in a variety of rural (and some urban) sites, including hospitals, health departments, and clinics, using T1 lines that support high-speed internet. In the fiscal year ending June 2021, UAMS specialists offered 2,377 maternity telemedicine consults, which are covered by Medicaid. By offering these supports as well as continuing medical education, the program is building the capacity of rural maternity care providers to handle uncommon but high-acuity events, says Joseph Sanford, M.D., director of the UAMS Institute for Digital Health & Innovation. For example, they are hoping to train rural obstetric providers in new approaches UAMS obstetricians and trauma surgeons have developed to treat hemorrhage during deliveries — perhaps even offering real-time teleconsultation in the delivery room.
The academic medical center also maintains a 24/7 call center staffed by labor and delivery nurses, backed up by OB physicians and advanced practice nurses, who offer advice to obstetrical providers and their patients from across the state and help facilitate transports when needed. This approach increased the number of preterm deliveries that happen in facilities with neonatal intensive care units from 28 percent in 2001 to 55 percent in 2017.
In 2009, using a $1.8 million grant from the BlueCross BlueShield of Tennessee Foundation, David Adair, M.D., a maternal-fetal medicine specialist in Chattanooga’s Regional Obstetric Consultants practice, launched a telemedicine program for Tennessee and other Appalachian residents who experience high-risk conditions during pregnancy. The Solutions to Obstetrics in Rural Counties (STORC) program is based on UAMS’ telemedicine program but attempts to be as much “high-touch” as “high-tech,” according to Adair.
STORC sends advanced practice nurses and sonographers into 12 areas of Tennessee, Alabama, North Carolina, and Georgia where long distances over mountainous terrain make it hard to travel to see specialists. The STORC teams rent space in local OB providers’ offices, bringing along ultrasound equipment, Wi-Fi hotspots, and laptops for secure video conferencing. Depending on the circumstances, patients who receive the specialist consults can remain under the care of their local clinicians, can be co-managed by local clinicians and the remotely located specialists, or in the most complex cases can be shifted to specialists’ care.
Among 10,000 people treated by STORC providers since the program’s inception, nearly all (91%) have been able to deliver at the closest rural hospital, according to Adair. “These local rural hospitals are struggling. If we can help them keep appropriate business there, that helps them on their margin,” he says. “It also helps patients, who don’t have to spend money on gas or lose wages for the day to attend appointments.”
The structure of the arrangement also helps allay concerns among rural providers that their urban counterparts are there to poach patients. Under most maternity payment bundles, the majority of a clinician’s payment for maternity care and all of a hospital’s payment comes from providing delivery services, so transferring a patient before then means a significant loss of revenue.
Pregnancy Care ECHO
The University of Utah Health is also engaged in efforts to educate rural maternity care providers in best practices for treating people with high-risk pregnancies. In 2015, staff there created the nation’s only Pregnancy Care ECHO (Extension for Community Healthcare Outcomes), offering biweekly videoconferences focused on topics suggested by university clinicians or participants. Sessions have focused on hypertension, substance use, hyperthyroidism, and gestational diabetes, among other topics. Over the past year, they’ve attracted nearly 600 people, including advanced practice clinicians, family physicians, obstetricians, and both hospital- and community-based midwives. “It has allowed us to bridge into the out-of-hospital birth world,” says Linda Sossenheimer, R.N., clinical educator outreach nurse at University of Utah Health.
Unlike some other ECHO programs, Utah’s does not rely heavily on participants submitting cases from their own practice for discussion. “It can be intimidating,” says Erin Clark, M.D., associate professor and division director of maternal-fetal medicine at the University of Utah Health. “A lot of rural providers may not have time to prepare cases. We want to meet them where they are instead of having our success dependent upon case submission.”
Expanding the Rural Maternity Workforce
Not only are there shortages of OBs and maternal-fetal medicine specialists in rural communities, but fewer family physicians are providing any obstetric care. Federal programs that offer tuition reimbursement for health care professionals who practice in rural areas have not moved the needle.
Preparing Rural Nurses
John Cullen, M.D., family physician in Valdez, Alaska with a newborn baby
Leaders in the field including John Cullen, M.D., a board member of the American Academy of Family Practice and a family physician in Valdez, Alaska, have called for the development of training programs for rural nurses. Cullen helps delivers some 50 babies a year at the 10-bed Providence Valdez Medical Center, which is a six-hour drive from Anchorage and covers a service area the size of Ohio. Given that bad weather can make it impossible to transfer patients to Anchorage, Cullen and his colleagues prepare to handle urgent situations. Newly hired nurses undergo a bootcamp on procedures for cesarean sections and neonatal resuscitation, for example, and Cullen and Providence’s three other family physicians and 12 nurses cross-train so all teams can deliver babies, handle emergencies, and take care of hospitalized patients.
Cullen says a rural nursing designation could offer this kind of broad and deep training. “Our nurses have all the certifications, everything from pediatric acute life support to emergency nursing to ICU nursing to neonatal resuscitation and OBGYN,” he says. “And so there really needs to be a specialty designation that recognizes that level of competence and commitment, and the nurses need to be paid on a level that rewards the value they bring.”
Even if a community is not planning on providing maternity care, they still are going to be providing maternity care, but they won’t be ready for obstetrical emergencies.
John Cullen, M.D.
Family physician in Valdez, Alaska
Frontier Nursing University, based in Versailles, Kentucky, has a long history of training nurses to practice in rural areas. Its roots go back to the Frontier Nursing Service, which was founded in 1925 and sent nurse midwives, some on horseback, to provide care in isolated communities in the Appalachian region of Kentucky. Well before the pandemic, the university followed a distance-learning model that allowed nurses living in rural and underserved communities to become nurse midwives. Today the student body of 2,500 includes both nurse midwives and nurse practitioners from every state, including some of the most remote areas of the country. While most instruction is virtual, students come together in Kentucky for team training and simulation exercises. Nearly half of the students live in areas declared health professional shortage areas by the Health Resources and Services Administration (HRSA) and 20 percent also live in rural areas; the majority of graduates remain in their communities to provide care.
Beginning in the 1920s, nurse midwives, some traveling by horseback, began providing care to families in isolated communities in the Appalachian region of Kentucky. Photo courtesy of Frontier Nursing University.
Over the past decade, leaders have made a deliberate effort to train more nurses and midwives of color to promote racially concordant care. “Providing education in an equitable and inclusive environment is critical to the goal of improving health outcomes,” says Susan Stone, D.N.Sc., C.N.M., Frontier’s president.
Aided by grants from HRSA, Frontier has used scholarships and targeted recruitment (e.g., attending conferences of the Black or Hispanic nurses’ associations to encourage nurses to pursue advanced degrees) to attract more students of color. The school has also adopted new admissions criteria to ensure inclusion of minority and rural students. To make students of color feel welcome, staff offer mentoring, online forums, tutoring, and support from the Office of Diversity and Inclusion. The number of Frontier students of color increased from 9 percent in 2010 to nearly 28 percent in 2020, when Frontier graduated 208 nurses of color, including 57 nurse-midwives and 151 nurse practitioners.
Can Centering Pregnancy Work in Rural America?
The Centering Pregnancy model of group prenatal care, in which pregnant people come together to receive prenatal services and learn from clinicians and each other, has been linked to increased breastfeeding rates, greater patient and clinician satisfaction, and increased parental knowledge of childbirth and child-rearing. Observational studies have also connected it to reductions in preterm births, NICU admissions, and emergency department use during pregnancy. Some evidence suggests that the model can be particularly helpful for people of color and those with low incomes.
The model can be hard to implement in rural communities, given the problem of small numbers, even though group visits might help rural maternity care providers stretch their resources and spend more time with patients. Rebecca Pfaff, M.D. — a family medicine physician who delivers about 40 babies a year at Forks Community Hospital, a critical access hospital in Forks, Washington — recently started three Centering groups. Forks is an isolated region of timber forests and lakes in the extreme northwestern edge of the continental U.S.; the hospital serves some 10,000 people in a catchment area 50 miles across.
One Centering group is for women of the Makah Tribe; their reservation has an Indian Health Center offering urgent obstetric care but no prenatal services. Another group serves Mam women, an indigenous group from Guatemala who’ve come to the region to pick salal, a native shrub used in floral arrangements. Many Mam women speak only Mam, a Mayan language that is mostly oral, and are unable to read or write in any language. There is also a group open to all members of the community.
Rebecca Pfaff, M.D., a family medicine physician who delivers some 40 babies a year in Forks, Washington, began offering Centering group prenatal visits to Mam women, an indigenous group from Guatemala that has immigrated to Washington State. Photo: Ulf Huebner / Alamy Stock Photo
Leveraging funds from a state department of health grant from the Birth Equity Project, Pfaff received training and materials from the Centering Healthcare Institute to start the Centering groups. While the groups were disrupted by the pandemic, the Mam and community groups have restarted, typically attracting four to seven women for each visit. Pfaff plans to restart the Makah group this fall, when the tribe reopens its reservation to visitors.
Pfaff has adapted her approach along the way. She now hires a translator who offers Mam translation via audio conference; previously, she’d spoken Spanish and women who could speak the language would translate to Mam-only speakers, but information often got lost. “Having the right translation unlocked these really intelligent and interesting women,” Pfaff says. She’s also adapted the curriculum to rely less on written materials and include basic information about women’s anatomy and how birth control works. She’s been able to talk through induction, pain medicine, and other decisions that can be hard to discuss while in labor and without the benefit of translation or basic health literacy.
Pfaff plans to continue to offer Centering after the grant runs out because it’s cost effective, even after paying for translation, and appears to be helping her break down barriers and empower patients.
Enlisting Nonclinical Partners
In some communities, rural maternity providers are enlisting nonclinical partners. In Forks, funds from the Birth Equity Project will be used to train members of the Makah and other local American Indian tribes to work as doulas, lay people who provide emotional and practical support during pregnancy, childbirth, and the postpartum period. Medicaid agencies in at least five states (Indiana, Minnesota, New Jersey, New York, and Oregon) pay for doula services. A study led by Katy B. Kozhimannil, Ph.D., M.P.A., found that Medicaid beneficiaries who received doula support had lower rates of cesarean sections and preterm births, compared with other pregnant women enrolled in Medicaid.
Leaders of the Don’t Quit the Quit program run by the University of North Dakota are training tribal and other community members to work as postpartum doulas to support pregnant and parenting women who are in recovery from opioid use disorder. Leaders are also educating staff at Women, Infants, and Children (WIC) offices about substance use disorder and local treatment options. “One of our WIC counselors said, ‘I never believed that I needed this information,’” says Maridee Shogren, C.N.M., a practicing nurse midwife and clinical professor at the University of North Dakota in Grand Forks. “And then she had her first client who disclosed her substance use disorder. She hadn’t told anybody else. But because she had a rapport with her WIC counselor, she disclosed, and the counselor was able to ask a few basic questions and refer her to a local treatment provider.”
Training Rural Obstetricians
In 2018, the University of Wisconsin at Madison Department of Obstetrics and Gynecology created the nation’s first rural obstetrics and gynecology residency. From 1996 to 2016, the number of rural Wisconsin counties offering OB services dropped by half (from 40 percent to 20 percent). “Stemming the tide of hospital obstetric closures will require payment and policy changes,” says Ryan Spencer, M.D., the university’s obstetrics and gynecology (OB/GYN) residency program director. But giving OB/GYN residents an opportunity to gain confidence in working in rural environments can also be part of rebuilding services, he says. These residents spend about six months rotating through rural community hospitals and the rest of their residency in Madison, where they gain experience in handling rare but high-risk events that arise in a facility that delivers 5,000 babies a year. Last year, there were 200 applications for the one rural residency position — evidence of high interest in the program.
While young physicians may worry about being far from specialists and the support of a major institution, “all the residents have said working in rural facilities is not as scary as they thought it would be,” says Spencer. They’ve also been surprised by the variety and complexity of what rural providers handle. “They’ll say, ‘They do way more out there than I thought they did,’” he says. The residency program is being replicated at the University of Iowa, and leaders from other academic medical centers have expressed interest.
Policy Implications
Regional collaborations among maternity providers appear to be a promising way to bolster services for pregnant and parenting people in rural communities. Partners in these efforts are learning how to create the infrastructure — and trust — needed to work together. While the RMOMS grants last only four years, federal policymakers envision them as a proof of concept and plan to replicate the program if results are promising.
The following policies would support efforts to create regional networks of maternity care.
Creating equitable telemedicine policies. The pandemic-era lifting of restrictions for how and when telemedicine platforms can be used appears to have made maternity care more accessible for more people.It will be important for payers to learn from what has worked, such as paying for audio-only visits so those without broadband access can still participate. Lifting requirements for people to have in-person visits before teleconsultations would also expand access. Startup funds may also be needed to enable providers to invest in and maintain technology platforms.
Expanding Medicaid coverage. Research has shown that in states that have expanded eligibility for their Medicaid programs, women of childbearing age have better access to preventive care and fewer adverse health outcomes before, during, and after pregnancies. In the 12 statesthat have not expanded eligibility, many people lose Medicaid coverage just 60 days after giving birth. The American Rescue Plan Act creates a streamlined pathway for states to extend Medicaid coverage for one year postpartum, making sure people continue to have oversight and care.
In addition to expanding access to Medicaid, it is important to ensure Medicaid reimbursements for maternity care are adequate. On average, Medicaid pays just half of what commercial insurers do for deliveries, making it hard for rural hospitals to cover their fixed costs with relatively few deliveries. Because rural hospitals are more dependent on Medicaid than their urban counterparts, they are unable to offset losses with higher reimbursements from commercial health plans.
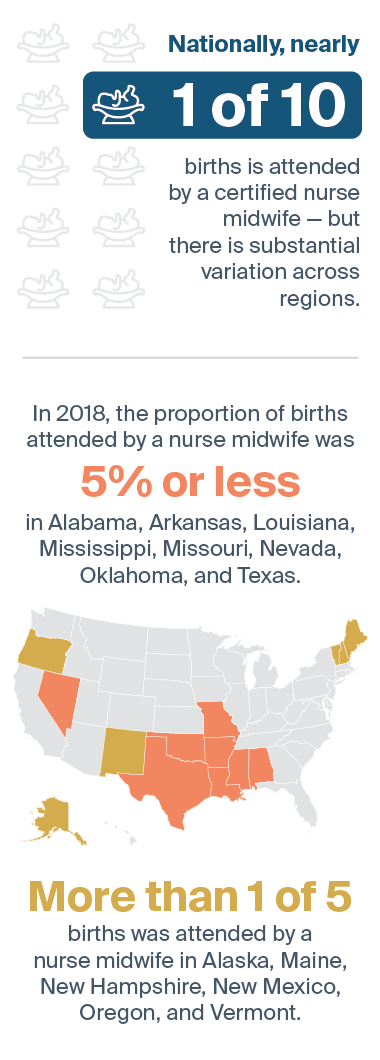
Source: National Center for Health Statistics, final natality data, 2018.
Investing in nurse midwives. Nurse midwives could help fill the gaps in rural communities, reduce overreliance on medical interventions, and bring down costs. One study found that states such as Washington that have done a better job of integrating midwives into maternity care tend to have better outcomes for parents and babies. But there remain significant payment and licensure barriers hindering midwives from offering services, particularly in states where more Black babies are born. Expanding the scope of practice for nurse midwives could grow this workforce. Efforts are also needed to encourage partnerships among nurse midwives and physicians to create a continuum of care for pregnant people with differing risks and needs.
Investing in nonmedical services. Medicaid programs could consider paying for low-cost, nonclinical services that could yield substantial returns for rural communities. These could include rides to clinics, doula services, navigation, and other services that can create a continuum of support for pregnant and parenting people before, during, and after childbirth.
Value-based payment models from Medicaid and other payers should take wraparound services into account and reward the efforts of community-based organizations, says Sue Kendig, J.D., W.H.N.P.-B.C., who serves as a technical consultant to Missouri’s Bootheel Perinatal Network. “You cannot make sure screenings are done, make sure people get into care, and help them transition through the perinatal continuum to well-woman care unless you rely on community partners,” she says. “It is important to identify payment mechanisms beyond grants that include reimbursement for these essential services.”
Q&A: Promoting Equity in Rural Maternity Care
Katy Backes Kozhimannil, Ph.D., M.P.A.
Katy Backes Kozhimannil, Ph.D., M.P.A., a professor of health policy and management at the University of Minnesota’s School of Public Health and director of the University of Minnesota Rural Health Center, researches the effects of rural hospital closures on maternal health outcomes. In a 2018 Health Affairs commentary, Reversing the Rise in Maternal Mortality, she described the event that sparked her interest in maternal mortality: learning that her grandmother’s sister died from a pulmonary embolism after giving birth. Her great aunt left behind five children who were adopted out of the family, a trauma that reverberated over generations. Transforming Care asked Kozhimannil what policy changes are needed to increase access to care in rural communities like the one her family hails from.
Transforming Care: Your research has found that rural counties with higher percentages of Black people of reproductive age were more likely to lose obstetric services than other rural counties. What prompted you to look at the intersection of race and rurality?
Kozhimannil:We started looking at rural obstetric unit closures after a group of Black grandmothers in Alabama raised concerns that local hospitals were no longer offering maternity care. They were troubled that their daughters had no place to give birth and went to their legislator, Congresswoman Terri Sewell, to ask why all the hospitals around them seem to be either closing or closing their birth units. They were having to take care of their grandchildren while their daughters were traveling long distances to give birth. They asked a very good question, and we had the opportunity to answer it through our work.
Transforming Care: What did you learn from research about the causes of the closures and what would you like to see done to address racial equity in maternity care, particularly in rural areas?
Kozhimannil: There are so many different systems coming together to create a situation where Black women living in rural communities are losing access to basic maternity services. I think it’s structural racism in all its facets — from lack of investment in economic development and housing to food insecurity and health care. As an example, Medicaid covers the majority of births in rural communities and among Black women but pays less than what commercial insurers pay, making it hard for hospitals to remain open and for women to find obstetric providers. In designing solutions, we have to be careful that we are not simply increasing access to a system that harms people by perpetuating racism. That is, we need to institute antiracist policies that improve health by dismantling racism in health at both interpersonal and structural levels.
Transforming Care: What would you change about the way we measure the quality of maternity care in the U.S.? What problems are being missed?
Kozhimannil: We need to go well beyond maternal mortality and include things that matter to people giving birth. Right now, we have very few measures of quality of care or quality of life, especially in the postpartum period. We need to assess whether people are getting information in culturally relevant ways, whether they are treated with dignity and respect, and whether they have autonomy in decision-making, among other things. The people who should be directing the research and policy questions we investigate are the people in the communities who are most affected by poor maternal health outcomes. They know the questions to ask. We have found in a lot of rural communities, both patients and providers are so consumed with logistics of managing poverty and distance to care — how to get to appointments if you don’t have a reliable vehicle, childcare, or money for gas, for instance — that they don’t always have time to discuss risk factors and issues like domestic violence. Half of all maternal deaths are not from obstetric causes. The single most common non-obstetric cause is violence. So, we’re losing moms because they're being killed — often by their partners. Making matters worse, there are limited resources for people experiencing domestic violence in rural communities, much less for those who speak other languages.
Transforming Care: In your Health Affairs article, you call for a national maternal mortality review committee, noting that the problem of small numbers in some state maternal mortality review committees has prevented the data from being useful. How would it help to have rural providers on these committees?
Kozhimannil: You need different voices at the table — not just clinicians or medical people but birth workers broadly and people who are survivors of a near miss of maternal morbidity; family members who have lost someone; and importantly, Black and Indigenous people of color. It would also really help to have people who are immigrants or who are non-native English speaking. Rural representation is also extremely important because health care is different in rural places. When we did research on state maternal mortality review committees, we found only two states require rural representation. And yet we know rural folks die at higher rates. In addition to having more diverse representation on maternal mortality review committees, we need greater and more consistent access to information about the moms we lose. The way these committees get information is highly variable — most comes from clinical records that don’t include information on social risks that we need to have to understand what happened. We also need to give maternal mortality review committees some teeth to be able to enforce some of the recommendations they make and share data with researchers.
Transforming Care: Would increasing Medicaid reimbursement based on social risk factors help shore up the delivery system in rural communities?
Kozhimannil: Medicaid is so important, and a great tool, but as a public health insurance program it can’t do everything to remake the social safety net for this country. I don’t think the onus can fall only on Medicaid especially as an entitlement program that is politically vulnerable to changes that state legislatures make. The state borders that surround you shouldn’t necessarily determine what care you can access during pregnancy and for how long you have insurance coverage postpartum. But Medicaid is absolutely a part of potential policy efforts to improve maternal health. It can be a building block to create a broader social insurance structure that supports people during pregnancy and parenting. For instance, we can make reimbursement in Medicaid and commercial insurance consistent so clinicians and health systems don’t discriminate based on type of insurance.
Transforming Care: Is the RMOMS model — providing federal grant funding to communities to form networks of maternity care providers and fill gaps in the continuum of services — a scalable approach?
Kozhimannil: I love RMOMS. It’s an investment by the federal government that grew out of the research questions raised by the grandmothers in Alabama. The demonstrations RMOMS has funded will give us information to improve the way we do things, but that is not, in and of itself, transformative. It’s an attempt to retrofit the existing system rather than transform it. I think we need to change the financial incentives and rules about where the money flows. The fee-for-service health care system is not well aligned with the goals of safe and healthy maternity care. For starters, we should be paying well for healthy births as opposed to paying more simply based on the intensity of procedure used during childbirth. We spend so much money on birth and we don't necessarily need more money. We need to spend it better.
Publications of Note
Hospital at Home Program Reduces Long-Term Care Use
Elderly patients in the United Kingdom who received hospital-level care at home along with a comprehensive geriatric assessment had similar outcomes as patients who received care in hospitals. The group receiving care at home also had fewer in admissions to long-term care facilities following the acute episode; researchers found 78.6 percent of the patients receiving care at home were still living at home after six months versus 75.3 percent of a comparison group. The researchers also found fewer patients receiving care at home had died (16.9% vs. 17.7%) within six months. Sasha Shepperd et al., “Is Comprehensive Geriatric Assessment Admission Avoidance Hospital at Home an Alternative to Hospital Admission for Older Persons?”Annals of Internal Medicine 174, no. 7 (July 2021):889–98.
Patient Navigation Services Reduce Readmissions for Patients with Substance Use Disorders
Hospitalized patients with comorbid substance use disorders (SUDs) who received patient navigation services at an academic medical center in Maryland were less likely to have an inpatient readmission within 30 days of discharge than patients who received treatment as usual (15.5% vs. 30%). They were also more likely to enter treatment for SUD after discharge (50.3% vs. 35.3%). The navigation program offered proactive case management, advocacy, and motivational support for three months following hospital discharge. Jan Gryczynski et al., “Preventing Hospital Readmission for Patients with Comorbid Substance Use Disorder,” Annals of Internal Medicine 174, no. 7 (July 2021):899–909.
Racial and Ethnic Differences in Self-Reported Health Status Largely Persisted Over the Last Two Decades
A study of U.S. adults found marked racial and ethnic differences in self-reported measures of health status, health care access, and affordability between 1999 and 2018. Black individuals with low incomes had the highest estimated prevalence of poor or fair health status (29.1% in 1999 vs. 24.9% in 2018), while white individuals with middle and high income levels had the lowest (6.4% in 1999 vs. 6.3% in 2018). The researchers, who relied on National Health Interview Survey data for 596,355 adults, found significant reductions in the racial and ethnic differences in some self-reported measures of health care access, but not affordability. Shiwani Mahajan et al., “Trends in Differences in Health Status and Health Care Access and Affordability by Race and Ethnicity in the United States, 1999–2018,” Journal of the American Medical Association 326, no. 7 (August 2021):637–48.
Health Care Spending Varies Widely by Race and Ethnicity
A study examining how health care spending varied by race and ethnicity in the U.S. from 2002 to 2016 found per-person spending was significantly greater for white individuals than all other population groups for ambulatory care. Per-person spending was significantly greater for Black individuals for emergency department (ED) and inpatient care, and for American Indian and Alaska Native individuals for ED care. Hispanic, Asian, Native Hawaiian, and Pacific Islander individuals had significantly lower per-person spending than the all-population mean. Total health care spending per person in 2016 was $7,649 for American Indian and Alaska Native individuals; $4,692 for Asian, Native Hawaiian, and Pacific Islander individuals; $7,361 for Black individuals; $6,025 for Hispanic individuals; $9,276 for individuals categorized as multiple races; and $8,141 for white individuals, who accounted for an estimated 72 percent of health care spending. Joseph L. Dieleman et al., “U.S. Health Care Spending by Race and Ethnicity, 2002–2016,” Journal of the American Medical Association 326, no. 7 (August 2021):649–59.
Promoting Equity Through Value-Based Payment
In a commentary in the Journal of the American Medical Association, Joshua M. Liao, Risa J. Lavizzo-Mourey, and Amol S. Navathe recommend that federal policymakers establish national pay-for-equity goals for the next decade to set expectations and direction for the health care industry. They also recommend revising legislation to incorporate equity into the evaluation of value-based payment models and consider the expansion of models that reduce disparities even if those models are found to increase spending. They also suggest convening a multistakeholder group of clinicians, insurers, and community and patient groups to guide the agenda for achieving equity goals. A National Goal to Advance Health Equity Through Value-Based Payment,” Journal of the American Medical Association 325, no. 24 (June 2021):2439–40.
Responding to Long COVID: Recommendations for Clinicians and Policymakers
In a commentary in the New England Journal of Medicine, Steven Phillips and Michelle A. Williams outline five steps the U.S. should take to address the needs of patients who continue to experience symptoms of COVID-19 weeks or months after becoming infected with the novel coronavirus. They include establishing a research agenda to identify the causes, mechanisms, and means of prevention and treatment of long COVID; drawing lessons from other post-infection syndromes, such as myalgic encephalomyelitis/chronic fatigue syndrome; expanding the use of multispecialty long COVID clinics; giving credence to patients who report symptoms; and, as a means of prevention, emphasizing the avoidable scourge of long COVID in vaccination campaigns. Steven Phillips and Michelle A. Williams, “Confronting Our Next National Health Disaster — Long-Haul Covid,” New England Journal of Medicine 385, no. 7 (August 2021):577–9.
The Challenges of Promoting Health Equity Through Medicaid
In a commentary in the New England Journal of Medicine, Sara Rosenbaum, an editorial advisor to Transforming Care, outlines four challenges President Biden will face in strengthening Medicaid, which now covers 76 million people, 60 percent of whom are Black, Latino, or members of other racial and ethnic minority groups. They include closing the Medicaid coverage gap in states that have elected not to expand their programs to more low-income adults; ending harmful experiments with Section 1115 waivers such as making coverage contingent on work; providing adequate funding to meet long-term care needs; and managing the end of the COVID-19 public emergency, which will put millions at risk of losing Medicaid coverage simultaneously. Rosenbaum suggests several possible solutions, including allowing low-income residents in nonexpansion states to enroll in fully subsidized marketplace plans and pursuing waiver experiments that simplify enrollment and address certain social determinants of health. Sara Rosenbaum, “Health Equity and Medicaid Transformation — Operationalizing President Biden’s Agenda,” New England Journal of Medicine 384, no. 25 (June 2021):2361–64.
Second Iteration of Medicare’s Bundled Payment Program Produces Modest Savings
Researchers found the Medicare Bundled Payments for Care Improvement–Advanced program, which was launched by the Center for Medicare and Medicaid Innovation in October 2018, was associated with small reductions in Medicare payments among participating hospitals. The savings were driven by reductions in spending at skilled nursing facilities. They also found that reductions in spending for postacute care and total spending were not associated with higher readmissions rates, nor did participating hospitals reduce the proportion of patients who were older or had more medically complex conditions. Participating hospitals had the option of selecting bundles for 29 inpatient and three outpatient episodes of care. Congestive heart failure was the most commonly selected condition, followed by sepsis, cardiac arrhythmia, pneumonia, and acute myocardial infarction. Karen E. Joynt Maddox et al., “Year 1 of the Bundled Payments for Care Improvement—Advanced Model,” New England Journal of Medicine 385, no. 7 (August 2021):618–27.
Utilization of Behavioral Health Services Lower Among Medicare ACO Populations
Researchers who assessed the impact of the Medicare Shared Savings Program (MSSP) on mental health and substance use services examined differences in utilization among two populations of patients attributed to accountable care organizations (ACOs): adults age 65 and older and those who qualified for Medicare due to disability. They found small reductions in outpatient mental health and substance use visits in the disability population and inadequate care of depression for both the disability and age-eligible populations. They also found increases in psychotropic medications among both groups of patients, as well as reductions in inpatient mental health stays. The number of hospital stays related to substance use among the disability population was also reduced. The researchers recommend adding more robust behavioral health quality measures to ACO contracts and monitoring disparities in care. Andrea Acevedo et al., “Impact of the Medicare Shared Savings Program on Utilization of Mental Health and Substance Use Services by Eligibility and Race/Ethnicity,” Health Services Research 56, no. 4 (August 2021):581–91.
Barriers to Ambulatory Care Contribute to ED Use for Medicare Beneficiaries with Disabilities
Researchers found Medicare beneficiaries with disabilities were 119 percent more likely to report difficulty accessing care and were 33 percent and 49 percent more likely not to have annual visits for primary and specialty care, respectively, than those without disabilities. Beneficiaries with disabilities also had higher likelihood of having all-cause (42%), nonemergent (67%), and preventable emergency department (77%) visits. Kenton J. Johnston, Hefei Wen, Karen E. Joynt Maddox, and Harold A. Pollack, “Ambulatory Care Access and Emergency Department Use for Medicare Beneficiaries with and Without Disabilities,” Health Affairs 40, no. 6 (June 2021):910–19
Mortality Rates During Pandemic Varied by Race, Occupation
Researchers found that groups exposed to greater economic or social disadvantage experienced large increases in all-cause mortality during the COVID-19 pandemic. The increases were greatest for adults living in correctional facilities or in health care–related group quarters; those without health insurance coverage; those with family incomes below the federal poverty level, and those in occupations with limited work-from-home options. For almost all subgroups, mortality increases were higher among non-Hispanic Black respondents than among non-Hispanic white respondents. Hispanic respondents with health insurance, those not living in group quarters, those with work-from-home options, and those in essential industries also experienced larger increases in mortality during the pandemic compared with non-Hispanic whites in those categories. Occupations that experienced the largest mortality increases were related to installation, maintenance, and repair and production. Sarah Miller, Laura R. Wherry, and Bhashkar Mazumder, “Estimated Mortality Increases During the COVID-19 Pandemic by Socioeconomic Status, Race, and Ethnicity,” Health Affairs 40, no. 8 (August 2021):1252–60.
Older, Poorer, and Sicker Americans Had Less Access to Telemedicine Prior to the Pandemic
Concerned that the COVID-19 pandemic would exacerbate disparities in access in health care services, researchers sought to establish patterns of telemedicine use prior to the pandemic. They found that while overall telemedicine uptake was low (0.12% of 846 million outpatient visits), there was even lower use among patients who were older, had more comorbidities, were in rural areas, and had lower median household incomes. Jashvant Poeran et al., “Pre-existing Disparities and Potential Implications for the Rapid Expansion of Telemedicine in Response to the Coronavirus Disease 2019 Pandemic,” Medical Care 59, no. 8 (August 2021):694–98.
Editorial Advisory Board
Special thanks to Editorial Advisory Board member Anne-Marie Audet for her help with this issue.
Jean Accius, Ph.D., senior vice president, AARP
Anne-Marie J. Audet, M.D., M.Sc., senior medical officer, The Quality Institute, United Hospital Fund
Eric Coleman, M.D., M.P.H., director, Care Transitions Program
Marshall Chin, M.D., M.P.H., professor of healthcare ethics, University of Chicago
Timothy Ferris, M.D., M.P.H., CEO of Massachusetts General Physician Organization and professor of medicine at Harvard Medical School
Don Goldmann, M.D., chief medical and scientific officer, Institute for Healthcare Improvement
Laura Gottlieb, M.D., M.P.H., assistant professor of family and community medicine, University of California, San Francisco, School of Medicine
Allison Hamblin, M.S.P.H., vice president for strategic planning, Center for Health Care Strategies
Thomas Hartman, vice president, IPRO
Clemens Hong, M.D., M.P.H., medical director of community health improvement, Los Angeles County Department of Health Services
Kathleen Nolan, M.P.H., regional vice president, Health Management Associates
J. Nwando Olayiwola, M.D., M.P.H., chief health equity officer and senior vice president, Humana
Harold Pincus, M.D., professor of psychiatry, Columbia University
Chris Queram, M.A., president and CEO, Wisconsin Collaborative for Healthcare Quality
Sara Rosenbaum, J.D., professor of health policy, George Washington University
Michael Rothman, Dr.P.H., executive director, Center for Care Innovations
Mark A. Zezza, Ph.D., director of policy and research, New York State Health Foundation
NOTES
The ROAMS, Rural Ob Access & Maternal Services, grant is funded by the Health Resources and Services Administration (HRSA), part of the U.S. Department of Health and Human Services (HHS). Please visit www.ROAMSnm.org for information on the grant and services provided. The ROAMS project is supported by the HRSA as part of a financial assistance award totaling $2,982,779, all funded by HRSA/HHS. The information was provided by ROAMS and does not necessarily represent the official views of, nor an endorsement, by HRSA/HHS, or the U.S. Government.
Publication Details
Date
Contact
Martha Hostetter, Consulting Writer and Editor, Pear Tree Communications
Martha Hostetter and Sarah Klein, “Restoring Access to Maternity Care in Rural America,” Transforming Care (newsletter), Commonwealth Fund, Sept. 30, 2021. https://doi.org/10.26099/CYCC-FF50