In 2012, the United States Supreme Court ruled that the Affordable Care Act’s (ACA) Medicaid expansion was an unenforceable mandate. Currently, a dozen states have yet to expand. However, after a ruling by its state Supreme Court finding a voter initiative to establish expansion lawful, Missouri is now expected to join the expansion states. The federal government currently provides a 90/10 funding match to expansion states; the American Rescue Plan (ARP) will provide additional funding.
But for residents in states that have not expanded Medicaid, relief may come in the $3.5 trillion budget package that is expected to follow the infrastructure bill. A federally funded “fallback” option would extend help to millions but could take various forms. This post examines some of those options.
Federally administered Medicaid program for residents of nonexpansion states. Senators Raphael Warnock (D–Ga.), Jon Ossoff (D–Ga.), and Tammy Baldwin (D–Wis.) have introduced the Medicaid Saves Lives Act (MSLA). This would direct the Secretary of Health and Human Services (HHS) to establish a federally funded program for working-age adults who fall within the ACA Medicaid eligibility group (i.e., those with incomes up to 138 percent of the federal poverty level and not otherwise eligible for Medicaid) who live in states that have not expanded Medicaid. This would include the ACA expansion group. The bill also emphasizes that, consistent with the 2012 Supreme Court decision, it establishes no “state mandate.”
The bill dramatically expands the American Rescue Plan’s expansion bonus. The ARP created a new temporary (eight calendar quarters) sweetener for nonexpansion states, raising the federal share of their state Medicaid expenditures by a full 5 percentage points — for example, in a state with a federal match of 65 percent, the match would go to 70 percent during the temporary period. The MSLA would double this incentive, to 10 percentage points, while quintupling the temporary enhancement period to 40 calendar quarters. In addition to bonus payments, newly expanding states would receive the same permanent 90 percent enhanced federal matching rate for their expansion population that all expansion states receive.
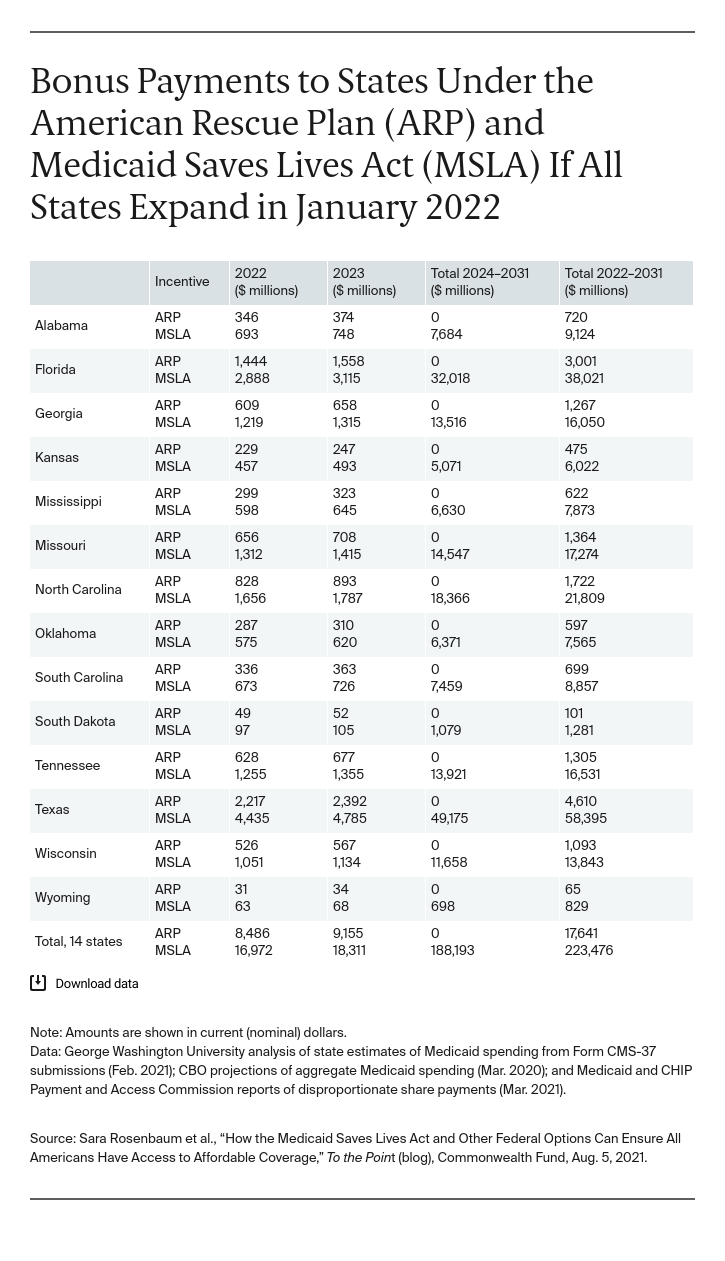
Our table shows how much states would gain under this increase, compared to the ARP, in federal Medicaid funding, beginning in January 2022. The ARP would invest $17.6 billion; under MSLA the investment would skyrocket to nearly $225 billion over the bonus period. If Texas expands, payments will rise from $4.6 billion under the ARP to $58 billion over the bonus period. Wisconsin’s potential bonus would increase from slightly less than $1.1 billion to nearly $14 billion. Payments to Georgia would rise to more than $16 billion compared to under $1.3 billion. Prior research found that the ARP expansion incentive, which would last for eight quarters, would exceed the 10 percent state share for the expansion population. It is thus safe to assume that the MSLA 40-quarter expansion bonus would dramatically exceed states’ costs.