Israel’s National Health Insurance Law ensures universal coverage for all citizens and permanent residents. Citizens and residents choose from four competing nonprofit health plans that provide a mandated benefits package, known as the “health basket.” The compulsory insurance system is funded primarily through a national income tax and additional government funding.
Most citizens and residents purchase voluntary health insurance to cover medications not covered by the health basket and to gain faster access and greater provider choice. The health care system is overseen by the Ministry of Health; health plans are responsible for providing health care.
While the health system offers universal coverage, ongoing challenges — including long wait times for elective procedures, workforce shortages, and infrastructure gaps — contribute to broader concerns about equitable access, particularly for marginalized groups.1 For example, health indicators, such as life expectancy and infant mortality, are consistently lower among Palestinian citizens of Israel. Disparities are even greater for Palestinians living in the occupied territories of the West Bank, East Jerusalem, and Gaza, where a blockade is enforced by Israel.2 Under international law, Israel is obligated to ensure access to health care in territories under its effective control.3
Israel’s National Health Insurance (NHI) Law introduced universal health care for all citizens and permanent residents by creating a more sustainable, efficient public system that delivered care based on medical need rather than ability to pay.
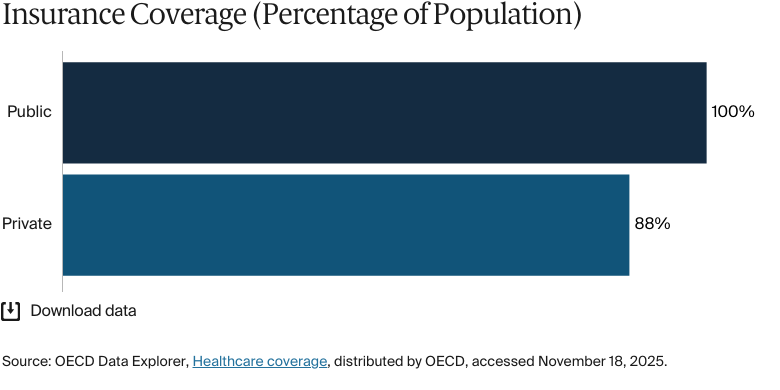
Public insurance coverage: 100% of population
Private insurance coverage: 88% of adult population
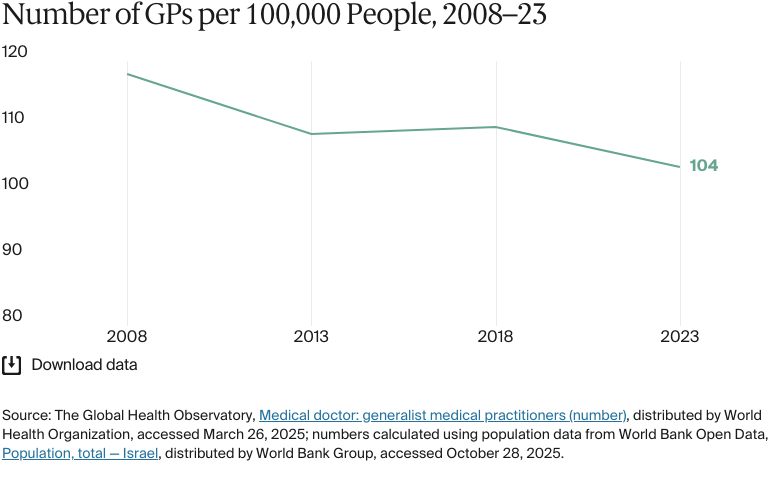
Primary care physicians: 104 per 100,000 people
Specialist physicians: 255 per 100,000 people
In 2024, total health expenditure was NIS 146 billion (USD 39.4 billion), an increase from NIS 127.3 billion (USD 34.4 billion) in 2021. Government spending (65%) was the largest source of health expenditure, followed by out-of-pocket spending and prepaid private spending.
Pharmaceutical spending: 12.9% of total health care budget
Out of pocket spending: 19.9% of total health care spend
There are significant disparities in health care outcomes between Jewish Israelis and Palestinian citizens of Israel. Life expectancy is one indicator of these disparities.
There are also health disparities across socioeconomic groups. A 2023 report found that individuals from lower socioeconomic backgrounds were more likely to experience high blood pressure and diabetes. Since 2019, obesity rates among women in this group have also increased. The gap between public and private health care deepens inequities. People who can afford private insurance receive faster and more comprehensive care, while those reliant on the public system often face delays.
By the mid-1970s, access to health care in Israel was provided by four health maintenance organizations (Kupot Holim) — Clalit, Maccabi, Meuhedet, and Leumit.4 Clalit was affiliated with Histadrut, the dominant labor federation in Israel from the 1920s to the early 1990s, while Maccabi Healthcare Services was introduced in 1940 to provide a less bureaucratic model that preserved physician autonomy and allowed patients to choose doctors and institutions.5
By the late 1980s, long wait times and financial instability led to public pressure for reform, culminating in the 1995 National Health Insurance (NHI) Law.6 The law introduced universal health care for all citizens and permanent residents and formally separated health coverage from political or union affiliation.7 The NHI Law also restructured the system, requiring the four health funds to compete with one another as regulated, nonprofit health plans that are responsible for delivering a standard package of services.8
The NHI Law aimed to ensure access to health care for all permanent residents by creating a more sustainable, efficient public system that delivered care based on medical need rather than ability to pay.9
The Role of Public Health Insurance
The Ministry of Health (Misrad HaBri'ut) regulates and funds the health care system, but the four health plans are responsible for providing care.10 The plans are legally required to provide a standardized package of essential health care services known as the “health basket” (Sal HaBri'ut), designed to ensure citizens and residents can access a comprehensive range of health services.11 The health basket is updated annually based on recommendations of the Public Committee for the Expansion of the Basket.12 Health plans also offer optional insurance for additional services and a broader choice of providers (see The Role of Private Health Insurance).13
NHI is funded by a dedicated health tax set at a fixed percentage of individual income, along with additional government funding.14 These funds are distributed to health plans based on membership size and demographic composition.15
There are two rates for the health tax. For salaried employees and self-employed individuals, the first rate, which covers the portion of monthly income up to 60 percent of the average wage, is 3.2 percent. The second rate, applying to income above the 60 percent threshold, is 5.2 percent.16
The NHI Law aimed to reinforce financial and health care equity by mandating universal coverage, prohibiting health plans from denying coverage to applicants, and implementing a risk-adjusted capitation system. While NHI covers most people, soldiers and prisoners are insured under separate systems or private plans. These groups made up about 2 percent of the population as of 2021.17
Jewish immigrants to Israel (olim) — including those granted citizenship under the Law of Return, returning minors, and Israeli citizens born abroad and immigrating for the first time — are entitled to public health coverage upon arrival, provided they register with a health fund.18 In contrast, Israeli citizens returning after extended stays abroad must reestablish residency with the National Insurance Institute before regaining eligibility for public health insurance, or they must pay a reentry fee to avoid a waiting period.19 B1 visa holders, asylum seekers, undocumented migrants, and foreign workers are excluded from NHI and rely on private insurance or publicly funded emergency services.20
Pharmaceuticals (only certain medications as listed in the health basket)
Dental care (only for children under age 18 and for older adults age 72 and over)
Eye care (partial coverage)
Mental health care
Palliative care
Rehabilitative care
Home visits
Assistive devices (partial coverage).
Copayments are required for most outpatient specialist visits, emergency care without referral, outpatient imaging, prescribed medicines, and medical products. There are caps in place for specialist visits, diagnostic imaging, and medications for chronic conditions (see Safety Nets).22
Adults age 72 and over are eligible for free or reduced-cost dental care.23 In general, adult dental care is paid out of pocket or through optional private insurance.24
Children age 7 and under are eligible for one free pair of glasses per year.25 Some eye surgeries for conditions such as cataracts are covered but need to be approved by the health plan. Some health plans offer up to 50 percent off the cost of glasses and contact lenses.26
Assistive devices are not fully covered, but financial aid is available for eligible patients.27
Safety Nets
Some population groups are eligible for exemptions from paying health insurance contributions. These groups include housewives, children, prisoners, organ donors, some soldiers, new immigrants and those in national service.28
Some pensioners are exempt from paying health tax or pay a reduced rate. Those below retirement age pay 3.2 percent on the portion of their pension that does not exceed 60 percent of the average wage and 5.2 percent on the portion that does. Widows receiving a survivor’s pension or a benefit because of a family member’s work-related death are exempt, as are individuals receiving a disability pension.29
Unemployed individuals pay the minimum health insurance contributions of NIS 120 (USD 32)..30Olim(see The Role of Public Health Insurance) are exempt from paying health insurance contributions for the first six months after arrival or up to 12 months if they receive a living allowance from the Ministry of Aliyah and Integration. Payment of contributions begins once this exemption period ends.31 Children of refugees, asylum seekers, and undocumented migrants receive the same benefits as resident children, provided their parents pay this minimum contribution.32
Many groups are exempt from copayments for medications listed in the health basket, or they are eligible for reduced rates. These include patients with chronic conditions (such as cancer and HIV/AIDS), Holocaust survivors, groups receiving income support (such as World War II veterans), organ donors, and some pensioners.33
Specialist appointments require copayments, which are billed quarterly. The groups listed above, as well as children under age 18, are exempt from paying these quarterly fees. Victims of traffic or work accidents are exempt or are refunded for treatment received for their injuries.34
The Role of Private Health Insurance
Private health insurance operates alongside the public health care system, covering services and benefits that are not included in the health basket. These services include adult dental care, private hospital rooms, and shorter wait times for specialist appointments.35
Supplemental insurance is provided by health plans.
Commercial insurance is provided by for-profit private insurers.
Supplemental insurance is regulated by the Ministry of Health. Health plans cannot reject applicants, and premiums are based solely on age. Although supplemental insurance covers services beyond NHI coverage, it does not cover medications that aren’t in the health basket.37
Commercial insurance tends to be more comprehensive, individually tailored, and expensive. Premiums are primarily determined by age and gender, and policies can be either collective or individual.38
Many residents choose dual coverage (both supplemental and commercial insurance) to enhance their health care access.39 In 2022, 88 percent of adults had dual coverage..40
The Role of Government
The health care system is managed centrally by the Ministry of Health, which is responsible for policymaking, regulation, planning, and service provision.41 The National Insurance Institute, meanwhile, collects health insurance funds and distributes them to the health plans.42
Several government bodies contribute to health care governance and oversight:
The National Health Councils manage resource constraints and advise the Ministry of Health on medical policies, prevention, and treatment strategies to ensure that health care decisions align with medical advancements.43
The Israel National Institute for Health Policy Research facilitates discussions on health policy, funds research on health care economics and quality, and assesses the impact of the NHI Law.44
Integration and Care Coordination
One strength of the Israeli health system is its advanced health information exchange, which connects primary care providers, specialists, and hospitals to enable efficient data sharing. The exchange of information is particularly beneficial for managing chronic and complex conditions, as it ensures patients receive continuous, coordinated care across health care settings.45
To further enhance care integration, health plans have implemented targeted care management programs that use videoconferencing, sophisticated information systems, and other technologies to improve patient monitoring and coordination.46
One example of these initiatives is the Maccabi Transitional Care Program, launched in 2015 to improve transitions from hospital back into the community. Specially trained nurses assess post-hospitalization needs and connect patients with appropriate community-based care. This program helps to reduce hospital readmissions and maintain continuity of care.47
Operations and Resources
Overview of the Delivery System
Israel’s health care system is structured into three levels of care:48
Primary care is the backbone of the system, delivered by a mix of general practitioners (GPs) and other specialists, and free at the point of use.
Specialist care is mainly provided in community settings by self-employed physicians and is subject to copayments.
Hospital care covers emergencies, imaging, diagnostic treatments, and inpatient care — the latter is free at the point of use.
The public health care system is centrally regulated and universally funded. The Ministry of Health oversees policy, planning, and regulation, while the four health plans deliver and pay for services. Coverage is mandatory for all residents under the NHI, with funding collected through income-related health taxes and general government revenues. These funds are pooled by the National Insurance Institute and distributed to the health plans using a risk-adjusted formula.49 The Knesset Finance Committee regulates these payments to maintain affordability and manage overall health care costs.50
Primary Care
Primary care services are fully covered under NHI, with copayments applying only to specialist visits. Patients receive primary care through one of the four competing nonprofit health plans, which employ or contract with primary care physicians, including GPs, family medicine specialists, and pediatricians.51 GPs are most commonly reimbursed through weighted capitation, which requires at least one patient visit per quarter, with no extra payments for additional visits.52
The four NHI health plans (Clalit, Maccabi, Meuhedet, and Leumit) have different approaches to organizing care. Clalit, the largest health plan, provides most primary care in clinics it owns and operates, and GPs are salaried employees. Clalit also contracts with independent physicians, many of whom provide services from Clalit’s own facilities, where they can purchase logistical support, such as nursing services, from the fund. The other three health plans rely heavily on independent physicians to provide primary care services.53
Salaries of Clalit clinic-based physicians are set via a collective bargaining agreement with the Israel Medical Association.54
Clalit and Leumit use predominantly passive capitation, a monthly per-member payment made regardless of whether the member visited the GP. Leumit also uses this model, but to a much lesser extent. Meuhedet uses a quarterly visit-based payment model for independent physicians, in which doctors are paid for each member’s first visit per quarter. Maccabi primarily uses per-visit (fee-for-service) payment for independent physicians. Across all plans, independent physicians also receive limited fee-for-service payments for certain procedures.55
Patients have unrestricted access to their primary care physicians through their chosen health plan, and appointments are generally easy to schedule.56 While physicians are not required to provide out-of-hours care, this care is supported by 24/7 call centers staffed by nurses and operated by all four health plans. These centers offer guidance on various illnesses and symptoms.57
In 2023, there were 104 GPs for every 100,000 people in Israel. This is fewer than in Portugal and Switzerland, which are comparable in size and had 303.5 and 115 GPs for every 100,000 people, respectively, in 2022.58 As of 2024, about 35 percent of GPs in Israel were self-employed, and 65 percent were employed by health plans.59
In terms of funding and strategic focus, Israel places much greater emphasis on primary care than hospital care.
The Israeli health care system, unlike most other systems, is by and large a primary-care-focused and community-care-focused system.
Ran Balicer
Deputy Director General and Head
Innovation Division at Clalit Health Services
More broadly, preventive service use has declined across the entire population since the COVID-19 pandemic, which is limiting early detection and chronic disease management. Since then, screening rates for body mass index, blood pressure, smoking, and hemoglobin levels have fallen across all age groups, and the sharpest decline is among children and people from lower socioeconomic groups. To strengthen health promotion and reduce disparities, the Ministry of Health has been promoting health units and health-focused planning in seven regional clusters, along with targeted initiatives in Arab, Druze, and Circassian communities.60
Outpatient/Specialist Care
Specialized ambulatory care is predominantly provided in community settings, with hospitals increasingly expanding their outpatient departments to accommodate these services.61 Specialist care involves fixed copayments, but to limit the financial burden on patients, there’s a capped limit on copayments for outpatient specialist visits (see Safety Nets).62
In 2023, there were 255 specialists for every 100,000 people, which is below the 2022 figures for Portugal (280.6) and Switzerland (275.2).63 There are no current data for the proportion of specialists employed publicly versus privately.
The medical workforce is aging, with 44 percent of specialist doctors age 67 and over and nearing retirement. Although the number of specialists per capita increased by 3.4 percent increase since 2010, a large share is nearing retirement (see Physician Education and the Workforce).64 This aging workforce is contributing to persistent gaps in specialist access. Wait times for specialist consultations are an issue. For example, in the first quarter of 2024, the average national wait time for an endocrinologist or neurologist was 50 days.65
Physician Education and the Workforce
The physician-to-population ratio is below the OECD average, and the physician workforce is aging. About 40 percent of physicians are age 67 or over, suggesting that a retirement wave is looming.66
Another issue is the growing adoption of commercial insurance, which reimburses private providers at higher rates than the four health plans do, drawing health care workers away from public facilities. This has worsened workforce shortages in the public system and limited access to care.67
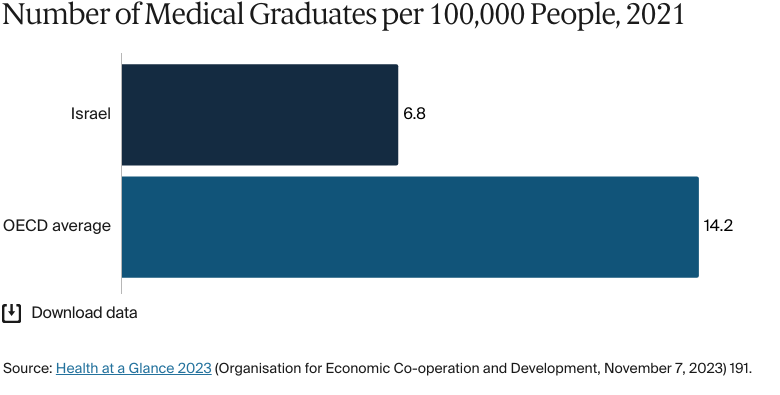
The small number of medical graduates further exacerbates the problem. In 2023, there were 7.2 medical graduates for every 100,000 people, up from 6.8 in 2021 but still far below the 2021 OECD average of 14.2.68 Historically, Israel has relied on foreign-trained physicians to meet demand, with more than half of its doctors earning their degrees abroad. In 2023, only 30 percent of newly licensed physicians were graduates of Israeli medical schools, and just 42 percent of practicing physicians were trained domestically.69
In 2022 and 2023, 1,240 physicians immigrated to Israel from abroad, helping to sustain the health care workforce. Over half (56%) of these physicians emigrated from Russia.70 To raise medical education standards, however, a reform introduced in 2019 will disqualify foreign medical schools that don’t meet World Federation for Medical Education standards. Set to take full effect in 2026, the policy is expected to limit the recognition of many foreign medical degrees.71 In 2024, the Committee for Immigration, Absorption and Diaspora Affairs said that this could create a 40 percent shortage in the number of physicians.72
The Ministry of Health has announced several strategies to address the workforce shortage. These include expanding and regulating clinical training sites, which are hospital-based facilities where medical students gain hands-on clinical experience; launching a strategic workforce planning body; and shifting residency training to community-based programs. The goal is to boost the number of new medical students each year to 2,000 by 2030.73
There are five undergraduate medical schools.74 It typically takes between four and six years to get a medical degree. After graduating, all medical students must complete a one-year internship to qualify for a practicing license and to pursue a postgraduate residency. Residency training enables doctors to specialize, and it takes an additional four to seven years, depending on the specialty. Typically, it takes nine to 11 years to become a fully trained medical specialist.75
For the 2022-2023 academic year, an undergraduate medical degree cost around NIS 11,000 (USD 2,972) and a graduate degree cost around NIS 15,000 (USD 4,053).76
675 nurses and midwives per 100,000 people in 2023.78
Patients can choose between public and private hospitals, depending on their insurance coverage. Public hospitals are government-funded and provide free care with a referral, while private hospitals receive mixed funding and require supplementary insurance, commercial insurance, or out-of-pocket payments.79
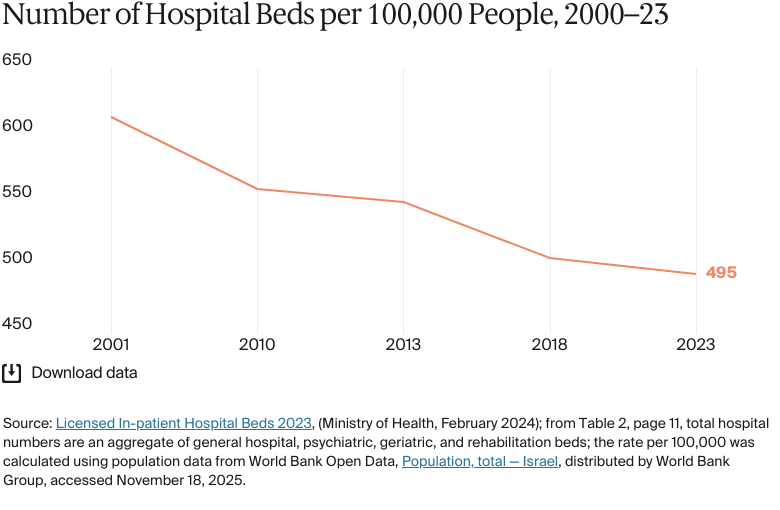
In 2023, there were 495 hospital beds for every 100,000 people, above the 2021 OECD average (430).80 The Ministry of Health owns and operates 45 percent of acute care beds in general hospitals, as well as numerous long-term care and psychiatric facilities. Other stakeholders in the ownership of general acute care beds include Clalit (30%) and nongovernmental organizations (22%), while the rest (3%) are owned by Maccabi and other private for-profit entities that manage private hospitals.81
The Ministry of Health published a hospital bed plan in 2023 to reduce gaps, shorten wait times — especially for mental health services — and improve accessibility and care quality. The plan includes adding 1,790 general beds, 300 rehabilitation beds, and 245 psychiatric hospital beds by 2028.82
Nursing shortages are ongoing. In 2023, there were 659 nurses for every 100,000 people, well below the European average of 826 in 2022 (see Physician Education and the Workforce).83
Public hospitals sell services to health plans, and payment methods and prices are regulated by the Ministry of Health. Public hospitals operate under an activity-based payment system using the procedure-related group model, which categorizes payments by procedure rather than diagnosis. Additional payments apply for multiple major procedures on different organs and elective surgeries performed outside regular hours.84
Public hospitals are subject to two income limitations. The first is a capping mechanism through which the Ministry of Health sets annual revenue limits from each health plan for each hospital. These caps include both a minimum guaranteed payment and a maximum reimbursement limit; both are formally reviewed and adjusted every three years. The second limitation involves contracts negotiated between individual hospitals and health plans, which can replace the cap arrangement. These contracts often include customized discounts.85
Mental Health Care
BY THE NUMBERS
16 psychiatrists per 100,000 people in 2021 (compared with 18 across OECD countries)86
The mental health care system is governed by the Rehabilitation Law (2000). This law facilitates the rehabilitation and community integration of individuals with mental health disabilities, providing access to a basket of rehabilitation services, including housing, employment, education, rehabilitative support, family assistance, and dental care.88
Access to mental health care varies across population groups. This is especially true for Palestinian citizens of Israel who largely reside in segregated and underserved areas (see Addressing Health Inequities), leading to higher rates of psychological distress.89 A study in 2020 found that 60.5 percent of women in this group suffered from anxiety, compared to 42.1 percent of Jewish Israeli women.90
As with many other areas of the system, workforce shortages lead to long wait times as the system struggles to meet the growing demand for mental health care.91 In 2021, there were 104 mental health practitioners for every 100,000 people, below the OECD average of 123.92 This shortage is mainly a result of psychologists choosing to work in the private sector.93
The shortage of workers has been particularly acute since the start of the war in the Gaza Strip in 2023.94 The proportion of individuals suffering from stress, depression, and post-traumatic stress disorder increased by an average of 16 percentage points between August and November of that year.95 The health plans launched a number of initiatives to address this.96 Clalit, for instance, introduced a new role, resilience coach, to provide short-term practical support to individuals experiencing emotional distress.97
More generally, the government implemented reforms to expand mental health services, funded by an increase in the health tax (see The Role of Public Health Insurance).98 The funds support a program to hire therapists within the public health care system. Services will be enhanced across health plans, mental health facilities, and resilience centers. The program includes establishing multidisciplinary clinics to provide integrated care, improve access to psychological services, and support the needs of health care organizations and the entire health system.99
Long-Term Care and Social Support
The National Insurance Institute oversees community-based long-term care, while the government finances institutionalized care. This fragmented system, involving the National Insurance Institute, the Ministry of Health, and the Ministry of Welfare and Social Affairs, has led to overlapping responsibilities and coordination issues.100
Clalit Health Services’ Ran Balicer says that this approach is particularly harmful for elderly care. “Elderly care in Israel is fragmented, with different agencies responsible for different stages of need,” says Balicer. “As a person’s condition worsens, responsibility shifts from one body to another — often abruptly. This creates gaps in care and coordination. Unlike other parts of the health system that are well integrated, such as mental health care, elderly care lacks that continuity. It’s a longstanding issue that hasn’t yet been resolved.”
Institutional long-term care is generally the financial responsibility of the patient and their family, but government subsidies are available on a sliding-scale basis. Community-based services are supported through the Long-Term Care Insurance Law and include personal care support, housekeeping, and access to day-care centers. Eligibility is based on disability and income, but income thresholds are high enough that most elderly individuals who meet clinical criteria qualify.101
Despite this, family members frequently contribute both financially and through unpaid caregiving. As such, informal caregivers play a central role in supporting individuals living with chronic illnesses, disabilities, or mental health conditions.102
A 2018 reform expanded long-term care benefits to informal caregivers, aiming to alleviate their financial burden.103 By the end of 2023, the number of older adults receiving long-term care benefits had nearly doubled since 2018, from 180,000 to 346,000. The National Insurance Institute primarily funds in-home caregivers. About 30,000 patients receive out-of-home care — mainly in nursing homes regulated by the Ministry of Health or retirement homes overseen by the Ministry of Welfare and Social Affairs.104 Overall, 4.1 percent of elderly individuals reside in long-term care institutions; the rest receive care at home.105
In 2022, long-term care expenditure reached NIS 23.6 billion (USD 6.4 billion). Of this, 71 percent came from public spending and 29 percent came from private spending. Most of the funds supported community care, and the rest was allocated to long-term care hospitalization and nursing facilities.106
Cost and Affordability
Health Care Spending Overview
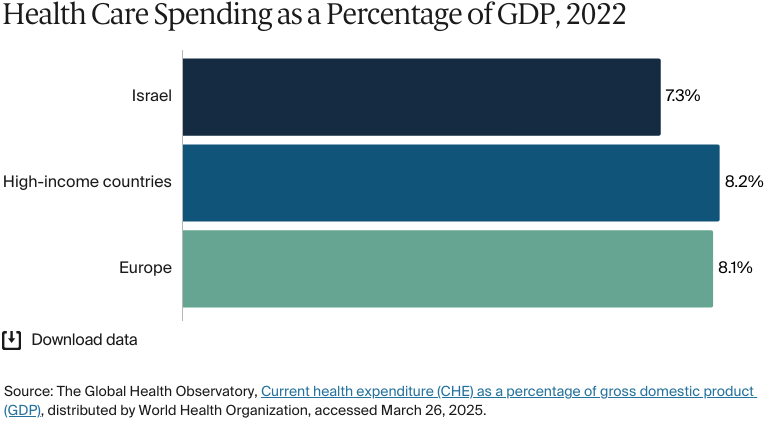
Health care spending has returned to pre-COVID-19 levels, when it peaked at 8.4 percent of gross domestic product (GDP) in 2020.107 In 2024, health care spending as a percentage of GDP was estimated at 7.3 percent, similar to 7.5 percent in 2003.108 However, this is still below the average for high-income countries and Europe (8.1%).109
In 2024, total health expenditure was NIS 146 billion (USD 39.4 billion), an increase from NIS 127.3 billion (USD 34.4 billion) in 2021. The expenditure per capita (USD 3,941) was well below the Western European average (USD 5,200) and the average across high-income countries (USD 5,930).110
In 2024, government spending (65%) was the largest source of health expenditure, followed by out-of-pocket spending (19.9%) and prepaid private spending (13.7%).111
Pharmaceutical Spending
In 2022, 12.9 percent of total health expenditure was spent on pharmaceuticals. Pharmaceutical spending per capita was USD 405 per year, lower than that for Portugal (USD 561) and Switzerland (USD 955).112 Pharmaceuticals are sold by a mix of health plan-owned and independent pharmacies, and plans encourage patients to choose generic medications.113
Patients make percentage-based copayments for pharmaceuticals: 10 percent of the maximum consumer price for generic drugs and 15 percent for branded drugs, based on prices set by the Ministry of Health. In both cases, there is a minimum charge of NIS 18 (USD 5).114
To manage pharmaceutical expenses, the Ministry of Health strictly regulates drug prices, which it negotiates directly with drug manufacturers.115 The Ministry of Health sets maximum prices based on the three lowest prices from a pool of seven reference countries.116
The national health basket covers a wide range of medicines, which keeps out-of-pocket costs low for patients.117 In 2024, the Ministry of Health mandated a 3.6 percent reduction in the maximum prices of 1,500 prescription drugs.118 Drugs outside the basket require special approval — in February 2025, the Public Committee for the Expansion of the Healthcare Services Basket recommended the introduction of 117 medications and technologies focused on preventive medicine and chronic conditions.119
Cost Sharing and Out-of-Pocket Spending
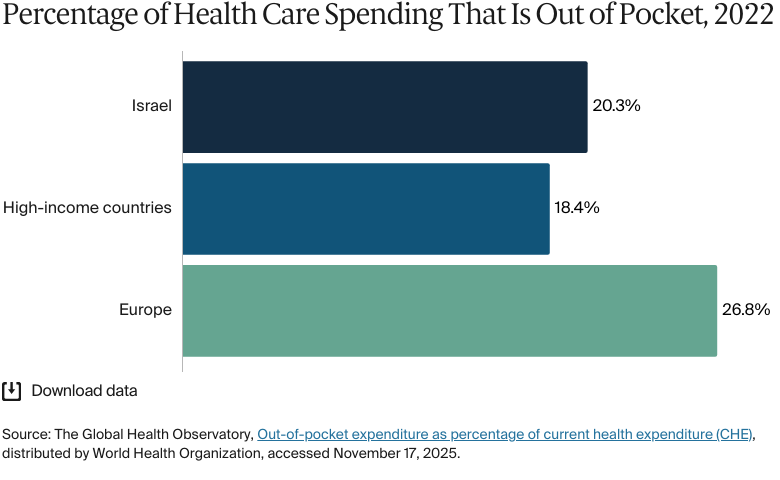
In 2024, out-of-pocket spending accounted for 19.9 percent of total health care expenditure, below the level for Europe (26.8%) but above that in high-income countries (18.4%).120
In 2022, the annual average out-of-pocket health care expenditure per person reached NIS 2,375 (USD 642), a significant increase from NIS 1,632 (USD 441) in 2005. Dental care was the largest contributor, accounting for 38 percent of these expenses, followed by outpatient medications (23%), medical products (18%), and outpatient care (19%). Spending on inpatient care and diagnostic tests was minimal — just 3 percent of total out-of-pocket payments.121
Pediatric, gynecologic, and internal medicine specialist visits are covered under NHI, but other specialist visits require a copayment of NIS 22–35 (USD 6–10) for the first visit in each quarter.122
Emergency visits without referral also require copayments of NIS 94.2 (USD 25.5) for community visits, NIS 217 (USD 59) for hospital visits between 01:00 and 06:00, and NIS 911 (USD 246) for hospital visits between 06:00 and 01:00.123
There are no data for the percentage of the population that has been pushed below the poverty line by health care costs. However, in 2022, five percent of households experienced catastrophic health spending and 2 percent were impoverished or further impoverished by out-of-pocket payments. In 2021, unmet health care needs due to financial constraints affected 11 percent of adults, rising to 19 percent for individuals in the poorest quintile.124
How Are Costs Contained?
Drug price regulation and preventive care initiatives are the main focus of efforts to control expenditure (see Pharmaceutical Spending). For example, hospital-at-home services are expected to be delivered within global budgets. Under the reform, providers that fail to expand these services face a 1 percent budget reduction.125
The cost-containment strategy also prioritizes preventive care to reduce long-term health care expenses. The Healthy Israel 2020 initiative promotes chronic disease management, tobacco and alcohol regulation, and public health education to curb the incidence of costly medical conditions. Well baby clinics provide essential maternal and child health services, including vaccinations and developmental support, and district health offices oversee infectious disease control and food safety.126
Quality and Outcomes
Health Outcomes
BY THE NUMBERS
Average life expectancy was 81.7 years in 2021 (compared with 79.7 years across high-income countries).127
The avoidable mortality rate was 134 deaths per 100,000 people in 2022.128
Malignant neoplasms (cancer): 122 deaths per 100,000 people
Heart diseases: 68 deaths per 100,000 people
COVID-19: 46 deaths per 100,000 people.
The maternal mortality rate was three deaths per 100,000 live births in 2023 (compared with 11 on average across Europe).130
The infant mortality rate was 3 deaths per 1,000 live births in 2023 (compared with an average of 7 across Europe).131
In 2021, the share of the population with mental health disorders was 15 percent (compared with an average of 16% in high-income countries).132
The suicide rate was 6 per 100,000 people in 2023, lower than the average of 12 per 100,000 people across high-income countries.133
The gun death rate was 2 deaths per 100,000 people in 2023.134
23 percent of adults were affected by obesity in 2022.135
Women live longer than men. In 2023, their average life expectancy was 85.5 years, compared with 81 years for men.136
Noncommunicable diseases were the leading cause of death in 2021, accounting for 76.9 percent of all deaths. Communicable diseases and maternal, perinatal, and nutritional conditions contributed to 19 percent of deaths, and injuries accounted for the remaining 4.1 percent.137
Addressing Health Inequities
There are significant disparities in health care outcomes between Jewish Israelis and Palestinian citizens of Israel. Life expectancy is one indicator of these disparities. In 2024, for Arab populations, the highest regional average life expectancy (in the north) was 80.1 years, compared with a regional high for Jewish and non-Arab individuals of 84.3 years (in Tel Aviv).138 Health inequities affecting Palestinian citizens extend beyond overall longevity. In 2020, neonatal mortality was 2.6 times higher among Palestinian citizens than among Jewish Israelis, with even higher disparities in the South (3.6 times higher). Additionally, a study in 2023 found that the towns with the highest mortality rates (both overall and from heart disease) were entirely inhabited by Palestinian citizens.139
In 2021, the Ministry of Health started implementing measures to address health inequities affecting the Arab community, focusing on issues such as mental health, early years, and lung disease, as well as creating health units in underserved areas. At the time of writing, the results of these initiatives are unclear.140
Health inequities in the occupied Palestinian territories
Under international law, Israel is responsible for the health of people living in the occupied territories.141 However, severe disparities exist, especially for Palestinian citizens of Israel. Making up 20 percent of Israel’s population (as of 2021), Palestinian citizens of Israel are individuals of Palestinian descent who remained within the borders of the state of Israel after its establishment in 1948 and hold Israeli citizenship today. These citizens struggle to access care, partly due to physical barriers. In 2020, more than 90 percent of Palestinian citizens of Israel were found to be living in segregated localities, far from health care services, which are mostly concentrated in Jewish Israeli towns.142
These factors contribute to lower use of care and worse health outcomes. A 2023 study reported that Jewish Israelis are twice as likely to use preventive care than Palestinian citizens.143 In 2021, the infant mortality rate in the occupied territories was 12 deaths for every 1,000 live births, whereas in Israel, it was three deaths for every 1,000 live births. Mortality for children under age 5 was also several times higher in the occupied territories: 14 for every 1,000, compared with four for every 1,000 in Israel. Adults ages 30 to 70, meanwhile, had an 18 percentage point higher risk of dying from noncommunicable diseases than their counterparts in Israel.144
The occupied territories face high rates of unemployment (44% in the Gaza Strip and 14% in the West Bank as of 2022), food insecurity, and poor living conditions that contribute to ill health. Access to clean water and sanitation is also impeded, particularly in disadvantaged areas.145
Physical and administrative barriers further hinder access to health care. A 2023 U.N. assessment found that more than half of “fixed movement” obstacles (339 of 645) severely restricted Palestinian’s access to main roads and essential services, including health care facilities.146
Access to health care is also shaped by a fragmented system of identity documentation. Palestinian residents of East Jerusalem who hold Israeli-issued permits are covered by Israel’s public health insurance. In contrast, Palestinians with West-Bank- or Gaza-issued permits rely on the Palestinian health system and must apply for permits to access hospitals in East Jerusalem or Israel.147 In 2022, 15 percent of permit applications by patients in the West Bank who were seeking care in East Jerusalem or Israeli health facilities were not approved by the time of the scheduled appointment. Additionally, 93 percent of ambulance transfers to East Jerusalem were delayed due to the “back-to-back” procedure, where patients are transferred from a Palestinian- to an Israeli-licensed ambulance at checkpoints.148
As of June 2025, ongoing hostilities in Gaza had resulted in 55,000 reported deaths; widespread damage to medical infrastructure, with 94 percent of hospitals affected; and significant restrictions on the entry of humanitarian aid, including food, fuel, and medicine.149 In 2024, the United Nations reported the deaths of more than 1,000 health workers and the detention of hundreds more.150
There are also health disparities across socioeconomic groups. A 2023 report found that individuals from lower socioeconomic backgrounds were more likely to experience high blood pressure and diabetes. Since 2019, obesity rates among women in this group have also increased. However, from 2019 to 2022, women from upper-middle socioeconomic backgrounds were more likely to smoke than those from lower-income groups.151
The gap between public and private health care deepens inequities. People who can afford private insurance receive faster and more comprehensive care, while those reliant on the public system often face delays.152 In 2021, the Ministry of Health found that health care providers spent 2.3 times more time on privately insured individuals in Jewish and mixed towns than in non-Jewish towns. The Decade Committee for Reducing Health Inequality, a government committee set up to establish a strategy to reduce health inequity by 2030, recommends setting shared and measurable targets, improving health care access in underserved areas, and integrating health services within local authorities.153
Regional disparities in health outcomes reflect underlying socioeconomic patterns. Infant mortality rates in the Southern region, for instance, are especially high: in 2024, the likelihood of death during the first year of life was 2.8 times greater than in the Central region. These gaps are shaped not only by income but also by reduced access to health care infrastructure. In 2022, the number of hospital beds was about two for every 1,000 people in both the Southern and Northern Districts, below the national average of 2.6. By contrast, Tel Aviv and the Haifa Districts had the highest availability, with 3.4 and 3.7 beds for every 1,000 people, respectively. A similar pattern appears in the distribution of health care professionals.154
Financial incentives have been designed to encourage health care professionals to work in rural areas. In 2018 and 2019, specialists in these regions received grants that were more than 60 percent higher than those of their counterparts in central Israel.155
As of 2024, there were language assistance programs and orientation sessions to help immigrants navigate the health care system and access essential services. These initiatives collectively aim to reduce health inequities and improve outcomes for marginalized populations.156
Innovation and Reform
Health Care Innovation
The most notable recent health care reforms have focused on standardizing private health insurance. In 2023, a reform by the Capital Market, Insurance and Savings Authority consolidated all private health insurance policies into five tiers to simplify coverage options. All insurers must offer a basic Tier 1 package that includes transplants, overseas specialized treatments, and drugs not covered by public health insurance. Higher tiers cover surgeries at private clinics, outpatient care, and additional medical services, such as critical illness coverage.157
Before 2024, individuals could enroll in one of the two private health policies, either “First Shekel” or a supplemental insurance plan, meaning that they often paid twice for similar coverage. In 2024, an amendment was introduced to automatically transfer individuals with the more expensive First Shekel to one of the more affordable supplemental plans. The aim is to reduce household health care expenses by about NIS 1,300 (USD 351) per year while ensuring the same medical services and streamlining health care financing.158
Health Care Technology
Israel has made significant public and private investments in its digital health sector.159 By 2030, it aims to integrate big data and advanced analytics into health care to enhance personalized medicine and improve patient outcomes.160 Big data refers to large volumes of health information collected over time — such as electronic medical records, lab results, and genetic data — while analytics involves using algorithms and statistical tools to identify patterns and make predictions from this information. Big data is already being used for early disease detection, such as for colorectal cancer, and sensor-based monitoring is enabling home hospitalization, which can cut costs and improve patient recovery.161
Under the Medical Information Mobilization Law — 2024 patients will be able to give permission for their medical information to be shared between health care providers on a dedicated platform. It’s hoped that providing physicians with quicker access to patient information can lead to better, more personalized care while allowing patients to choose how their medical information is shared.162 The legislation is expected to come into force in July 2027.163
This content was produced by FT Longitude, the specialist research and content marketing division of the Financial Times Group, on behalf of the Commonwealth Fund. Research and content for the Commonwealth Fund country profiles were collected by FT Longitude between February and December 2025.
This profile reflects data as of January 2026. New or updated information may have become available since its release.
Osama Tanous et al., “Structural racism and the health of Palestinian citizens of Israel.” Global Public Health 18, no. 1 (May 20, 2023):2214608, https://doi.org/10.1080/17441692.2023.2214608; Yazid Barhoush and Joseph J Amon, “Medical apartheid in Palestine. Global Public Health 18, no. 1 (April 23, 2023):2201612, https://doi.org/10.1080/17441692.2023.2201612.
↩
3
Barhoush and Amon, "Medical apartheid in Palestine."
↩
Yoel Angel et al., “Adapting the Israeli national health insurance law to the 21st century — a report from the 19th Dead Sea Conference,” Israel Journal of Health Policy Research 10 (January 5, 2021):1, https://doi.org/10.1186/s13584-020-00432-y.
↩
Lior Beres, “Health insurance in Israel for B1 visa holders,” The Israeli Association for International Couples, last updated April 23, 2025, https://aic.org.il/health-insurance-for-b1-partner-visa-holders/; World Health Organization, Health Systems in Action: Israel, 2024.↩
Daniel K Rotenberg et al., “Similarities and differences between two well-performing healthcare systems: a comparison between the Israeli and the Danish healthcare systems.” Israel Journal of Health Policy Research 11 (February 28, 2022):14, https://doi.org/10.1186/s13584-022-00524-x.
↩
State Comptroller of Israel and Ministry of Health, Regulation of Clinical Training for Doctors.
↩
77
Information Division, Medical Technologies Division, Information and Research, Hospital beds and licensed positions; from Table 4 on page 12, the figure is an aggregate of general hospital, psychiatric, geriatric, and rehabilitation beds.
↩
78
Ministry of Health, Manpower In the Health Professions, 140.
↩
79
World Health Organization, Health Systems in Action: Israel, 2022.↩
80
Information Division, Medical Technologies Division, Information and Research, Hospital beds and licensed positions; from Table 4 on page 12, the figure is an aggregate of general hospital, psychiatric, geriatric, and rehabilitation beds; Organisation for Economic Co-operation and Development, Health at a Glance 2023.
↩
81
World Health Organization, Health Systems in Action: Israel, 2022.↩
Ministry of Health, Manpower In the Health Professions, 140; World Health Organization, Density of nursing and midwifery personnel (per 10,000 population, distributed by WHO Data, accessed October 29, 2025, https://data.who.int/indicators/i/B54EB15/5C8435F.
↩
84
Ruth Waitzberg et al., “The 2010 expansion of activity-based hospital payment in Israel: an evaluation of effects at the ward level.” BMC Health Services Research 19, no. 292 (May 8, 2019), https://doi.org/10.1186/s12913-019-4083-4.
↩
85
Waitzberg et al., “The 2010 expansion of activity.”
↩
Nihaya Daoud et al., “Residential segregation, neighborhood violence and disorder, and inequalities in anxiety among Jewish and Palestinian-Arab perinatal women in Israel.” International Journal for Equity in Health 19, no. 218 (2020), https://equityhealthj.biomedcentral.com/articles/10.1186/s12939-020-01339-5.
↩
91
World Health Organization, Health Systems in Action: Israel, 2024.↩
92
Organisation for Economic Co-operation and Development, A New Benchmark for Mental Health Systems; note: figures were derived for mental health practitioners by adding the total for psychiatrists, psychologists, and mental health nurses as presented in Table 1.3.
↩
Yossi Levi-Belz, et al.“PTSD, depression, and anxiety after the October 7, 2023 attack in Israel: a nationwide prospective study.” eClinicalMedicine, 68 (February 2024):102418, https://doi.org/10.1016/j.eclinm.2023.102418; note: the average was calculated from the percentage differences in the shares of people suffering from PTSD, generalized anxiety disorder, and depression.
↩
95
Levi-Belz, et al. “PTSD, depression, and anxiety”; note: the average was calculated from the percentage differences in the shares of people suffering from PTSD, generalized anxiety disorder and depression.
↩
96
World Health Organization, Health Systems in Action: Israel, 2024.↩
Ministry of Health, “Expanding the workforce of the mental health care center,” GOV.IL, last updated March 27, 2024, https://www.gov.il/en/pages/recruitment-mental-health-team; Health Systems and Policy Monitor (HSPM), “Progressive rise in NHI contributions.”
↩
International Long-Term Care Policy Network (LTC), “LTCcovid country profile.”
↩
104
Chen Mashiach, “Long Term Care in Israel” (Press Release, Taub Center for Social Policy Studies in Israel, April 2, 2024), https://www.taubcenter.org.il/en/pr/ltc/.
↩
105
J Brodsky et al., “Geriatric health care to the elderly in Israel.” Archives of Gerontology and Geriatrics 35, no. Suppl. 8 (2022):59–73, https://doi.org/10.1016/S0167-4943(02)00105-X.
↩
Fishman and Eini, “National Expenditure on Health, 2024.”; Central Bureau of Statistics, National Expenditure on Health 1962–2021; Institute for Health Metrics and Evaluation, Financing Global Health, distributed by IHME, accessed October 29, 2025,https://vizhub.healthdata.org/fgh/.
↩
111
Fishman and Eini, “National Expenditure on Health, 2024,” Note: government spending includes health tax and government budget; prepaid private spending includes households’ private insurance, private nonprofit institutions, and other private bodies.
↩
Ministry of Health, “The Price of prescription drugs has reduced by an average of 7.47%,” GOV.IL, last updated February 13, 2023, https://www.gov.il/en/pages/27122022-05.
↩
Ministry of Health, “Decrease in the maximum price.”
↩
119
Ministry of Health, “The Public Committee for the Expansion of the Healthcare Services Basket for the year 2025 concluded discussions and submitted its recommendations to the Minister of Health,” GOV.IL, last updated February 11, 2025, https://www.gov.il/en/pages/06022025-01.
↩
Elliot Rosenberg et al., “Healthy Israel 2020: Israel’s blueprint for health promotion and disease prevention.” Public Health Reviews 35, no. 1 (June 11, 2013), https://doi.org/10.1007/BF03391690.
↩
The Global Health Observatory, Maternal Mortality, distributed by World Health Organization, accessed January 21, 2026, https://www.who.int/data/gho/data/indicators/indicator-details/GHO/maternal-mortality-ratio-(per-100-000-live-births);Max Roser and Hannah Ritchie, “Maternal mortality,” Our World in Data, February 2024, https://ourworldindata.org/maternal-mortality.
↩
“Suicide Rate by Country 2026”,World Population Review, accessed January 21, 2026, https://worldpopulationreview.com/country-rankings/suicide-rate-by-country
↩
134
Institute for Health Metrics and Evaluation, GBD Results, distributed by IHME, accessed October 29, 2025, https://vizhub.healthdata.org/gbd-results/. Overall firearm mortality is the aggregate of physical violence by firearm, self-harm by firearm, and unintentional injuries by firearm.
↩
135
World Health Organization, Age-standardized prevalence of obesity among adults (18+ years), distributed by WHO Data, last updated February 29, 2024, https://data.who.int/indicators/i/C6262EC/BEFA58B.
↩
World Health Organization, Health data overview for the State of Israel, distributed by WHO Data, accessed November 25, 2025, https://data.who.int/countries/376.
↩
Ministry of Health, “Interim recommendations of the Decade Committee for Reducing Health Inequality and the Health Inequality and Its Management Report for 2021,” GOV.IL, last updated February 7, 2023, https://www.gov.il/en/pages/14112022-02.
↩
Iranian Thalassemia Society, “Attacks on Health Facilities in the Gaza Strip and the Violation of International Humanitarian Law,” (Written Statement, United Nations General Assembly, March 18, 2024), https://apps.who.int/gb/ebwha/pdf_files/WHA76/A76_15-en.pdf.
↩
145
Director General, Health Conditions in the Occupied Palestinian Territory, Including East Jerusalem, and in the Occupied Syrian Golan (World Health Organization, May 17, 2023) https://apps.who.int/gb/ebwha/pdf_files/WHA76/A76_15-en.pdf (accessed May 15, 2025).
↩
146
“Movement and access in the West Bank | August 2023,” United Nations Office for the Coordination of Humanitarian Affairs, August 15, 2023, https://www.ochaopt.org/2023-movement.
↩
147
Director General, Health Conditions in the Occupied Palestinian Territory.
↩
148
United Nations Office for the Coordination of Humanitarian Affairs, “Movement and access in the West Bank.”
↩
Davidovitch and Lev, The Healthcare System in Israel.↩
155
Eyal Jacobson and Vered Ezra, “Financial incentives as a governmental tool to bridge the medical manpower gap between Israel’s center and periphery.” Israel Journal of Health Policy Research 8, no. 74 (October 14, 2019), https://doi.org/10.1186/s13584-019-0344-2; note: the percentage was calculated using grants listed for periphery versus center in Table 1.
↩
“Israel Life Sciences and Health-Tech Industry Report for 2024-25” (Press Release, Israel Innovation Authority, March 3, 2025), https://innovationisrael.org.il/en/press_release/israel-life-sciences-and-health-tech-industry-report-for-2024-25/.
↩
Ministry of Health, “The Medical Information Mobilization Law passed today in the Health Committee ahead of second and third readings in the Knesset,” GOV.IL, last updated July 15, 2024, https://www.gov.il/en/pages/12072024-03.
↩
Explore how countries compare on key health system characteristics including health care coverage and spending, the health workforce, health outcomes, and more.