Our Scorecard ranks every state’s health care system based on how well it provides high-quality, accessible, and equitable health care. Read the report to see health care rankings by state.
Integrating Behavioral Health Services into Primary Care
How One Medicaid Managed Care Plan Made It Work
The sun sets along Main Street in Rangely, Colo. The state outperforms most others on several measures of health and wellness, but it has relatively high rates of suicide and deaths related to drugs and alcohol. To combat these high rates, Rocky Mountain Health Plans expanded access to behavioral health services for its Medicaid members. Photo: Helen H. Richardson/Denver Post via Getty Images
The sun sets along Main Street in Rangely, Colo. The state outperforms most others on several measures of health and wellness, but it has relatively high rates of suicide and deaths related to drugs and alcohol. To combat these high rates, Rocky Mountain Health Plans expanded access to behavioral health services for its Medicaid members. Photo: Helen H. Richardson/Denver Post via Getty Images
Toplines
Integrating behavioral health into primary care can make it easier to find treatment and reduce the stigma surrounding addiction and mental health issues
One managed care plan found a way to increase access to behavioral health services for Medicaid beneficiaries without increasing overall health spending
Toplines
Integrating behavioral health into primary care can make it easier to find treatment and reduce the stigma surrounding addiction and mental health issues
One managed care plan found a way to increase access to behavioral health services for Medicaid beneficiaries without increasing overall health spending
Advocates have long argued that integrating behavioral health services into primary care can increase access to treatment and reduce the stigma surrounding addiction and mental health issues. But there is little financial incentive to do so, and proponents face many administrative barriers. Among other challenges, payers often maintain separate provider networks with different billing practices for primary care and behavioral health services.
In this case study, we describe how Rocky Mountain Health Plans (RMHP) overcame these obstacles to expand access to behavioral health services for its Medicaid members. The managed care plan is a UnitedHealthcare subsidiary that serves Colorado’s Western Slope, including Medicare, Medicaid, and privately insured members. RMHP works with its network of contracted health care providers to strengthen their services. It also acts as the Regional Accountable Entity, tasked with coordinating Medicaid beneficiaries’ primary and behavioral care.
The health plan developed an alternative payment model for its contracted primary care practices to enable them to hire behavioral health staff and offer services such as routine screenings, brief interventions, ongoing therapy for mild to moderate conditions, and warm handoffs to therapists and other specialists. Launched in 2014 and expanded in 2018, this payment approach has increased the number of Medicaid beneficiaries receiving behavioral health services. The resulting reductions in the total cost of care offset the health plan’s upfront investments, which amount to roughly 0.04 percent of its total health care spending.
Our goal is to create an economic basis for whole-person health. Primary care is where most people access the health care system. It’s one of the few proactive spaces in health care. And it’s really the only place where people can develop comprehensive, decades-long relationships.
Patrick Gordon
CEO of Rocky Mountain Health Plans
Behavioral Health Challenges on the Western Slope
As tracked in the Commonwealth Fund’s Scorecard on State Health System Performance, Colorado outperforms most states on several measures of health and wellness, but it has relatively high rates of suicide and deaths related to drugs and alcohol. In 2022, the nonprofit Mental Health America ranked Colorado last among states on a composite measure that takes into account the prevalence of mental health conditions, substance use, suicidal ideation, and people’s access to treatment.
On Colorado’s mountainous Western Slope, many people struggle with what Jennifer McAtamney, executive director of Building Hope Summit County — a local nonprofit devoted to mental health — describes as the “paradise paradox.” “We are in this beautiful part of the Rocky Mountains; people think, ‘How could things be bad up there?’” she says. “The truth is, living in a rural resort area is very hard. People come here without their traditional support systems. It’s unusual for people to have extended family here. And our winters are really long.”
The region also has a shortage of therapists and other behavioral health providers, particularly those who accept Medicaid patients, and some of the nation’s highest costs for private health insurance. Until July 2018, the state paid organizations owned and controlled by community mental health centers to provide behavioral health services, and few independent behavioral health providers had a means of receiving payment to serve Medicaid patients. Patients reported long waits for treatment.
RMHP has sought to increase access to behavioral health services for its Medicaid members by using premium dollars from the state — which it receives as a Medicaid managed care plan — to provide upfront payments to primary care practices to hire staff, including licensed clinical social workers and psychologists. The health plan also provides technical assistance to practices to help them screen all patients for mental health and substance use disorders and adjust clinical workflows to respond to identified needs. RMHP also offers coaching and training on behavioral health topics and convenes providers to share best practices for protocols, such as deciding which behavioral health patients can be treated in house and which ones should be referred to specialists.
RMHP’s Payments to Support Advanced Primary Care
Rocky Mountain Health Plans’ efforts to help practices integrate behavioral health services are part of broader efforts to promote advanced primary care.
Step One
A primary care practice must be designated as tier 1 in the health plan’s medical home program. Tier 1 practices must:
be fully open to accepting Medicaid patients
meet benchmarks on performance measures (e.g., for depression screening and follow-up or initiation of treatment for substance use disorder) and take steps to improve their performance
provide patients with advanced access including after-hours and telehealth services
assess patients’ risks and develop care plans
earn designation as a patient-centered medical home by the National Committee for Quality Assurance.
Practices that achieve tier 1 status — which is reassessed annually — receive per member per month (PMPM) payments that offer a predictable cash flow, enabling them to invest in new care models.
Step Two
To support behavioral health integration, tier 1 practices are eligible to apply for a separate contract, known as a Community Integration Agreement.
The Community Integration Agreement helps practices hire behavioral health staff. The funding amount depends on the number of Medicaid members attributed to practices. It is usually between $75,000 and $200,000 per year. These funds supplement the other incentive payments RMHP gives tier 1 practices.
Patrick Gordon, RMHP CEO
RMHP is not prescriptive about the types of providers practices can hire or how they are deployed. Per RMHP CEO Patrick Gordon: “Instead of trying to calculate the particular costs for particular services or make benefit changes, we just decided to keep it simple and say, ‘What does it take to have a base level of behavioral health staff given the practice panel size.’”
Taken together, these payments increase Medicaid reimbursements by more than 60 percent, to a level significantly higher than a primary care provider would receive under the state’s fee-for-service program. The enhanced payments make up a relatively small portion of the health plan’s overall budget because primary care spending accounts for a small share of total spending. But the additional funds create a significant incentive for practices to expand efforts to provide whole-person, population-focused care. The number of practices that achieved tier 1 status increased from about 44 in 2018 to 63 in 2022. Together, these practices care for 60 percent of the health plan’s Medicaid members, up from 20 percent in 2018.
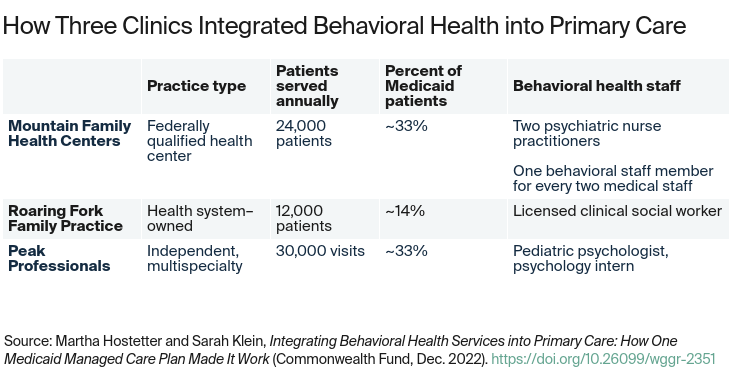
Mountain Family Health Centers
Mountain Family Health Centers is a federally qualified health center that serves 24,000 patients at four health centers and six school-based clinics. The communities Mountain Family serves near the ski towns of Vail and Aspen are ones of “extraordinary wealth and extraordinary poverty,” according to its CEO, Ross Brooks. More than 40 percent of the health center’s patients are uninsured because of the high numbers of undocumented immigrants in the community, and many people earn too much to qualify for Medicaid but can’t afford private coverage. About one-third of Mountain Family’s patients have Medicaid coverage (nearly all through RMHP), a small number (4%) have Medicare, and about 18 percent have private coverage.
Mountain Family negotiated its first Community Integration Agreement in 2013, as part of the pilot effort. RMHP initially provided $75,000 in grants and other funds to support community care coordination, which grew to more than $1 million annually to hire new behavioral health staff, support care transitions, and improve the health of the communities served by Mountain Family. It achieved tier 1 status in 2017. Mountain Family also participates in the state’s Payment Reform Initiative for Medicaid Enrollees (PRIME) initiative, enabling the health center to receive shared savings on top of other PMPM payments from RMHP.
The investments from RMHP and the PRIME program have enabled Mountain Family to substantially expand its behavioral health services. Ten years ago, the health center had one part-time behavioral health clinician; now, it has one behavioral health clinician (most are licensed clinical social workers) for each two medical providers. There are also two psychiatric nurse practitioners, and Brooks would like to hire more to meet demand for prescribers.
Mountain Family’s goal is to take care of people with mild to moderate behavioral health problems through brief interventions or therapy and refer people who need more intensive, ongoing therapy to the community mental health center or other specialists.
To assess patients’ needs, Mountain Family uses a risk-assessment tool that ingests data from medical records, the regional health information exchange, and a community platform that gathers information on residents’ social needs. All patients are also screened for depression at every visit. In a given year, about 20 percent of Mountain Family’s patients receive behavioral health services, most for anxiety or depression, and some for addiction, most commonly alcohol use disorder.
Roaring Fork Family Practice
Roaring Fork Family Practice is a tier 1 practice in Carbondale, Colorado, that is owned by the nonprofit Valley View Health Care system. Its six physicians and two nurse practitioners (some part time) serve 12,000 patients, about 14 percent of whom are covered by RMHP’s Medicaid plan, 5 percent are uninsured, and the rest are covered by Medicare or private insurance.
Like several other private practices in Colorado, Roaring Fork participated in the Comprehensive Primary Care Initiative, though which it benefitted from funding and coaching from RMHP; Medicare and private payers also participated in the initiative. “Rocky Mountain Health Plans was our teacher,” says Gary Knaus, M.D., former medical director of Roaring Fork and former board member of RMHP. “They had a whole staff of people who taught us how to provide advanced primary care.” In addition to the extra funds from the Community Integration Agreement, Roaring Fork receives care management fees and other incentives from value-based contracts, including Primary Care First.
The training and additional funding from these contracts enabled Roaring Fork to integrate behavioral health services into their work. Before each visit, all patients respond to a survey that asks questions about symptoms of anxiety, depression, loneliness, substance use, and other health risks. Providers then initiate conversations with patients who appear to have issues and offer to make a warm handoff to Jennifer Bouchet, the practice’s licensed clinical social worker. “If I’m able to, I will see patients immediately following their medical visit,” says Bouchet. “We talk through what’s happening. For something like anxiety, we talk through some skills right then. And then I ask patients what they’re looking for when they leave. For those who say they want counseling, my job becomes helping to bridge them to these resources.”
Bouchet says the COVID-19 pandemic unmasked a lot of trauma and grief among patients, and demand for behavioral health services has increased. It can be hard to find timely therapy appointments with private practitioners or at the community mental health center, particularly for patients with Medicaid coverage or those whose primary language is Spanish. In some cases, Bouchet offers ongoing counseling for patients who have trouble finding it elsewhere.
Peak Professionals
Peak Professionals operates multispecialty practices in Montrose and Gunnison, Colorado. They have grown since opening in 2015 by filling gaps in the market for primary care as well as psychology, chiropractic, urology, general surgery, and other services. Peak also offers a primary care subscription, which, for $39 a month, gives patients four visits a year and access to providers via telehealth and telephone.
RMHP helped Peak earn designation as a patient-centered medical home, enabling it to achieve tier 1 status in 2019. The practice provides about 30,000 visits a year. About one-third of patients are covered by Medicaid, mostly through RMHP, one-third are covered by Medicare, and the rest have private coverage, are uninsured, or buy Peak’s primary care subscription plan.
Joe Adragna, M.D., president and founder of Peak Professionals’ family medicine practice
Like Mountain Family and Roaring Fork, Peak’s practice is bolstered by support from Medicaid PRIME’s PMPM fees, enabling it to hire additional primary care providers, offer telehealth and remote monitoring programs, and other wraparound services. Still, PRIME on its own would not be sufficient to support behavioral health integration, according to Joe Adragna, M.D., president and founder of Peak’s family medicine practice: “That’s where Rocky’s Community Integration Agreement came in and took us to the next level.” The funds from RMHP allowed Peak to support an adult psychologist (who recently retired, and whom the practice is trying to replace), a pediatric psychologist, and a psychology intern.
All of Peak’s patients are screened at least once a year for depression, tobacco use, and alcohol overuse, and, if indicated, they will be screened for anxiety, illicit drug use, and other issues. Most patients receive brief interventions, medication management if indicated, and handoffs to therapists. According to Adragna, between the rising number of therapists in private practice, reduced wait times at the community mental health center, and the emergence of telehealth options, most patients can now find counseling appointments within a few days. Telehealth in particular has helped expand access for Medicaid patients, but they still face weeks-long waits for psychiatric evaluations — one of the reasons Peak is trying to recruit a psychiatrist.
RMHP’s Community Integration Agreement has enabled Peak to offer warm handoffs and other ad hoc behavioral health services that would not be possible within the traditional fee-for-service payment system, according to Adragna. “It gave us the flexibility to help whoever came through the door,” he says. “We used our psychologist for many things. Say somebody came in with a blood pressure that was really high. We’d have them spend 15 minutes with our psychologist, who would offer relaxation techniques. We’d recheck their blood pressure, and it would have come down 30 points. And now we don’t have to send that patient to the emergency department. The psychologist could also talk about medication compliance, adherence to low-sodium diets, and the need to monitor blood pressure for long-term control. It expanded much beyond just doing depression and anxiety and substance use. It actually helped us in other areas of primary care that we didn’t expect.”
We used our psychologist for many things. Say somebody came in with a blood pressure that was really high. We’d have them spend 15 minutes with our psychologist, who would offer relaxation techniques. We’d recheck their blood pressure, and it would have come down 30 points. And now we don’t have to send that patient to the emergency department.
Joe Adragna, M.D.
president and founder of Peak Professionals’ family medicine practice
Impacts of Integration on Access to Behavioral Health Care
RMHP’s use of Community Integration Agreements over the past decade has increased the number of primary care practices offering behavioral health services on the Western Slope. This has allowed providers to respond to greater demand during the pandemic: from January 2019 to September 2021, the number of members receiving behavioral health services outside of community mental health centers increased nearly 66 percent, while the average number of psychotherapy services billed across settings increased nearly 77 percent.
Depression screenings also increased dramatically. The percentage of patients age 12 and older who were screened for depression in primary care settings and, when appropriate, had a documented follow-up plan, increased to 68 percent in 2021, up from 4.2 percent in 2014.
The approach also appears to have reduced the total costs of care. Compared with non–tier 1 practices in RMHP’s network, tier 1 practices generated $9.9 million in savings over three years (fiscal years 2018–19, 2019–20, and 2020–21). While it is hard to discern how much of the savings are attributable to behavioral health integration and how much to other aspects of advanced primary care, the results of a demonstration of the model suggest integrated behavioral services can reduce overall medical spending.
In that demonstration, known as Sustaining Healthcare Across Integrated Primary Care Efforts, conducted from 2012 to 2014 by RMHP and its partners, three primary care practices received upfront payments based on the anticipated costs of hiring new behavioral health staff and providing routine screenings for issues such as substance use and depression. Another three practices served as controls, receiving the usual fee-for-service payments. An evaluation of this approach found that net cost savings of $1.08 million were achieved after 18 months for 9,042 Medicaid, Medicare, and dually eligible beneficiaries — primarily from reduced numbers of hospitalizations.
According to Benjamin Miller, Psy.D., past president of the Well Being Trust and one of the evaluators of the demonstration, the Community Integration Agreement is a unique and radically straightforward approach to behavioral health integration. “You set targets and you hold people accountable. You give them a budget that’s appropriate to achieve those targets. That’s it,” he says. “You can look around the country and not find anything quite like this.”
Lessons
Rocky Mountain Health Plans’ approach offers lessons for other health care payers and primary care practices as well as for state and federal policymakers.
Behavioral health integration helps normalize mental health and addiction treatment as part of routine primary care.
The practices that negotiated Community Integration Agreements offer varying levels of services, but all routinely screen patients for behavioral health needs and help them find support. Primary care providers have noticed improvements in the management of physical health conditions, too. “It is a common refrain I hear from our medical providers, ‘Thank God for behavioral health,’” says Brooks of Mountain Family.
To integrate behavioral health services, practices need more than funding.
Many of the clinicians in the tier 1 practices built their capacity to work in teams through participation in programs like the Comprehensive Primary Care Initiative or patient-centered medical home certification. And as noted above, RMHP provides coaching and technical assistance to help practices integrate behavioral health services.
“Practices need more than turning on billing codes for integrated behavioral health to work,” says David Mok-Lamme, B.A., vice president of data systems and strategy at RMHP. “RMHP’s clinical informaticists and coaches work with practices to identify, implement, monitor, and improve integrated behavioral health interventions, workflows, and innovations.”
Even with support, integrating behavioral health is a balancing act. Practices struggle to recruit their own behavioral health staff and find places to refer patients for ongoing care — particularly for Medicaid beneficiaries and/or Spanish-speaking patients. Leaders also struggle to allocate behavioral staff members’ time between scheduled appointments and open slots that are needed for ad hoc services.
Scaling behavioral integration will require investments from all health care payers — as well as solutions for the uninsured.
Tier 1 practices offer additional behavioral services to all patients, not just those who have Medicaid coverage, but this strains their capacity and limits what they’re able to do. And, of course, there are no value-based payments to cover uninsured patients.
In recognition of the work Mountain Family does to provide integrated care to uninsured patients and reduce unnecessary emergency department utilization, Aspen Valley Hospital, Pitkin County, and Eagle County give the health center a per member per month payment for each uninsured patient served in the health center’s Basalt location. Mountain Family is working to expand this model to other service areas in partnership with hospitals and local counties.
Knaus of Roaring Fork also suggests that hospitals have an incentive for helping the uninsured. By setting up programs that help pay for primary care and other services for the uninsured, hospitals can help prevent unnecessary admittance, which costs them millions of dollars in uncompensated care. “What if we turn those millions of dollars into a positive thing and we can keep people out of the hospital?”
Behavioral health integration may be gaining traction, thanks to Medicaid programs and new federal funding.
Medicaid is the nation’s largest payer for behavioral health services. In recent years, several states, including Arizona, Michigan, and New York, have been working to integrate primary care and behavioral health services for their Medicaid beneficiaries. Colorado, too, has published a blueprint for reform that called for behavioral health integration to expand access to care for all residents. A recent Bipartisan Policy Center report outlines several steps states can take to promote behavioral health integration through their contracts with Medicaid managed care organizations. The report calls for clearer definitions and measurement of what we mean by integration, training and technical assistance for primary care providers, and the use of telehealth platforms and other technology to support integration.
Colorado policymakers and other state leaders are looking to leverage the American Rescue Plan Act and other stimulus funding to implement these reforms. The Biden administration has also proposed doubling federal funding for behavioral health integration programs, and testing payment models that support an integrated approach to whole-person care.
Publication Details
Date
Contact
Martha Hostetter, Consulting Writer and Editor, Pear Tree Communications
Martha Hostetter and Sarah Klein, Integrating Behavioral Health Services into Primary Care: How One Medicaid Managed Care Plan Made It Work (Commonwealth Fund, Dec. 2022). https://doi.org/10.26099/wggr-2351