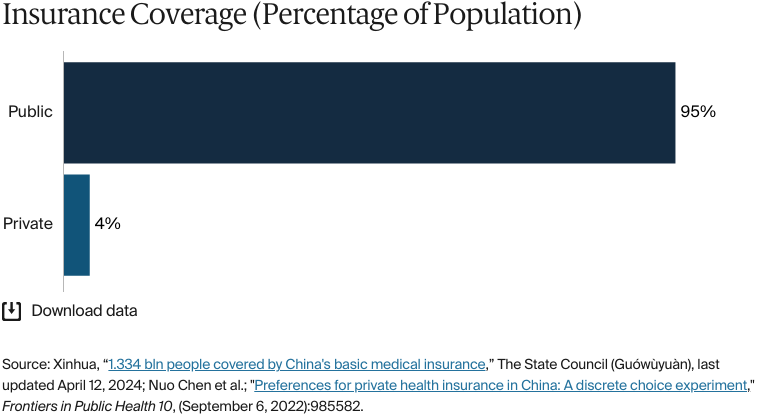
China’s health care system is publicly funded and built around a two-tier basic medical insurance program. The Urban Employee Basic Medical Insurance (Chéngzhèn Zhígōng Jīběn Yīliáo Boxin) is mandatory for formally employed urban workers and is funded through payroll taxes. Other residents are covered by the Urban and Rural Resident Basic Medical Insurance (Chéngxiāng jūmín jīběn yīliáo bǎoxiǎn), a voluntary program supported by government subsidies and individual contributions. Together, these two programs covered more than 95 percent of the population in 2023.
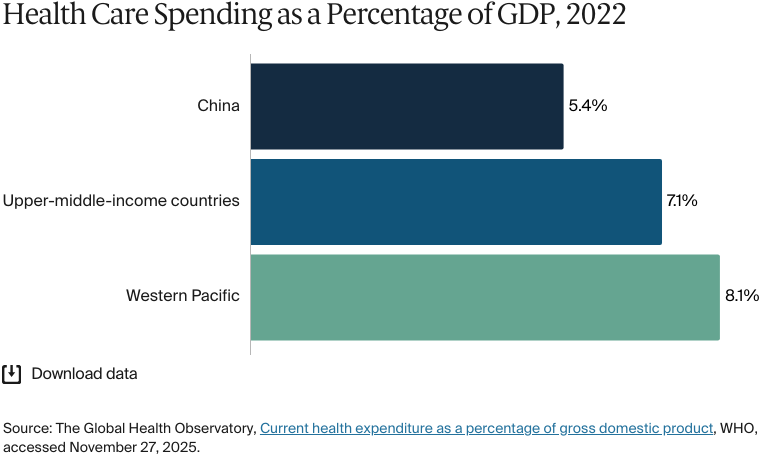
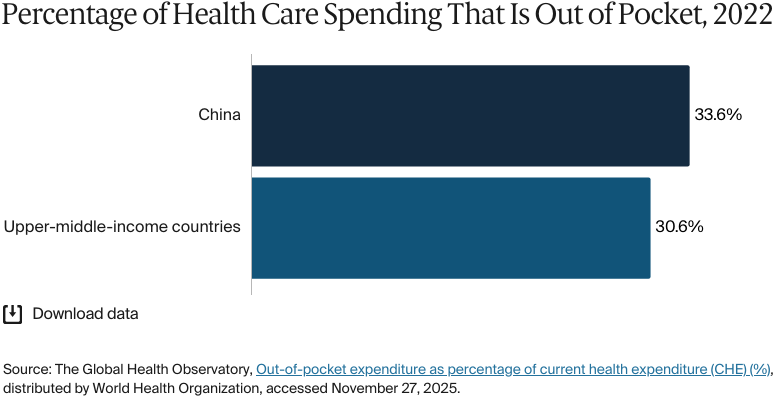
Although it provides near-universal coverage, the Chinese health system faces systemic challenges related to affordability, equity, and care coordination. Health spending is lower than in many other upper-middle-income countries, while out-of-pocket costs make up more than a third of total spending.
Health outcomes, such as life expectancy and infant and maternal mortality, and access to mental health services have improved significantly over the past two decades, though disparities between urban and rural areas persist.
In 2023, China’s basic medical insurance system, the Urban and Rural Resident Basic Medical Insurance, covered 1.3 billion people, including 371 million urban employees and 963 million rural and nonworking urban residents. Citizens and permanent residents are covered by both, but visitors and undocumented immigrants are excluded.
Public insurance coverage: 95% of population
Private insurance coverage: 4% of population
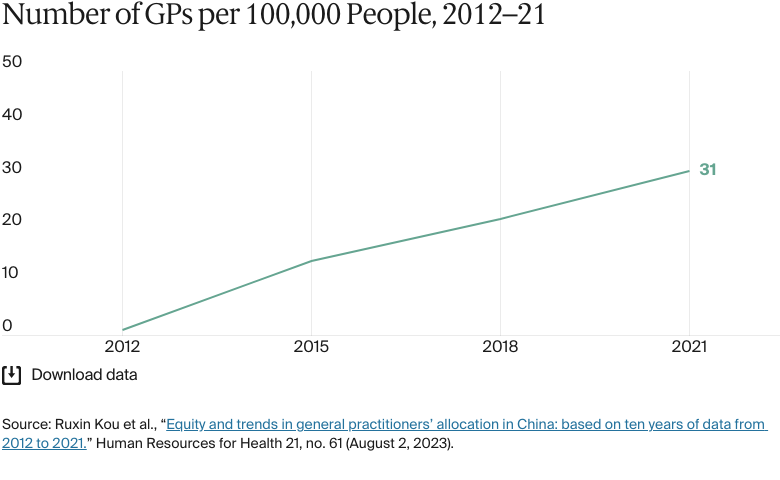
Primary care physicians: 39.9 per 100,000 people
Total health expenditure increased from CNY 85.3 trillion (USD 11.9 trillion) in 2022 to CNY 90.6 trillion (USD 12.6 trillion) in 2023. In 2023, social health spending was the largest source of health expenditure, at 46 percent. The next highest were out-of-pocket spending and government spending.
Pharmaceutical spending: 26.9% of total health care budget
Out of pocket spending: 32.2 of total health care spend
In 2021, life expectancy for urban populations exceeded that of rural populations by two years overall.
In areas with high proportions of ethnic minorities, such as Yunnan and Sichuan, use of maternal and child health services was found to be lower for minority women than for Han women, with disparities in terms of access to doctors and geographic accessibility to hospitals. In 2023, Chinese Han households in the region reported fewer deaths than Turkic households in the Xinjiang Uyghur Autonomous Region — one death for every 29 Han households compared with one death for every nine Turkic households.
The health care system has undergone several major transformations since the People’s Republic of China was founded in 1949.1 Between 1949 and 1979, the government built a centrally planned, publicly funded health system based on socialist principles that emphasized public ownership, prevention, and the integration of traditional and Western medicine. Despite its limited resources, the system achieved near-universal access and improved life expectancy, among other outcomes.2
With China’s shift toward a socialist market economy beginning in 1978, the government began to introduce market mechanisms into the health care system. Over the next three decades, this led to reduced government health spending, less focus on public health and rural areas, and excessive use of high-cost or unnecessary treatments.3 For example, the fee-for-service payment model that dominated during this period gave providers financial incentives to deliver more services (such as consultations or laboratory tests) regardless of need, driving up costs without necessarily improving outcomes.4 These changes contributed to rapid advances in medical technology and services but also created problems such as rising out-of-pocket costs, inequitable access, and a decline in public health services, particularly in rural areas (see Addressing Health Inequities).5
This situation left many people without health care coverage.6 By 1998, only 5 percent of the rural population and 38 percent of the urban population were covered.7 In response, the government introduced three insurance programs: the Urban Employee Basic Medical Insurance (UEBMI) in 1998 for public- and private-sector workers, the New Rural Cooperative Medical Scheme in 2003 for rural residents, and the Urban Resident Basic Medical Insurance in 2007 for urban residents without formal employment.8
In 2009, a major new phase of health reforms focused on five priorities: expanding health insurance coverage, improving access to essential medicines, strengthening primary care, enhancing public health services, and piloting hospital reforms.9 In 2016, the government merged the New Rural Cooperative Medical Scheme and the Urban Resident Basic Medical Insurance into one system: the Urban and Rural Resident Basic Medical Insurance (URRBMI).10
As of 2023, the basic medical insurance system (comprising the UEBMI and the URRBMI) (see The Role of Public Health Insurance) covered 1.3 billion people — more than 95 percent of the population — including 371 million urban employees and 963 million rural and nonworking urban residents.11 This marks a dramatic expansion from just 13.4 percent coverage in 2003.12
The Role of Public Health Insurance
China’s public health insurance is built around two programs:
The UEBMI is mandatory for urban employees and is funded jointly by employers and employees through payroll taxes.13
The URRBMI is a program that provides coverage for all rural residents and for urban residents who are not formally employed, such as children, students, the elderly, and unemployed residents. The program is voluntary (people are not automatically enrolled by the government).14
Together, the two programs form China’s basic medical insurance.15 Citizens and permanent residents are covered by both, but visitors and undocumented immigrants are excluded.16
The programs’ funding structures differ. Employers contribute monthly to the UEBMI, with the rates, which are set by local authorities, ranging from 7 to 10.5 percent, depending on location. For example, in Shanghai, employers contribute 10.5 percent; in Guangzhou, it’s 7 percent.17 Employees always contribute 2 percent, which is deducted directly from their salaries.18
The URRBMI is primarily supported by government subsidies, with insured people making relatively small fixed annual contributions. As of 2021, government funding covered about 67 percent of total yearly costs, with subsidies amounting to CNY 580 (USD 80.7) per person per year. The remaining yearly costs, CNY 320 (USD 44) per person, were covered by individual enrollees.19
Contributions are collected annually, and local governments have the authority to increase subsidy levels or adjust premiums based on local conditions. In Beijing, for instance, government subsidies covered up to 90 percent of the total premium for children and seniors in 2021.20
Services Covered by Public Health Insurance
The following services are covered under the basic medical insurance system:21
Inpatient care (partial coverage)
Outpatient care (partial coverage)
Primary care
Pharmaceuticals (only those included in the National Reimbursement Drug List)
Mental health care
Dental care (only for emergencies)
Eye care (partial coverage for certain inpatient procedures)
Rehabilitation (coverage for physical therapy)
Home visits (only in some cities through pilot programs)
Preventive services, such as immunizations, disease screening, and preventive traditional Chinese medicine, are included in a separate public health benefit package funded by central and local governments. Every resident is entitled to these services, which have no copayments or deductibles.22
Inpatient and outpatient care, including prescription drugs, are subject to different deductibles, copayments, and reimbursement ceilings depending on the insurance program, region, type of hospital (community, secondary, or tertiary), and other factors (see Cost Sharing and Out-of-Pocket Payments).23
Certain procedures such as cataract surgery are partially reimbursed, but no other eye care services are covered.24 Emergency dental services are covered, but routine care is paid out of pocket.25
The following services are not covered:
Maternity care
Palliative care
Long-term care.
Maternity care is covered by a separate insurance program, but in 2019 the government announced that it was going to be merged into the basic medical insurance.26 The aim is for the basic medical insurance program to provide the financial support needed to keep the maternity insurance fund sustainable amid the rising costs of policies aimed at encouraging childbirth. For instance, in 2019, the urban employees’ medical insurance fund in Jiangsu Province had a total balance of CNY 182 billion (USD 25.3 billion), compared with just CNY 3.5 billion (USD 486.9 million) in the maternity insurance fund.27
Long-term care is covered under a separate insurance program that’s being piloted in selected cities (see Long-Term Care and Social Support).28
Safety Nets
Local governments and social donations fund a medical financial assistance program in both urban and rural areas for individuals who can’t afford individual premiums for publicly financed health insurance or can’t cover out-of-pocket spending.29
This medical financial assistance program prioritizes catastrophic care expenses, with some coverage for emergency department costs. Funds are mainly used to pay for individual deductibles, copayments, and medical spending exceeding annual benefit caps. They also cover individual premiums for publicly financed health insurance.30
In 2023, CNY 74.6 billion (USD 10.4 billion) was allocated to medical assistance, subsidizing 80.2 million people and covering 153.4 million outpatient and inpatient cases. The central government contributed CNY 29.7 billion (USD 4.1 billion) of this amount.31
In 2023, over 99 percent of low-income rural residents were enrolled in basic medical insurance.32
There have also been improvements in the urban and rural medical insurance systems. In 2022, the reimbursement cap for outpatient and emergency care increased from CNY 3,000 (USD 417) to CNY 4,500 (USD 626).33
Additionally, people can reduce their taxable income by deducting high medical expenses. If their medical costs (after insurance reimbursement) exceed CNY 15,000 (USD 2,087) in a year, the excess can be deducted, up to a maximum of CNY 80,000 (USD 11,128) per year. These deductions can be applied to the taxpayer’s income or their spouse’s. Parents can also deduct any medical expenses incurred on behalf of children under age 18.34
The Role of Private Health Insurance
Private health insurance can be purchased individually or offered by employers as a benefit, especially in multinational corporations and large domestic firms. However, it plays a minor role in health care financing, covering only 5 percent of medical costs in 2020, compared with 44 percent from out-of-pocket expenses and 50 percent from basic medical insurance. Low enrollment in private insurance — with only about 4 percent of the population holding private policies — is due to high premiums, strict reimbursement policies, and short coverage periods.35
To address these challenges, in 2015, Huimin Insurance, a government-backed model of private supplementary insurance, was introduced at the local level before expanding across the country in 2020. It offers low premiums, broad coverage, and open enrollment and covers deductibles, copayments, and services not reimbursed by basic medical insurance.36 By 2022, 140 million people (10% of the population across 244 cities and 28 provinces) had enrolled in this coverage, generating CNY 14 billion (USD 1.9 billion) in premiums.37
Huimin Insurance is operated as a public-private partnership. Local governments work with private insurers by sharing basic medical insurance data and facilitating integrated payment systems. In exchange, insurers agree to higher payout rates and profit caps to keep the plans affordable and accessible.38
The Role of Government
The central government has overall responsibility for national health legislation, policy, and administration. Local governments — in provinces, prefectures, cities, counties, and towns — are responsible for organizing and providing these services.39
The Central Committee of the Communist Party of China defines overarching policy priorities, such as the goal of achieving universal health coverage, while the State Council translates these directives into national policy guidelines and coordinates implementation across ministries.40
Both national and local health agencies and authorities have responsibilities that cover health quality and safety, cost control, and provider fee schedules.41
In 2023, the State Council reorganized the central government’s health care structure.42 Agencies have the following responsibilities:43
The National Health Commission is the central health policy and health services regulatory authority, responsible for formulating national health policy, coordinating health system reforms, and overseeing health care services and quality.
The National Healthcare Security Administration, oversees the basic medical insurance programs, maternity insurance, catastrophic medical insurance, medical assistance and fund supervision – including the negotiation, pricing and reimbursement of pharmaceuticals.
The National People’s Congress is responsible for health legislation. (However, the State Council and the Central Committee of the Communist Party can initiate major health policies and reforms that are also regarded as law).
The National Disease Control and Prevention Administration is the lead national body responsible for disease prevention and control, public health surveillance and emergency response.44
The National Administration of Traditional Chinese Medicine is responsible for regulation and oversight of traditional Chinese medicine.45
The Ministry of Finance provides funding for health system infrastructure, government health subsidies, and health insurance contributions.
The National Development and Reform Commission manages health infrastructure projects.
The government is also expanding its role in health through public-private partnerships. These bring private capital and expertise into hospital construction, service delivery, and management. The goal is to increase access and efficiency while maintaining public oversight.46
Integration and Care Coordination
One strategy to better integrate health care delivery is to establish a tiered system whereby primary care facilities manage common and minor illnesses, while complex cases are referred to higher-level hospitals.47
To support this structure, China has been piloting medical consortia — networks linking tertiary hospitals with lower-tier institutions, such as community health centers — in various regions since 2012.48 These consortia establish two-way referral systems, which allow patients to move upward to higher-level hospitals for advanced care and downward to primary care institutions for follow-up rehabilitation. The aim is to reduce hospital overcrowding and use resources more efficiently.49 As of 2023, there are more than 18,000 medical consortia, and 30.3 million two-way referrals were recorded nationwide — a 9.7 percent increase on 2022 figures.50
In 2025, a new national alliance of 62 flagship hospitals was established to further integrate care, predominantly by combining traditional Chinese and Western medicine and incorporating artificial intelligence (AI) and data management tools to enhance coordination.51
Operations and Resources
Overview of the Delivery System
China's health care system is structured into three levels of care:52
Primary care provides basic health care and preventive services to the community. These are delivered by local hospitals and clinics.
Secondary care provides regional comprehensive health services, with secondary care hospitals taking in referrals from primary hospitals. Secondary care hospitals also carry out medical teaching and research.
Tertiary care provides advanced and specialist care. This is offered by large urban hospitals that serve as medical hubs for multiple regions.
Patients pay deductibles and copayments to hospitals for their primary care, specialty physician office visits, and hospital admissions at the point of service. Hospitals bill insurers directly (through electronic billing systems) for the remaining payment.53
Since 2019, there’s been a steady transition away from traditional fee-for-service reimbursement and a move toward bundled payments, using diagnosis-related groups (DRG) and diagnosis intervention packets (DIP).54 Under DRGs, a fixed payment rate is set based on diagnosis, treatment, and patient categories. Under the DIP, the final amount paid depends on the range and severity of the treatment, as well as the service volume (the services delivered).55
Primary Care
Primary care is delivered through a tiered system that includes community health centers in cities and township health centers and village clinics in rural areas.56 These facilities offer basic medical care, chronic disease management, and public health services, with general practitioners (GPs) responsible for diagnosing and treating everyday health problems.57
National reforms to improve access and reduce pressure on hospitals have increased primary care funding substantially. Since 2009, per capita subsidies for essential public health services rose from CNY 15 (USD 2) to CNY 89 (USD 12) by 2023.58 These funds support service delivery, infrastructure, and staff salaries, with additional subsidies and central transfers targeted to underserved regions.59
This funding increase is reflected in the growing workforce. Between 2012 and 2021, the number of GPs increased from 109,794 to 434,868, reaching 30.8 for every 100,000 people in 2021. By 2023, there were 39.9 GPs for every 100,000 people; this figure is projected to rise to 49 by 2026, meeting the government’s 2030 target ahead of schedule.60 In 2022, there were 311 doctors for every 100,000 people, above the average in countries across the Western Pacific (232).61
Despite the rising numbers, rural areas lack qualified GPs. “One of the main challenges is training enough GPs — or nonphysicians like nurses, and nurse practitioners — to deliver preventive care, health promotion, and health management in community health centers and rural clinics,” says Winnie Yip, professor of global health policy and economics at Harvard School of Public Health. Reforms under the Healthy China 2030 strategy aim to enhance rural care infrastructure, “but medically trained professionals often prefer to work in urban areas, which contributes to uneven access,” Yip explains.62
GP registration isn’t mandatory, and residents can access outpatient care at higher-level hospitals without a referral. Some regions promote voluntary contracts between patients and family doctor teams to improve continuity of care.63
One of the main challenges is training enough GPs — or nonphysicians like nurses, and nurse practitioners — to deliver preventive care, health promotion, and health management in community health centers and rural clinics.
Winnie Yip
Professor of Global Health Policy and Economics
Harvard School of Public Health
Most GPs are publicly employed by government-run centers, especially in urban and township settings. In contrast, village doctors typically operate private clinics under local public oversight.64
There are no data on whether GPs are required to provide out-of-hours care.
Outpatient/Specialist Care
Outpatient specialists are employed by and usually work in hospitals. Patients typically select specialists through hospital-based outpatient appointment systems, particularly in tertiary public hospitals.65
Despite the expansion of medical consortia (see Integration and Care Coordination), a lack of gatekeeping mechanisms means that patients don’t need to be referred by their primary care practitioners to access secondary or specialist care. Instead, they can visit these hospitals directly.66 This open-access system has contributed to a steady increase in outpatient volumes: Between 2012 and 2018, outpatient visits to hospitals grew at an average annual rate of 5.7 percent.67
Patient satisfaction with outpatient care in China varies across secondary and tertiary public hospitals. Research in 2018 showed that patients were less satisfied at tertiary care hospitals, primarily due to higher medical expenses, longer treatment durations, and less positive interactions with nonmedical staff.68
While most patients are highly satisfied with the medical part of care, satisfaction scores are lower in nonmedical dimensions such as wait times and the physical environment. A survey of tertiary hospitals in 2017 found that outpatient satisfaction scored 4.4 on a five-point scale, with the highest satisfaction being for service and treatment and the lowest for wait times.69
There are no official data for the number of specialist medical practitioners or the proportion who work publicly versus privately.
Physician Education and the Workforce
Medical education follows a three-stage system: medical school, graduate training, and continuing education. Medical students undertake five years of study and three years of residency.70As of 2021, there were 129 accredited medical schools, all of which were public, and more than 1.25 million students enrolled in medical programs — more than double the number in 2012.71
Tuition fees at public universities often range between about CNY 5,000 (USD 696) and CNY 7,000 (USD 974) per year.72
The health care workforce has grown overall. By 2023, there were 15.2 million health personnel, up from 14.4 million in 2022. Of these personnel, 4 million were doctors, and 5.7 million were nurses.73
Despite this growth, rural and remote areas have a shortage of qualified health professionals. Between 2021 and 2022, 55.6 percent of village doctors said there was insufficient staffing and 67.7 percent identified lack of skills in medical staff.74 They also said there were limited opportunities for further training and advancement, which has made retention more difficult in some regions.75
To improve medical provision in rural or remote areas, the 2010 Rural-Oriented Tuition-Waived Medical Education (RTME) program offers free tuition and living stipends to students admitted with lower entrance scores in exchange for six years of compulsory service in township health centers. Among the RTME graduates surveyed between 2015 and 2019, 86.1 percent entered rural service as required.76 But long-term retention is a concern: Between 2021 and 2022, only 31.8 percent of respondents indicated that they had plans to stay in rural health institutions after completing their six-year contracts.77
In 2025, the National Health Commission reported that over 1,500 health care professionals from outside the mainland were practicing in China under short-term arrangements.78 This comes after the introduction of new measures streamlining approvals for qualified foreign-trained doctors (including from Hong Kong, Macao, and Taiwan) to practice in the country on a short-term basis. However, there are no official data for the number of foreign-trained doctors.79 There are also no data for the proportion of the workforce that chooses to work overseas.
Hospitals
BY THE NUMBERS
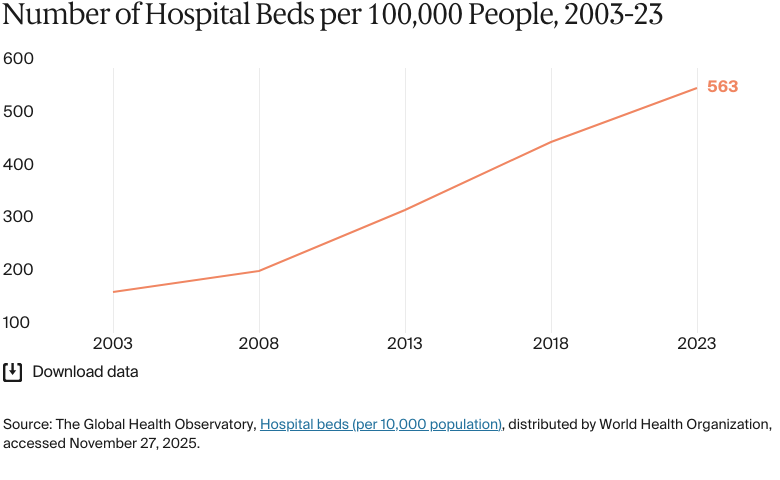
In 2023, there were 563 hospital beds per 100,000 people.80
In 2022, there were 367 nurses and midwives per 100,000 people (fewer than the Western Pacific average of 434).81
Hospitals can be public or private, nonprofit or for-profit.82 Rural township hospitals and urban community hospitals are often seen as primary care facilities.83
In 2023, there were 26,583 private hospitals and 11,772 public hospitals.84 Public hospitals provide the vast majority of care, accounting for 84.2 percent of outpatient visits and 81.4 percent of hospitalizations in 2021.85
Public hospitals are owned and managed by various levels of government agencies. The National Health Commission plays a central regulatory and administrative role in the health system, but it doesn’t directly control all hospitals — especially those affiliated with medical universities, which operate independently. Local health commissions and government departments at the provincial, city, and county levels often own public hospitals and exercise administrative authority over them. Additionally, national universities (which are directly administered by the Ministry of Education) maintain affiliated hospitals outside the National Health Commission’s direct control.86
Fee-for-service was historically the dominant provider payment method, but this has changed since 2021 with the transition to DRG/DIP payment models (see Overview of the Delivery System).87
Mental Health Care
BY THE NUMBERS
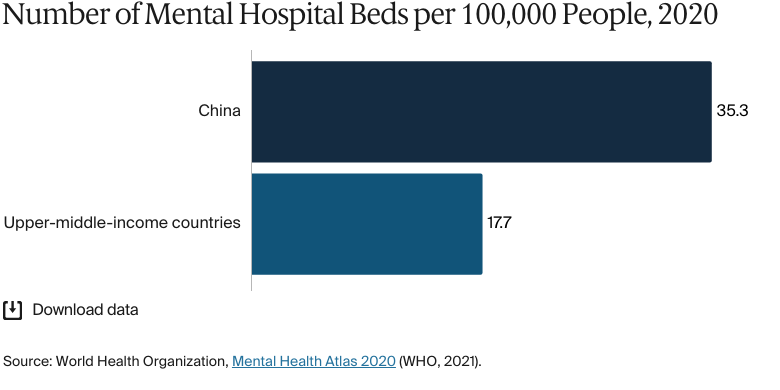
In 2020, there were 35 mental hospital beds per 100,000 people, significantly higher than the 18-bed average in upper-middle-income countries.88
In 2020, there were three psychiatrists per 100,000 people, higher than the average of two in upper-middle-income countries.89
In 2020, there were nine mental health professionals per 100,000 people, lower than the average of 15 in upper-middle-income countries.90
The diagnosis, treatment, and rehabilitation of mental health conditions are undertaken in special psychiatric hospitals and in the psychology departments of tertiary hospitals. Patients with mild illnesses are often treated at home or in community clinics; only severely ill patients are treated in mental hospitals.91
Since 2009, there have been significant efforts to expand and integrate mental health care into the broader health system. That year marked the incorporation of community-based mental health services into basic medical insurance, including follow-up care and rehabilitation guidance for patients with severe mental disorders. The 2012 Mental Health Law formalized patients’ rights and outlined who was responsible for service provision. By 2020, psychiatric departments had been established in over 3,000 general hospitals — four times the number in 2010 — and the number of psychiatrists had increased by nearly 145 percent.92
As part of the Healthy China 2030 strategy, in 2019, China launched the Healthy China Action (2019–2030) initiative, which is centered on prevention and health promotion. It focuses on prevailing health determinants, at-risk populations, and leading health concerns.93 In 2023, the government set a target for 95 percent of schools and universities to be staffed with psychology teachers by 2025, alongside mental health evaluations for students and expanded counseling services.94
To further improve access, a nationwide psychological support hotline was rolled out in early 2025. By May 2025, the hotlilne was operational in all 31 provinces. Additionally, the central government plans to implement outpatient services for psychological and sleep disorders in at least one hospital in every prefecture and city by 2025.95
Despite these improvements, mental health services are still unevenly distributed, with rural and less-developed regions facing shortages in trained personnel and infrastructure.96 Psychotherapy services, in particular, are underdeveloped because of a lack of standardized training, unclear pricing mechanisms, and limited integration into public health coverage.97
Long-Term Care and Social Support
To meet the needs of its rapidly aging population, China launched a long-term care insurance (LTCI) system in pilot cities in 2016.98 By the end of 2024, more than 180 million people had LTCI, and as of 2025, it is operational in 49 cities (out of 694).99
LTCI, which is voluntary, is designed to help individuals who can no longer manage basic daily tasks due to age, illness, injury, or cognitive decline.100 Long-term care isn’t universally free: Financing comes from a mix of public medical insurance funds, government subsidies, and individual contributions.101 For example, in Zhejiang Province, residents pay CNY 90 (USD 13) to be part of the LTCI program.102
Still, access to long-term care can be difficult. Although the government has expanded institutional care, many facilities remain underused. There’s also a shortage of home- and community-based services, which are preferred by most older adults.103
Staffing shortages also strain the system. Many caregivers are older adults themselves, have limited formal training, and earn low wages.104 In February 2025, the government reported approximately 500,000 qualified nurses — far short of the estimated demand of 10 million.105
In rural China, informal care provided by family members is still the norm. The government has managed to establish a rural pension insurance system and to level up medical and social assistance since the early 2000s, but the security system for the elderly remains at an early stage.106
Cost and Affordability
Health Care Spending Overview
Health care spending as a share of gross domestic product (GDP) has followed an upward trajectory since the 2009 reforms. In 2023, the ratio was estimated at 7.2 percent, up from 6.6 percent in 2019.107 This was the same as the 2022 average for upper-middle-income countries (7.1%) but below that for the Western Pacific region (8.1%).108
Total health expenditure increased from CNY 85.3 trillion (USD 11.9 trillion) in 2022 to CNY 90.6 trillion (USD 12.6 trillion) in 2023. In 2023, the expenditure per capita of CNY 6,425 (USD 894) was above the upper-middle-income country average for 2022 (USD 585).109
In 2023, social health spending was the largest source of health expenditure, at 46 percent. Social health spending encompasses social security, private health security, and nonpublic medical expenditure, alongside social donation assistance and administrative income.110 The next highest were out-of-pocket spending (27.3%) and government spending (26.7%).111
Pharmaceutical Spending
As of 2022, pharmaceutical spending accounted for 26.9 percent of China’s total health expenditure. Outpatient pharmaceutical spending has steadily increased, now making up 39 percent of total pharmaceutical expenditures, while hospital pharmaceutical spending has declined to 27.5 percent.112
Several cost-containment measures included within broader health care reforms have been designed to manage pharmaceutical expenditures. Centralized price negotiations with pharmaceutical companies, for example, have helped to make drugs cost-effective.113 The “4 + 7” drug procurement reform has centralized drug purchasing, reduced prices, and encouraged greater use of generics.114
Cost Sharing and Out-of-Pocket Spending
In 2023, out-of-pocket spending accounted for 32.17 percent of total health expenditure, more than the 30.6 percent average for upper-middle-income countries in 2022.115 In 2022, per capita out-of-pocket spending was USD 215, compared with USD 181.9 in upper-middle-income countries.116
Total medical expenses are not entirely covered by health insurance; there is also some level of cost sharing involved, with patients expected to pay copayments or other out-of-pocket expenses depending on the type of care they receive and their insurance coverage.117
Outpatient services, such as clinic visits, diagnostics, and prescriptions, typically have a higher cost-sharing element than does inpatient care. The latest government data show that 70 percent of inpatient and about 50 percent of outpatient costs were covered by public insurance.118 Some regions have deployed measures to alleviate this burden for patients. In 2023, outpatient services in Wuhan were reimbursed at 50 to 68 percent under the city’s 2023 outpatient mutual aid policy, which also set annual caps of CNY 3,500 (USD 487) for working individuals and CNY 4,000 (USD 556) for retirees.119
These local reforms were part of a broader effort to improve affordability and reduce avoidable hospitalizations. The 2021 outpatient coordination reform addressed structural inefficiencies by redirecting employer insurance contributions from underused personal medical accounts into a pooled fund. This allowed inpatient and outpatient claims to be reimbursed from the same source. The reform benefited patients with chronic illnesses who rely on regular outpatient care and medications.120
Medication copayments vary, but many prices were significantly reduced after being included in the National Reimbursement Drug List in 2023.121 That year, pharmaceutical manufacturers secured national coverage for 111 new products by agreeing to price cuts of 60.1 percent on average, which reduced costs for patients across a wide range of therapies. For example, the price of a rare disease drug used to treat spinal muscular atrophy dropped from CNY 63,800 (USD 8,874) to CNY 3,780 (USD 526) per bottle — a 94 percent reduction — after it was added to the National Reimbursement Drug List.122
There are no current data for the proportion of the population pushed below the poverty line by health care costs.
How Are Costs Contained?
Since 2018, the National Healthcare Security Administration has been leading a major reform to reduce drug prices through a system known as centralized, volume-based procurement. Under this program, the government pools demand from public hospitals across the country and organizes national bidding rounds where pharmaceutical companies compete to supply large amounts of commonly used, off-patent drugs. In exchange for guaranteed sales, the companies offer significantly lower prices. This approach has significantly reduced costs: By 2024, average prices had dropped by more than 70 percent across 10 procurement rounds, with some drug prices going down by more than 90 percent.123
In 2020, the government strengthened policies limiting the growth of high-cost health care infrastructure (such as the construction of new hospitals, expansion of the number of hospital beds, and purchase of expensive medical equipment, such as MRI scanners). Instead, resources are being directed toward upgrading existing facilities, expanding primary care, and promoting digital health infrastructure. All this is part of the Healthy China 2030 strategy.124
Quality and Outcomes
Health Outcomes
BY THE NUMBERS
In 2021, average life expectancy was 78 years (compared with an average of 74.2 years in upper-middle-income countries in 2021).125
Ischemic heart disease: 137 deaths per 100,000 people
Chronic obstructive pulmonary disease: 89 deaths per 100,000 people.
The maternal mortality rate was 15 deaths per 100,000 live births in 2023 (compared with an average of 35 deaths across the Western Pacific).127
The infant mortality rate was five deaths per 1,000 live births in 2023 (compared with an average of 12 deaths in upper-middle-income countries).128
In 2021, the share of the population with mental health disorders was 12 percent (compared with an average of 14% in upper-middle-income countries).129
The suicide rate was seven per 100,000 people in 2021, the same as in upper-middle-income countries.130
The gun death rate was 0.02 deaths per 100,000 people in 2023.131
7 percent of adults were affected by obesity in 2023 (compared with an average of 16% in upper-middle-income countries).132
There are currently no data available for the avoidable mortality rate in China.
Women in China live longer than men. In 2021, women’s average life expectancy was 80.5 years, compared with 75 years for men.133
Avoidable mortality among children under age 5 in China decreased by an average of 10.7 percent between 2004 and 2021, with urban–rural differences.134
Noncommunicable diseases accounted for 90.7 percent of deaths in 2021. Strokes were the leading cause of death,largely caused by hypertension. In 2020, 80.9 percent of stroke patients had also been diagnosed with hypertension.135 During 2005–2020, 87 percent of young adults with hypertension had not received treatment, and only 6.8 percent were aware of their condition.136
Long wait times are a persistent issue in the Chinese health care system, particularly in urban tertiary hospitals.137 Patients have often cited delays at registration, during diagnostic testing, and in settling their bills.138 In 2024, the government reported that it had made significant progress in responding to this issue. Some hospitals, such as those in Jiangsu, were implementing new policies to reduce in-hospital wait times and increase overall convenience for patients (see Health Care Innovation).139
Addressing Health Inequities
There are significant disparities in health care, primarily between urban and rural populations.140 In 2021, urban residents earned 2.5 times more in disposable income than their rural counterparts — a gap that directly affects access to health care.141 Urban areas have better medical facilities, specialized services, and more health care professionals, while rural populations have limited infrastructure, fewer trained doctors, and long travel distances.142
These structural inequities are reflected in outcomes. In 2021, life expectancy for urban populations exceeded that of rural populations by two years overall — with a 1.8-year gap for women and a 2.1-year gap for men.143
The URRBMI is tied to the household registration (hukou) system, which categorizes individuals as either rural or urban residents based on their place of origin — a status that’s typically inherited from parents. Even children born in cities to rural parents often hold a rural hukou, which limits their eligibility for urban services.144
This system creates particular challenges for rural migrants working in cities. Without an urban hukou, rural migrants are frequently excluded from public health insurance programs and employer-based services. This forces them to pay higher out-of-pocket costs or return to their hukou-registered hometowns for affordable care, which can disrupt continuity of treatment. Despite doing similar jobs, rural hukou holders often earn less and face restricted access to labor protections, health care, and social security.145
To make care more accessible for patients seeking treatment outside their hukou, China has expanded its national inter-provincial medical insurance settlement network.146 Administered by the National Healthcare Security Administration, this system allows patients to receive real-time insurance reimbursement when seeking care outside their home region, eliminating the need for lengthy reimbursement procedures.147 By the end of 2023, more than 550,000 designated medical institutions were connected to the network, enabling direct settlement for 120 million outpatient visits and 11.2 million inpatient stays across provinces.148
In areas with high proportions of ethnic minorities, such as Yunnan and Sichuan, use of maternal and child health services was found to be lower for minority women than for Han women, with disparities in terms of access to doctors and geographic accessibility to hospitals.149 There is a poor health literacy rate among some minority groups, such as the Hui, which has also led to a poor health-related quality of life and high prevalence of chronic diseases.150
A local initiative to address these disparities was the Ten-Year Action Plan for Health Development in Ethnic Minority Counties of Sichuan Province. Between 2011 and 2020, the Sichuan Province government invested over CNY 2 billion (USD 278 million) to expand the province’s medical infrastructure and boost the number of health care professionals serving ethnic minority communities in the region.151
Additionally, in 2023, the medical assistance fund subsidized the participation of 80.2 million people in basic medical insurance, which meant that over 99 percent of low-income rural populations were covered.152
Health Inequities Faced by the Uyghur Population
The Xinjiang Uyghur Autonomous Region is a majority Muslim population consisting of Uyghurs and other ethnically Turkic communities.153 In 2023, Chinese Han households in the region reported fewer deaths than Turkic households — one death for every 29 Han households compared with one death for every nine Turkic households.154
There have also been reports of widespread violations of reproductive rights, with claims that leaked Chinese government documents in 2019 indicated that a mass female sterilization campaign had taken place in Uyghur regions. Part of this policy included the forced implementation of intrauterine devices (IUDs). In 2018, 80 percent of all IUD placements in China happened in Xinjiang, a region comprising only 1.8 percent of the country’s population.155
Innovation and Reform
Health Care Innovation
To tackle high medical costs, in 2018, China launched a bulk procurement program for pharmaceuticals that centralized drug purchasing to reduce costs and expand access. Since the program’s launch, prices have been more than halved on average. In 2024, the government forecast that the program would expand to include 500 medications.156
There have also been reforms targeting the long wait times and fragmented administrative procedures in hospitals. As of 2024, more than 5,500 hospitals offered integrated “one-stop” services that allowed patients to register, receive care, and settle bills within the same system. This enabled 77.7 percent of hospitalized individuals to pay their bills the day they were discharged.157
Health Care Technology
There have been significant investments in digital health care, with nearly CNY 60 billion (USD 8.3 billion) allocated to “smart medicine” in 2021.158 The ;government's Five-Year Plan (2021–2025) sets an annual research and development growth target of 7 percent, with an emphasis on AI and digital integration in health care. Initiatives include enhancing grassroots digital health care, developing health information platforms, and encouraging the integration of traditional Chinese medicine.159
Telemedicine
Telemedicine uptake has accelerated because of national health reform agendas and an expanding digital infrastructure. By the end of 2023, 67.6 percent of secondary and higher-level public hospitals had adopted telemedicine services.160
AI
The government is using AI applications to aid drug research, diagnostics, and hospital management. For instance, there are more than 1,000 “internet hospitals” backed by tech firms such as Alibaba, Tencent, and Ping An. These hospitals offer online consultations, e-pharmacy services, and hospital information support systems. In addition, big data plays an increasing role in personalized care and predictive diagnostics.161
“Using AI to support diagnosis and treatment at community and primary care level is very much on China’s policy agenda,” says Harvard School of Public Health’s Winnie Yip. “However, the effectiveness and feasibility of use at this level remains to be proven.”
Electronic Health Records
There’s been substantial progress in electronic health and medical records since 2009. As of 2018, 97.8 percent of permanent residents had electronic health records, although their actual usage rates and post-2018 coverage data have not been reported.162
Despite this widespread coverage, it’s difficult to achieve seamless data integration. Hospitals often use inconsistent data standards and fragmented systems, making it difficult to share information across institutions. For example, the more than 500 hospitals in Beijing alone operate on more than 40 different IT systems. Even some hospitals under the same local health authority or university affiliation use incompatible systems, limiting the coordination of care.163
In 2017–18, the government initiated efforts to create standardized, interoperable platforms that would improve data sharing and care coordination. Supporting these reforms, China's health care IT market is projected to grow from CNY 80 billion (USD 11 billion) in 2021 to CNY 140 billion (USD 19.5 billion) by 2025.164
This content was produced by FT Longitude, the specialist research and content marketing division of the Financial Times Group, on behalf of the Commonwealth Fund. Research and content for the Commonwealth Fund country profiles were collected by FT Longitude between February and December 2025.
This profile reflects data as of January 2026. New or updated information may have become available since its release.
Notes
1
Wenjuan Tao et al., “Towards universal health coverage: lessons from 10 years of healthcare reform in China.” BMJ Global Health, 5, no. 3 (2020):e002086, https://doi.org/10.1136/bmjgh-2019-002086.
↩
Jiajia Zhang et al., “China’s universal medical insurance scheme: progress and perspectives.” BMC Global and Public Health 2, no. 62 (September 11, 2024), https://doi.org/10.1186/s44263-024-00096-9.
↩
7
Hao Yu, “Universal health insurance coverage for 1.3 billion people: what accounts for China's success?” Health Policy 119, no. 9 (September 2015):1145–52, https://doi.org/10.1016/j.healthpol.2015.07.008.
↩
8
Jiajia Zhang et al., “China’s universal medical insurance.”
↩
Liangwen Zhang et al., “Effects of urban and rural resident basic medical insurance on healthcare utilization inequality in China.” International Journal of Public Health 16, no. 68 (February 16, 2023):1605521, https://doi.org/10.3389/ijph.2023.1605521; Jiajia Zhang et al., “China’s universal medical insurance.”
↩
“Reply from the National Healthcare Security Administration to Proposal No. 9447 of the fourth session of the 13th National People's Congress,” National Healthcare Security Administration (Guójiā Yīliáo Bǎozhàng Jú), October 25, 2021, https://www.nhsa.gov.cn/art/2021/10/25/art_110_7250.html.
↩
20
International Labour Organization, Social Protection in Action.↩
Beibei Yuan et al., “Strengthening public health services to achieve universal health coverage in China.” BMJ 365 (June 21, 2019):12358, https://doi.org/10.1136/bmj.l2358; Xiao Tan and Christine Wong, “Anatomy of intergovernmental finance for essential public health services in China,” BMC Public Health 22, no. 914 (May 9, 2022), https://doi.org/10.1186/s12889-022-13300-y.
↩
Xinyu Zhao et al., “Incidence, causes and risk”; International Agency for the Prevention of Blindness, Financial Barriers.
↩
25
International Labour Organization, Social Protection in Action.↩
26
“General Office of the State Council on Comprehensively Promoting Maternity Insurance and Opinions on the Merger of Basic Medical Insurance for Employees,” The State Council, accessed December 1, 2025, https://www.gov.cn/zhengce/zhengceku/2019-03/25/content_5376559.htm; Xiaotian Zhang et al., “Effects of incentive-based population policies on sustainability of China’s recent maternity insurance system reform: a system dynamics simulation.” Health Research Policy and Systems 20, no. 140 (December 28, 2022):36578006, https://doi.org/10.1186/s12961-022-00945-9.
↩
27
Xiaotian Zhang et al., “Effects of incentive-based population policies.”
↩
28
Simiao Chen et al., “Long-term care insurance in China: current challenges and recommendations.” Journal of Global Health 14 (September 27, 2024):03015, https://doi.org/10.7189/jogh.14.03015.
↩
29
Yucheng Chen et al., “The impact of medical financial assistance on healthcare expenses and the medical financial burden: evidence from rural China,” Frontiers in Public Health 10 (January 19, 2023):1021435, https://doi.org/10.3389/fpubh.2022.1021435.
↩
30
Chen et al., “Impact of medical financial assistance.”
↩
31
“Statistical bulletin on the development of national medical security in 2023,” National Healthcare Security Administration (Guójiā Yīliáo Bǎozhàng Jú), July 25, 2024, https://www.nhsa.gov.cn/art/2024/7/25/art_7_13340.html.
↩
32
National Healthcare Security Administration, “Statistical bulletin.”
↩
“Who can enjoy deduction for health-care costs for major diseases? What and how much are the deductible health-care costs for major diseases?” State Taxation Administration (Guójiā Shuìwù Zǒngjú), September 11, 2023, https://www.chinatax.gov.cn/eng/c102444/c5211896/content.html.
↩
35
Nuo Chen et al., “Preferences for private health insurance in China: a discrete choice experiment.” Frontiers in Public Health 10 (September 6, 2022):985582, https://doi.org/10.3389/fpubh.2022.985582.
↩
36
Chen et al., “Preferences for private health insurance.”
↩
37
Chen et al., “Preferences for private health insurance”; figures calculated using population data from World Bank Open Data, Population, total, distributed by World Bank Group, accessed November 27, 2025, https://data.worldbank.org/indicator/SP.POP.TOTL).
↩
38
Chen et al., “Preferences for private health insurance.”
↩
39
Yuxi Wang et al., “Assessing the design of China’s complex health system: concerns on equity and efficiency.” Health Policy Open 1 (December 2020):100021, https://doi.org/10.1016/j.hpopen.2020.100021.
↩
40
Qingyue Meng et al., “What can we learn from China’s health system reform?” BMJ 365 (June 19, 2019):12349, https://doi.org/10.1136/bmj.l2349; Wang et al., “China’s complex health system.”
↩
41
Jiwei Qian and M Ramesh, “Strengthening primary health care in China: governance and policy challenges.” Health Economics, Policy and Law 19, no. 1 (October 17, 2023), https://doi.org/10.1017/S1744133123000257; Yanxian Lin et al., “Assessing the price levels of medical service and influential factors: evidence from China.” BMC Public Health 24, no. 119 (January 8, 2024), https://doi.org/10.1186/s12889-024-17639-2.
↩
Yanginq Zhang, et al., “Opportunities and challenges in China’s CDC system reform: a grassroots perspective,” International Health (2025), https://doi.org/10.1093/inthealth/ihaf061.
↩
Bo Liu et al., “The public–private partnerships in healthcare sector in China.” Chronic Diseases and Translational Medicine 9, no. 4 (August 11, 2023):288–98, https://doi.org/10.1002/cdt3.88.
↩
47
Xing Lin Feng et al, “Extending access to essential services against constraints: the three-tier health service delivery system in rural China (1949–1980).” International Journal for Equity in Health 16, no. 49 (May 23, 2017), https://doi.org/10.1186/s12939-017-0541-y; “A tiered health-care delivery system for China,” The Lancet 393, no. 10177 (March 23, 2019):P1178, https://doi.org/10.1016/S0140-6736(19)30730-5.
↩
48
Huan Gao et al., “The pathway of China’s integrated delivery system: based on the analysis of the medical consortium policies.” Current Medical Science 42 (October 17, 2022):1164–71, https://doi.org/10.1007/s11596-022-2654-9; Xinmei Yang et al., “Effects of medical consortium policy on health services: an interrupted time-series analysis in Sanming, China.” Frontiers in Public Health 24, no. 12 (January 24, 2024):1322949, https://doi.org/10.3389/fpubh.2024.1322949.
↩
49
Shasha Yuan et al., “Primary healthcare professionals’ perspective on vertical integration of healthcare system in China: a qualitative study.” BMJ Open 12, no. 2 (February 1, 2022):e057063, https://doi.org/10.1136/bmjopen-2021-057063.
↩
Shuyan Lin et al., “How medical insurance payment systems affect the physicians’ provision behavior in China: based on experimental economics.” Frontiers in Public Health 12 (May 2, 2024), https://doi.org/10.3389/fpubh.2024.1323090; Xinyu Zhang et al., “Hospital response to a new case-based payment system in China: the patient selection effect.” Health Policy and Planning 39, no. 5 (April 6, 2024):519–27, https://doi.org/10.1093/heapol/czae022; Huigang Liang, “Electronic data interchange usage in China's healthcare organizations: the case of Beijing's hospitals.” International Journal of Information Management 24, no. 6(December 2004): 507–22, https://doi.org/10.1016/j.ijinfomgt.2004.08.001.
↩
Jin Xu and BeiBei Yuan, FinancingPrimary Health Care in China (Lancet Global Health Commission on Financing Primary Health Care, 2021), https://www.lshtm.ac.uk/media/59781.
↩
58
Beijing Statistics, “Significant progress has been made in the health and wellness sector, and the people's health rights have been effectively protected—the 22nd in a series of reports on the economic and social development achievements of the People's Republic of China over the past 75 years,” The Paper (Péngpài Xīnwén), September 25, 2024, https://www.thepaper.cn/newsDetail_forward_28851266.
↩
National Health Commission (Guójiā Wèishēng Jiànkāng Wěiyuánhuì), “Statistical bulletin on the development of China's health and wellness undertakings in 2023,” Gov.cn, August 29, 2024, https://www.gov.cn/lianbo/bumen/202408/content_6971241.htm; Ruxin Kou et al., “Equity and trends in general practitioners’ allocation in China: based on ten years of data from 2012 to 2021.” Human Resources for Health 21, no. 61 (August 2, 2023), https://doi.org/10.1186/s12960-023-00841-5.
↩
Minjie Chen et al., “Enhancing access to specialist appointments in tertiary healthcare in Shanghai, China: a structured reservation pathway using digital health technologies.” BMJ Open 14 (December 12, 2024):e085431, https://doi.org/10.1136/bmjopen-2024-085431.
↩
66
Xinyu Zhao et al., “Patient preferences and attitudes towards first choice medical services in Shenzhen, China: a cross-sectional study.” BMJ Open 12 (May 24, 2022):e057280, https://doi.org/10.1136/bmjopen-2021-057280; Yun Liu, “Understanding patient choice of health care facilities in China” (Ph.D. thesis, Erasmus University Rotterdam, 2021), https://repub.eur.nl/pub/135627/12186insidepagesorder.pdf.
↩
67
Weicun Ren et al., “The situation and influencing factors of outpatient satisfaction in large hospitals: evidence from Henan province, China.” BMC Health Services Research 21, no. 500 (May 25, 2021), https://doi.org/10.1186/s12913-021-06520-2.
↩
68
Jingjing Yan et al., “Patient satisfaction with outpatient care in China: a comparison of public secondary and tertiary hospitals.” International Journal for Quality in Health Care 33, no. 1 (February 2, 2021):mzab003, https://doi.org/10.1093/intqhc/mzab003.
↩
69
Linlin Hu et al., “How perceived quality of care affects outpatient satisfaction in China: a cross-sectional study of 136 tertiary hospitals.” INQUIRY: The Journal of Health Care Organization, Provision, and Financing 56 (December 30, 2019), https://doi.org/10.1177/0046958019895397.
↩
70
Weimin Wang, “Medical education in China: progress in the past 70 years and a vision for the future.” BMC Medical Education 21, no. 453 (August 28, 2021), https://doi.org/10.1186/s12909-021-02875-6.
↩
“What will the tuition fee be for China Medical University in 2025? (See the fee schedule for each major),” GK100.com, May 5, 2025, https://www.gk100.com/read_22135750.htm; Teacher Jiajia, “Chengdu Medical College 2024 annual tuition fee revenue and expenditure special report,” Chengdu Medical College (Chéngdū Yīxuéyuàn), March 28, 2025, https://cwc.cmc.edu.cn/info/1011/1367.htm.
↩
73
National Health Commission, “Statistical bulletin.”
↩
74
Renmin Jin and Yan Chen, “Job satisfaction of village doctors in a rural-oriented tuition-waived medical education program in China.” Frontiers in Psychology 14 (July 25, 2023), https://doi.org/10.3389/fpsyg.2023.1184430.
↩
75
Dan Hu et al., “Evaluation of a medical education policy with compulsory rural service in China.” Frontiers in Public Health 11 (February 2, 2023):1042898, https://doi.org/10.3389/fpubh.2023.1042898.
↩
76
Hu et al., “Evaluation of a medical education policy.”
↩
Qi Zhang and Audrey Laporte, “Determinants of capital structure: a case of hospitals in China.” BMC Health Services Research 25, no. 1083 (August 15, 2025), https://doi.org/10.1186/s12913-025-13263-x.
↩
83
“During the 14th Five-Year Plan period, we will promote the high-quality development of the urban and rural community medical and health service system,” Gov.cn, February 9, 2022, https://www.gov.cn/xinwen/2022-02/09/content_5672796.htm.
↩
84
National Health Commission, “Statistical bulletin.”
↩
85
Xiaozi Zhange et al., “Rapid growth of private hospitals in China: emerging challenges and opportunities to health sector management.” The Lancet Regional Health 44, no. 100991 (March 2024), https://doi.org/10.1016/j.lanwpc.2023.100991.
↩
World Health Organization, Member State Profile; World Health Organization, Mental Health Atlas.
↩
90
World Health Organization, Member State Profile; World Health Organization, Mental Health Atlas.↩
91
Runzi Chen et al., “Mental health policy and implementation from 2009 to 2020 in China.” SSM: Mental Health 4 (December 15, 2023):100244, https://doi.org/10.1016/j.ssmmh.2023.100244.
↩
Chen et al., “Mental health policy”; World Health Organization, “Mental Health in China.”
↩
98
Kuan Du et al., “Evaluation of long-term care insurance pilot city policies in China: a cross-sectional study.” Frontiers in Public Health 13 (March 21, 2025), https://doi.org/10.3389/fpubh.2025.1570794; Xueying Xu et al., “Life expectancy, long-term care demand and dynamic financing mechanism simulation: an empirical study of Zhejiang Pilot, China.” BMC Health Services Research 24, no. 469 (April 15, 2024), https://doi.org/10.1186/s12913-024-10875-7.
↩
Qingwei Wang, “Modernizing care for older adults: long-term care policy evolution and challenges in China.” Journal of Aging and Social Policy (March 28, 2025):1–17, https://doi.org/10.1080/08959420.2025.2482299.
↩
Lianjie Wang and Yao Tang, “Changing trends and the effectiveness of informal care among rural elderly adults in China.” Sage Open 13, no. 4 (October 17, 2023), https://doi.org/10.1177/21582440231202580.
↩
The Global Health Observatory, Current health expenditure.
↩
109
National Health Commission, “Statistical bulletin”; Institute for Health Metrics and Evaluation, China, all-cause total spending, 2022–2023, distributed by IHME, accessed November 27, 2025, http://ihmeuw.org/7b6q.
↩
110
National Health Commission, “Statistical bulletin”; Hong-yan Li and Rui-xue Zhang, “Analysis of the structure and trend prediction of China’s total health expenditure.” Frontiers in Public Health 12 (September 24, 2024), https://doi.org/10.3389/fpubh.2024.1425716.
↩
111
National Health Commission, “Statistical bulletin.”
↩
112
Li and Zhang, “China’s total health expenditure.”
↩
113
Lei Si et al., “Using strategic price negotiations to contain costs and expand access to medicines in China.” BMJ Global Health 5, no. 1 (2020), https://doi.org/10.1136/bmjgh-2019-002256.
↩
Institute for Health Metrics and Evaluation, China, all-cause spending per person, 2022–2022, distributed by IHME, accessed November 27, 2025, http://ihmeuw.org/7b6r.
↩
117
“How will the reform of medical insurance payment methods affect medical treatment?” National Healthcare Security Administration (Guójiā Yīliáo Bǎozhàng Jú), April 10, 2024, https://www.nhsa.gov.cn/art/2024/4/10/art_14_12344.html; “Understand it all in one article! What do medical insurance pooled payments, personal payments, and out-of-pocket expenses mean?” The Paper (Péngpài Xīnwén), October 7, 2024, https://www.thepaper.cn/newsDetail_forward_28959896; “Statistical bulletin on the development of national medical security in 2024,” National Healthcare Security Administration (Guójiā Yīliáo Bǎozhàng Jú), July 14, 2025, https://www.nhsa.gov.cn/art/2025/7/14/art_7_17248.html.
↩
118
“National Healthcare Security Administration: the reimbursement rate for inpatient expenses within the policy scope remains stable at around 70%,” China National Radio, August 26, 2024, https://news.cnr.cn/native/gd/kx/20240826/t20240826_526872627.shtml; General Office of the State Council (Guówùyuàn Bàngōngtīng), “Guiding opinions of the General Office of the State Council on establishing and improving the outpatient co-payment mechanism for basic medical insurance for employees,” Gov.cn, April 22, 2021, https://www.gov.cn/zhengce/content/2021-04/22/content_5601280.htm.
↩
119
Junnan Jiang et al., “Does outpatient mutual‐aid reduce oncology patients' utilization of inpatient services? An empirical study of outpatient mutual‐aid policy in Wuhan, China.” International Journal of Health Planning and Management 40, no. 1 (October 7, 2024):174–93, https://doi.org/10.1002/hpm.3858.
↩
120
Jingping Lin et al., “Outpatient coordination reform improves the sustainability of China's Urban Employee Basic Medical Insurance Fund.” Frontiers in Public Health 12 (November 26, 2024), https://doi.org/10.3389/fpubh.2024.1446408; “Localities across China further explain health insurance reform,” Global Times, February 22, 2023, https://www.globaltimes.cn/page/202302/1286054.shtml.
↩
Institute for Health Metrics and Evaluation, GBD compare, distributed by IHME, accessed November 27, 2025, https://vizhub.healthdata.org/gbd-compare/; overall firearm mortality is an aggregate of physical violence by firearm, self-harm by firearm, and unintentional injuries by firearm.
↩
You-Xiang Wang et al., “Temporal trends of avoidable mortality among children under-five in China from 2004 to 2021,” Pediatric Research 98, no. 5 (November 2025): 1753–59, https://doi.org/10.1038/s41390-025-03979-1.
↩
135
World Health Organization, Health data overview for the People’s Republic of China, distributed by WHO, accessed November 27, 2025,https://data.who.int/countries/156; Wen-Jun Tu et al., “Estimated burden of stroke in China in 2020.” JAMA Network Open 6, no. 3 (March 1, 2023):e231455, https://doi.org/10.1001/jamanetworkopen.2023.1455.
↩
136
Zixin Wang, “National and subnational trends of mortality and years of life lost due to stroke and its subtypes in young adults in China, 2005–2020.” Neurology 103, no. 10 (October 25, 2024):e209982, https://doi.org/10.1212/WNL.0000000000209982.
↩
137
Jing Sun et al., “Reducing waiting time and raising outpatient satisfaction in a Chinese public tertiary general hospital: an interrupted time series study.” BMC Public Health 17, no. 668 (August 22, 2017), https://doi.org/10.1186/s12889-017-4667-z.
↩
138
Xiaoyi Wang et al., “Patient-centered outpatient process optimization system based on intelligent guidance in a large tertiary hospital in China: implementation report.” JMIR Medical Informatics 13 (September 1, 2025), https://doi.org/10.2196/60219.
↩
Jian Sun et al., “The effect of new rural cooperative medical scheme on the socioeconomic inequality in inpatient service utilization among the elderly in China” Risk Management and Healthcare Policy 13 (August 29, 2020):1383–90, https://doi.org/10.2147/RMHP.S252336; UNICEF China, “Basic medical insurance”; Sun et al., “Situation, challenges, and countermeasures.”
↩
Generis Global, Overview of the healthcare system.”
↩
143
Shasha Han et al., “Widening rural–urban gap in life expectancy in China since COVID-19.” BMJ Global Health 8, no. 9 (September 19, 2023):e012646, https://doi.org/10.1136/bmjgh-2023-012646; the source calculates the gap in months — 23.7 months overall, 21.2 months for women, and 24.9 months for men.
↩
144
UNICEF China, “Basic medical insurance”; Sun et al., “Situation, challenges, and countermeasures”; Martin Pollard, “Why millions of Chinese are becoming official,” BBC News, December 10, 2015, https://www.bbc.co.uk/news/world-asia-35063788.
↩
National Healthcare Security Administration (Guójiā Yīliáo Bǎozhàng Jú) and Ministry of Finance (Zhōnghuá Rénmín Gònghéguó Cái Zhèngbù), “Notice from the National Healthcare Security Administration and the Ministry of Finance on further improving the direct settlement of basic medical insurance for cross-provincial medical treatment,” Gov.cn, June 30, 2022, https://www.gov.cn/zhengce/zhengceku/2022-07/26/content_5702881.htm; “How can I get direct reimbursement for medical treatment in a different province?,” National Healthcare Security Administration (Guójiā Yīliáo Bǎozhàng Jú), June 7, 2025, https://www.nhsa.gov.cn/art/2025/6/7/art_14_16754.html.
↩
148
Beijing Statistics, “Significant progress has been made in the health and wellness sector, and the people's health rights have been effectively protected—the 22nd in a series of reports on the economic and social development achievements of the People's Republic of China over the past 75 years,” The Paper (Péngpài Xīnwén), September 25, 2024, https://www.thepaper.cn/newsDetail_forward_28851266.
↩
149
Xiuli Wang and Jay Pan, “Assessing the disparity in spatial access to hospital care in ethnic minority region in Sichuan Province, China.” BMC Health Services Research 16, no. 399 (August 17, 2016), https://doi.org/10.1186/s12913-016-1643-8; Chaofang Yan et al., “Ethnic disparities in utilization of maternal and child health services in rural Southwest China.” International Journal of Environmental Research and Public Health 17, no. 22 (November 19, 2020):8610, https://doi.org/10.3390/ijerph17228610.
↩
150
Cuili Wang et al., “Health literacy and ethnic disparities in health-related quality of life among rural women: results from a Chinese poor minority area.” Health and Quality of Life Outcomes 11, no. 153 (September 11, 2013), https://doi.org/10.1186/1477-7525-11-153.
↩
151
Fang Luo et al., “Ethnic disparities and temporal trends in health resource allocation: a retrospective decadal analysis in Sichuan, a multi-ethnic Province of Southwest China (2009–2019).” BMC Health Services Research 24, no. 541 (April 27, 2024), https://doi.org/10.1186/s12913-024-11036-6.
↩
Xiaozhao Yousef Yang and Scott Schieman, “Racial disparities in death rates and death incidences in Xinjiang: a study of multilevel ecological mechanisms.” Social Science and Medicine 340 (January 2024):116405, https://doi.org/10.1016/j.socscimed.2023.116405; the number of deaths per household was calculated using the reciprocal of the average deaths per household reported.
↩
Yizhou Xu, “The individuals’ awareness and adoption of electronic health records in China: a questionnaire survey of 1,337 individuals.” BMC Public Health 24, no. 905 (March 27, 2024), https://doi.org/10.1186/s12889-024-18423-y.
↩
Explore how countries compare on key health system characteristics including health care coverage and spending, the health workforce, health outcomes, and more.