Background and History
The origins of the modern health insurance system can be traced to the end of World War II. With medical facilities considerably damaged, health authorities focused on improving public health in the years that followed. They introduced more than 10 public insurance programs, each covering a particular group, such as government employees, farmers, and low-income households.
While this system improved health outcomes, it was fragmented, and just 59 percent of the population had coverage prior to 1995. In 1986, the government began a shift to a universal program. The planning process, which involved studying health insurance systems abroad, led to the merging of the various public insurance programs under a single-payer system.
The National Health Insurance (NHI) Planning Team was established by the Department of Health in 1991, followed by the NHI Act in 1994 and the NHI system in 1995. Subsequent reforms that were designed to make health care more financially sustainable and accessible led to the implementation of the Second-Generation NHI in 2013.
The Role of Public Health Insurance
Enrollment in NHI is mandatory for all citizens. At the end of 2023, 100 percent of the population was insured under the system.
The system is funded mainly through premiums paid by insured individuals, employers, and the government. The balance of revenue comes from supplementary premiums levied on non-payroll income, which were introduced under the Second-Generation NHI. This non-payroll income includes large bonuses (those exceeding four times the employee’s salary), rent, interest, dividends, professional fees, and income from second and third jobs. Other sources of supplementary premiums include additional government premium subsidies, tobacco taxes, and taxes on lottery gains.
The contribution ratio is based on the insured person’s monthly income. Premium contributions are capped at four members per household (the insured person plus three dependents). Any additional household members are covered at no cost. Caps and thresholds apply to payroll-based and supplemental premiums.
There are copayments for accessing medical services, which vary by service type, provider, and individual circumstances (see Cost Sharing and Out-of-Pocket Spending).
Services Covered by Public Health Insurance
NHI benefits are uniform and comprehensive. They include:
- Inpatient care
- Outpatient care
- Dental care
- Traditional Chinese medicine
- Pharmaceuticals
- Maternity care
- Primary care
- Eye care
- Rehabilitative care
- Palliative care
- Mental health care
- Long-term care
- Preventive care
- Home visits
- Assistive devices.
NHI doesn’t cover eyeglasses or medical equipment, such as wheelchairs and hearing aids, but it does cover costly cochlear implants for children. People who need wheelchairs or artificial limbs can apply for government subsidies under the People with Disabilities Rights Protection Act, while veterans who need hearing aids or artificial limbs can receive them free of charge at veterans’ hospitals.
Safety Nets
The government offers a range of assistance measures for people unable to cover the cost of their premiums, as well as for those working in specific professions or suffering from chronic illness or injury.
The government provides 100 percent premium subsidies for low-income households, military personnel, unemployed veterans, unemployed workers and their dependents, people with physical and mental disabilities, and unemployed native citizens under age 20 and over age 55.
Exemptions from outpatient copayments apply to childbirth and certain conditions, such as cancer, as well as some population groups, including residents of remote and mountainous areas and offshore islands, veterans and families of deceased veterans, low-income households, and children under age 3.
Others receive discounts on copayments. For example, outpatient copayments for people who have a disability certificate are limited to TWD 50 (USD 2). For patients in areas that lack medical resources, copayments are reduced by 20 percent.
Exemptions from drug copayments are given to patients with cancer or a chronic illness and to those who have received a major illness/injury certificate for any other serious condition. Finally, the National Health Insurance Administration (NHIA) waives copayments for all lifesaving drugs for people with rare diseases recognized by the Ministry of Health and Welfare (MOHW).
The government provides interest-free loans to people experiencing financial difficulty to help them cover their premiums and any unpaid copayments. In 2021, these loans totaled TWD 151 million (USD 5 million) distributed among 1,747 people.
The NHIA offers installment plans to people who owe premiums of more than TWD 2,000 (USD 62) and are not eligible for relief loans. In 2021, installment payment plans totaled TWD 2.3 billion (USD 72 million) and were paid across 70,000 cases.
The Role of Private Health Insurance
Private health insurance is supplementary to mandatory public health insurance. Private plans are offered by for-profit insurers, often as part of nonmedical insurance offerings such as life or car insurance. These don’t cover medical services already covered by NHI, nor do they buy faster access to, or a wider choice of, specialists. Instead, such policies offer disease-specific cash indemnity provisions. Policyholders can use this money to pay for private hospital rooms or devices, such as drug-eluting stents, that NHI does not cover.
There are no data available for private insurance uptake.
The Role of Government
The NHI program is administered by the NHIA, which falls under the MOHW. The NHIA is supported by six regional offices connected by a health information infrastructure. Local and municipal governments play little to no role in financing health care.
The bulk of NHI-covered services are provided through a predominantly private delivery system, although some hospitals are owned and operated by municipal governments.
The MOHW, which sets policy, determines how much the NHI global budget should grow each year (subject to approval by the premier’s office).
The NHIA’s main tasks include collecting premiums, pooling risk, and paying providers, as well as overseeing the utilization, expenditures, and quality of health services. The NHIA is also responsible for coverage decisions (based on the cost-effectiveness of new drugs and treatments), provider fee-setting and fee schedule adjustments, and cost containment.
Parliament plays an important watchdog role in all NHI matters. In addition to its role in negotiating any new health legislation, it must pass an amendment to the NHI Act for any premium rate increases above 6 percent.
Integration and Care Coordination
The Family Doctor Integrated Care Plan
Introduced in 2003, this community-based program seeks to improve access to continuous, comprehensive medical care. Community networks comprising five or more primary care physicians and one community hospital provide patient-centered primary care, including disease management, patient health education, and preventive care. Telephone consultations with family doctors are also available 24 hours a day for those enrolled in the program.
At the end of 2023, 5,590 primary care clinics (52.3%) and 7,807 physicians (45.4%) had formed 558 community health care networks serving more than 6 million people.
In 2024, the NHIA upgraded the program to include care programs for diabetes, early chronic kidney disease, and metabolic syndrome. It uses digital tracking management to monitor health conditions.
The Integrated Delivery System
The Integrated Delivery System (IDS) was introduced in 1998 to improve access to medical services and facilities in remote, underserved areas by increasing collaboration between large hospitals and local providers and introducing mobile specialist medical services. Over time, the IDS has gradually expanded to cover preventive health, community-based services, and chronic disease management.
Long-Term Care Plan 2.0
The Long-Term Care Plan 2.0 (LTC 2.0) was implemented in 2017 to support the aging population through a community care system that integrates home hospice care and home-based medical care (see Long-Term Care and Social Support).
The NHIA also supports care coordination by streamlining administrative processes. Its third-party payment mechanism, for example, handles medical expenses based on the NHI fee schedule, so physicians are not responsible for individual claims processing.
Despite these efforts, the health care system remains fragmented, partly because each health care institution receives payments based on its share of service volume. This fragmentation increases competition and disincentivizes collaboration between providers (see Overview of the Delivery System).
Overview of the Delivery System
The health care system comprises clinics, district hospitals, regional hospitals, and medical centers. These deliver three levels of care:
- Primary care is typically provided in clinics and district hospitals and is primarily responsible for monitoring and treating stable chronic diseases.
- Secondary care is provided in regional hospitals and offers a wider range of specialist services, inpatient care, and more advanced diagnostics.
- Tertiary care is typically provided in medical centers and offers highly specialized treatments, complex procedures, and advanced diagnostics.
Patients can access any level of health care directly without referral, but copayments incentivize patients to seek initial treatment at lower tiers, which reduces pressure on specialist facilities (see Cost Sharing and Out-of-Pocket Spending).
The NHI payment system relies on a third-party payment mechanism, with the NHIA paying hospital and clinic expenses according to the NHI fee schedule. The global budget payment system determines how financial resources are distributed across providers. Each year, the system sets a cap on the total available health resources for the sector, meaning that individual institutions receive payments based on their share of the total service volume. This system is efficient and effective at controlling costs from an administrative perspective, but it forces institutions to maximize volumes to ensure their financial stability.
Primary Care
Primary care is provided in clinics and district hospitals. Treatment is focused mainly on preventive care and the management of acute and chronic diseases.
There’s no referral system, and residents are not required to have their own general practitioner (GP). However, initiatives such as the Family Doctor Integrated Care Plan encourage residents to enroll with a regular doctor or clinic (see Integration and Care Coordination).
In 2024, there were 270 practicing physicians for every 100,000 people — a 29 percent increase from 2014.
Out-of-hours care is available at regional hospitals and medical centers, which are required to operate 24-hour emergency departments.
Physicians are paid predominantly on a fee-for-service basis according to national uniform fee schedules set by the NHIA with input from industry stakeholders. Other sources of income include patient registration fees, services and goods not covered by NHI, and copayments and coinsurance. Pay-for-performance programs offer additional financial incentives for doctors based on the standard of their care for certain diseases and conditions, including cancer and diabetes.
There are currently no data available for the number of practitioners employed publicly versus privately.
Outpatient/Specialist Care
Specialist care is provided in regional hospitals and medical centers. Care is typically accessed through primary care referral, self-referral, or hospital admission, depending on the severity of the patient’s condition.
There are currently no data available for the number of specialist medical practitioners or the proportion employed publicly versus privately.
Physician Education and the Workforce
There are both public and private medical schools, and the government limits admissions to 1,300 per year. In 2021, annual tuition fees at public schools totaled TWD 78,327 (USD 2,439), while fees at private schools totaled TWD 135,829 (USD 4,298).
While early specialty training is prioritized, including general medical practice in the initial years of residency, gaps in family medicine education remain. Only nine of the 13 medical schools, for instance, have dedicated family medicine departments.
International students can access a range of scholarship options. The Ministry of Education has a scholarship program which pays up to NTD 40,000 (USD 1,273) each semester for tuition fees and expenses.
The average salary for doctors depends on their specialty and experience. Typically, it falls in the range of TWD 1.2 million (USD 37,363) to TWD 3 million (USD 93,408) a year. Attending physicians work an average of 69.1 hours per week.
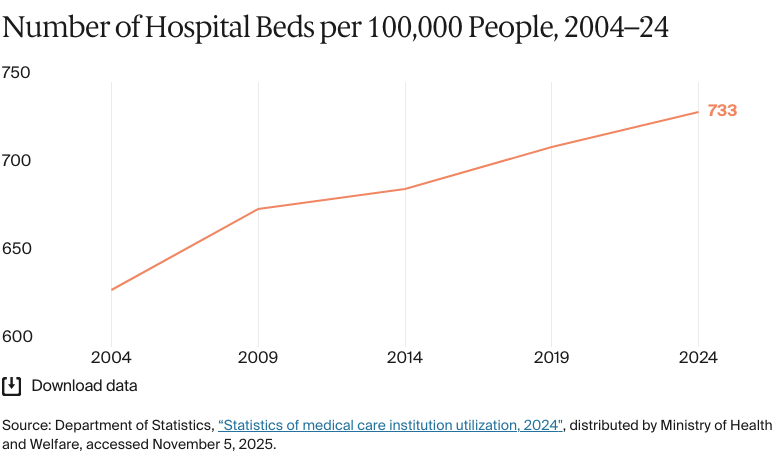
Hospitals