Abstract
- Issue: Enrollment in Medicare Advantage plans continues to increase rapidly. This has led to questions about which beneficiaries are enrolling in Medicare Advantage or in traditional Medicare and how their health care experiences compare.
- Goal: To assess the characteristics and experiences of beneficiaries in Medicare Advantage and traditional Medicare.
- Methods: Analysis of data from the 2018 Medicare Current Beneficiary Survey and the Commonwealth Fund 2021 International Health Policy Survey of Older Adults. Beneficiaries in Special Needs Plans (SNPs) were examined separately where sample sizes were sufficient.
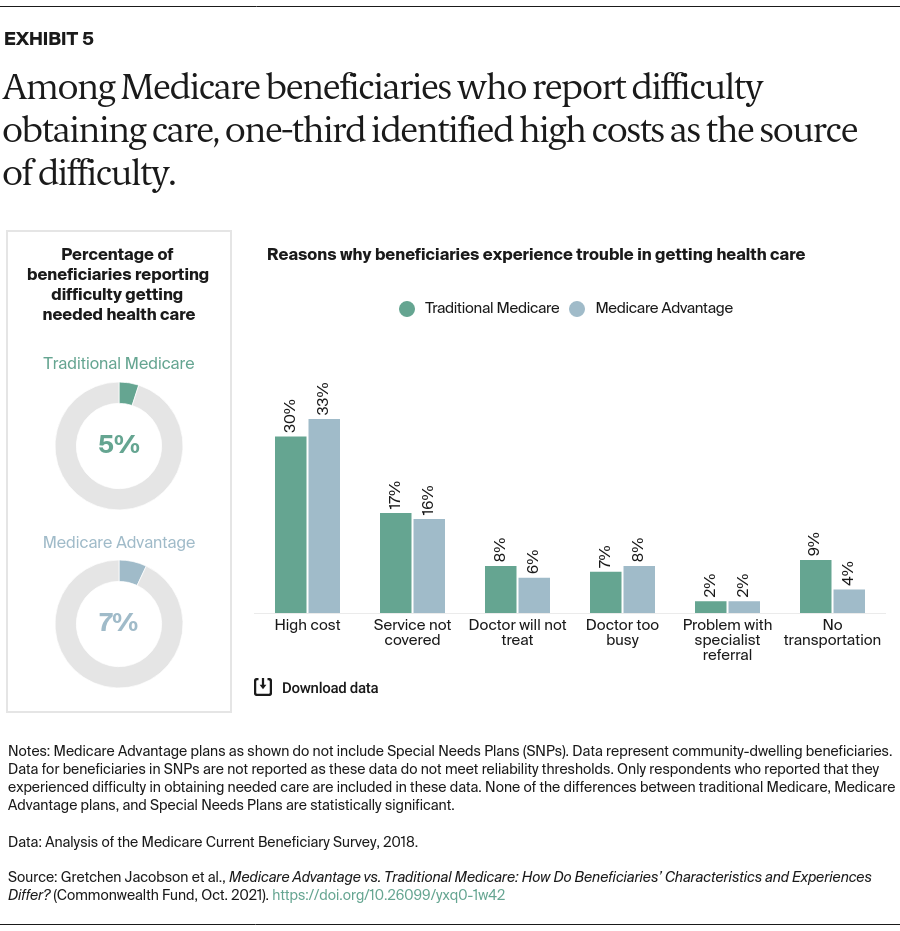
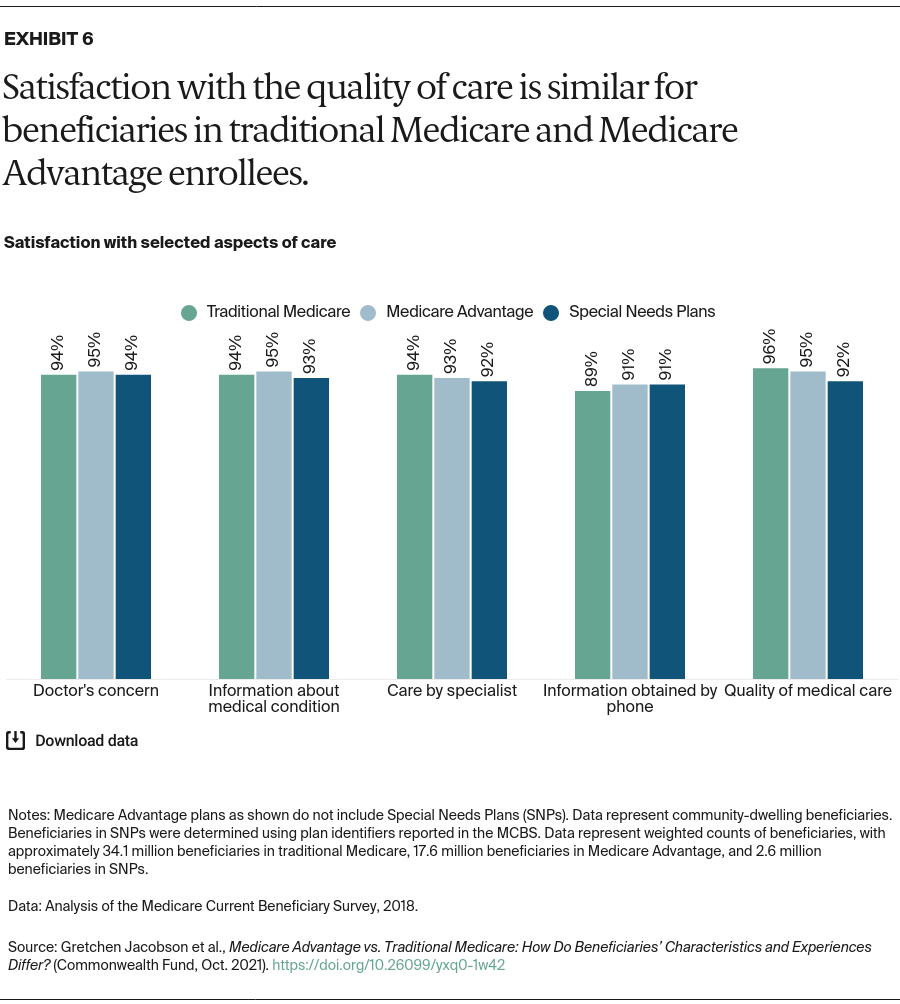
- Key Findings: Medicare Advantage enrollees do not differ significantly from beneficiaries in traditional Medicare in terms of their age, race, income, chronic conditions, satisfaction with care, or access to care, after excluding SNP enrollees. Both groups reported waiting more than a month for physician office visits. Similar shares of Medicare Advantage and traditional Medicare enrollees report that their out-of-pocket costs make it difficult to obtain care.
- Conclusions: Medicare Advantage and traditional Medicare are serving similar populations, with beneficiaries having comparable health care experiences. The care management services provided by Medicare Advantage plans appear to neither impede access to care nor reduce concerns about costs. Overall, the analysis highlights substantial barriers to care that all beneficiaries seem to be experiencing.
Introduction
Medicare beneficiaries can choose whether to receive their benefits from traditional Medicare or Medicare Advantage plans, which are offered by private insurers. These plans have experienced a surge in enrollment over the past decade, and half of beneficiaries are projected to be enrolled in a private Medicare Advantage plan by 2025.1 Medicare Advantage plans also have been paid more, on average, than what it costs to cover similar beneficiaries in traditional Medicare.2 As Medicare Advantage enrollment continues to grow, it is critical to examine the experiences of beneficiaries to ensure equity among beneficiaries and value for the Medicare program.
Traditional Medicare and Medicare Advantage: A Historic Divide
Beneficiaries weigh considerable trade-offs when deciding whether to enroll in Medicare Advantage plans or traditional Medicare. Unlike the latter, Medicare Advantage plans are required to place limits on enrollees’ out-of-pocket spending and to maintain provider networks.3 The plans also can provide benefits not covered by traditional Medicare, such as eyeglasses, fitness benefits, and hearing aids. Medicare Advantage plans are intended to manage and coordinate beneficiaries’ care. Some Medicare Advantage plans specialize in care for people with diabetes and other common chronic conditions, including Special Needs Plans (SNPs); SNPs also focus on people who are eligible for both Medicare and Medicaid and those who require an institutional level of care.
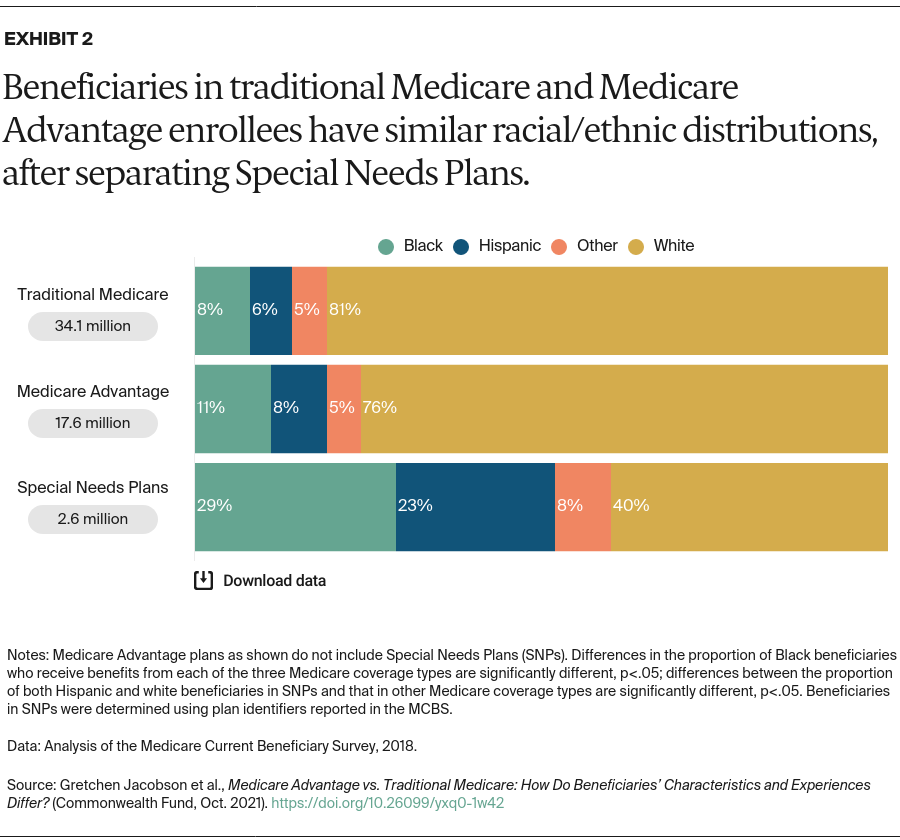
Traditional Medicare and Medicare Advantage enrollees have historically had different characteristics, with Medicare Advantage enrollees somewhat healthier.4 Black and Hispanic beneficiaries and those with lower incomes have tended to enroll in Medicare Advantage plans at higher rates than others.5 Traditional Medicare has historically performed better on beneficiary-reported metrics, such as provider access, ease of getting needed care, and overall care experience.6
This issue brief examines the characteristics and experiences of Medicare Advantage enrollees relative to beneficiaries in traditional Medicare, using the most recent available data from the 2018 Medicare Current Beneficiary Survey fielded by the Centers for Medicare and Medicaid Services. It examines SNPs separately from other Medicare Advantage plans when sample sizes are sufficient, with an eye toward understanding how the experiences of SNP populations differ from those of other beneficiaries. The analysis also includes data from the Commonwealth Fund 2021 International Health Policy Survey of Older Adults, which surveyed a sample of 1,609 individuals over age 65 in the U.S. between March and May of 2021.7
Findings
Beneficiaries Enrolled in Medicare Advantage and Traditional Medicare Look Similar, After Separating Out SNPs
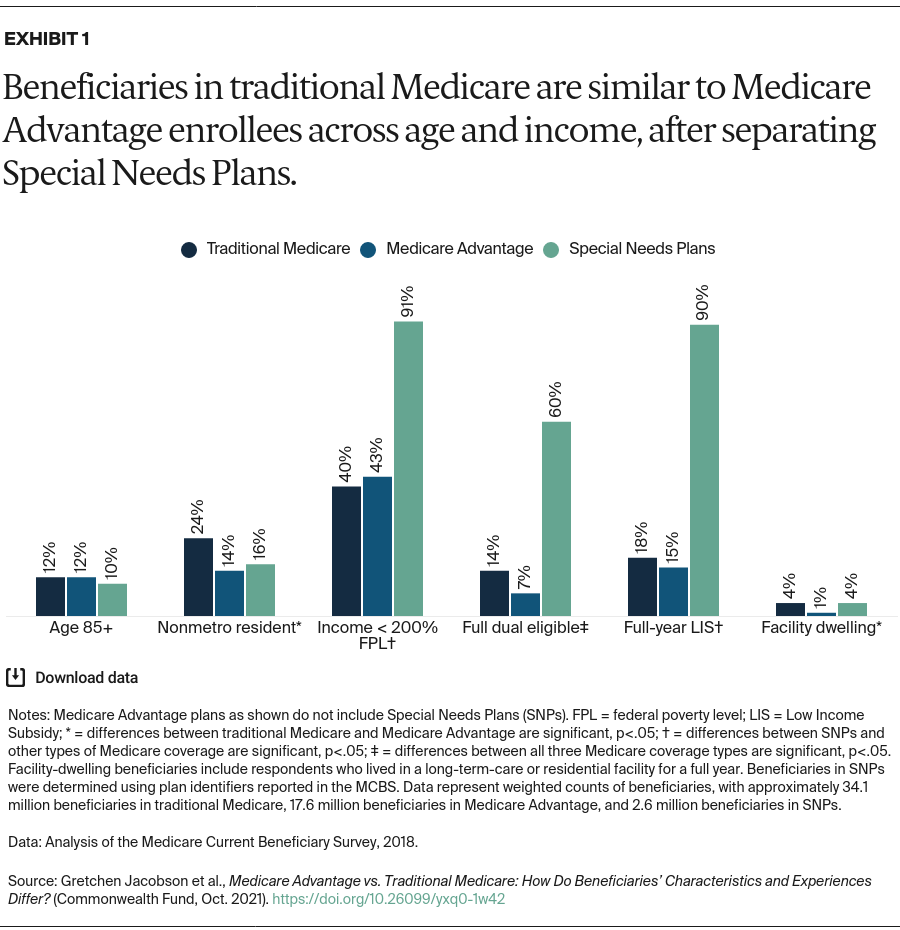
After excluding beneficiaries in SNPs, beneficiaries enrolled in traditional Medicare do not differ significantly from Medicare Advantage enrollees on age, income, or receipt of a Part D low-income subsidy (LIS), which helps low-income individuals pay for prescription drugs (Exhibit 1). However, beneficiaries in traditional Medicare are significantly more likely than Medicare Advantage enrollees to reside in a nonmetropolitan area, as well as more likely to live in a long-term-care or residential facility.
Beneficiaries in SNPs are different. Given the eligibility criteria for these plans, it is not surprising that enrollees tend to have significantly lower incomes and a greater likelihood of receiving Medicaid benefits or LIS than other Medicare beneficiaries. Enrollment in SNPs for people who require an institutional level of care has been growing rapidly, leading to a similar share of SNP enrollees and beneficiaries in traditional Medicare living in a long-term-care facility.8