Our Scorecard ranks every state’s health care system based on how well it provides high-quality, accessible, and equitable health care. Read the report to see health care rankings by state.
The Perils and Payoffs of Alternative Payment Models for Community Health Centers
Toplines
Population-based payments helped sustain some FQHCs during the pandemic as they curtailed in-person services and invested in telehealth and other tools.
To transition to alternative payment models, many FQHCs will require technical assistance, culture change, and better collaboration with other providers and health plans
Toplines
Population-based payments helped sustain some FQHCs during the pandemic as they curtailed in-person services and invested in telehealth and other tools.
To transition to alternative payment models, many FQHCs will require technical assistance, culture change, and better collaboration with other providers and health plans
In October 2021, the Center for Medicare and Medicaid Innovation (CMMI) announced a goal of having every Medicare beneficiary and the majority of Medicaid beneficiaries covered by some type of alternative payment model (APM) by 2030. CMMI considers APMs to be any arrangements whereby providers are held accountable for the quality and costs of care, not just paid based on the volume of services they deliver. The agency also pledged to promote health equity by making it easier for providers serving racial and ethnic minorities to participate in APMs.
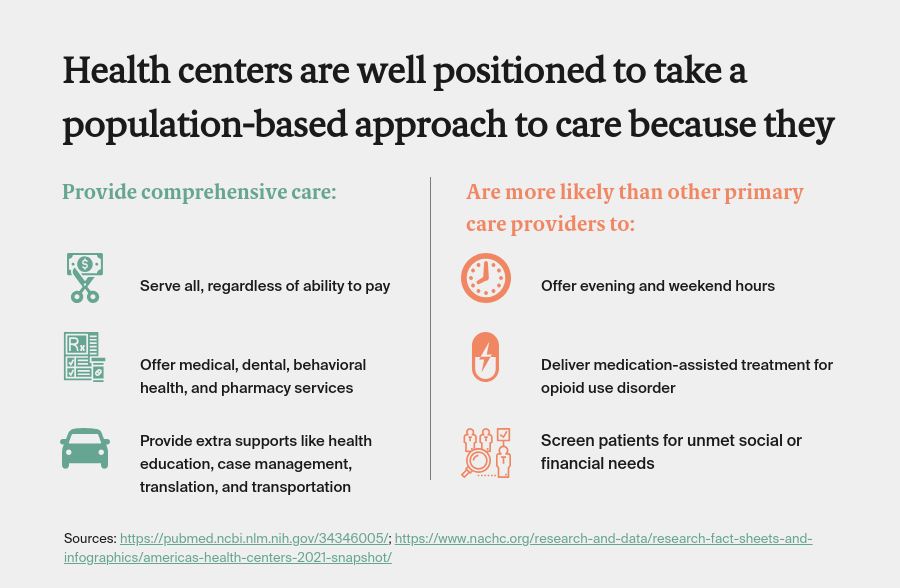
Community health centers, or federally qualified health centers (FQHCs) — the1,400 safety-net clinics that provide care to all, regardless of their ability to pay — are often not considered in the design of APMs, even though they provide care to one in six Medicaid beneficiaries and several million Medicare beneficiaries. This is in part because health centers have a unique payment model. Since 2000, Medicare and Medicaid programs have paid FQHCs through a prospective payment system (PPS) that provides a bundled rate for all primary care visits, regardless of the type or intensity of services provided. The PPS was intended to shore up FQHCs’ financing by accounting for the additional services health centers provide to what are often high-need patients. But many say the payment approach is no longer sufficient because it hasn’t kept up with health centers’ costs and it only covers in-person visits offered by clinicians. “The current model doesn’t reflect the fact that the nature of care has changed nor does it account for patients’ complexity, the magnitude of poverty, and the roles of trauma and the social determinants of health,” says Andie Martinez Patterson, senior vice president of strategy, integration, and system impact at the California Primary Care Association.
In recent years, some FQHCs have begun dipping their toes into alternative payment approaches, joining programs run by their state Medicaid agencies, Medicaid managed care organizations, or Medicare. Per federal rules, health centers can join any type of APM so long as: 1) their participation is optional and 2) their payment for delivering primary care services is not less than it would have been under PPS reimbursement. This means that FHQCs are allowed to take financial risk for other services, and some have — entering into contracts that attribute patients to their health centers, give them capitated payments, and hold them responsible for patients’ costs for specialty care, acute care, and other services beyond their clinics.
In this issue of Transforming Care, we profile FQHCs that are participating in a range of APMs. Many have been able to do so by leveraging state and federal funds for health system transformation, including Delivery System Reform Incentive Payment (DSRIP) funds. Health centers have also banded together to build the data analytics and other tools needed to manage population health.
Advanced APM Programs
Yakima Valley Farm Workers Clinic
Yakima Valley Farm Workers Clinic, which has 42 clinics serving 200,000 patients in Oregon and Washington State, got involved in APMs as a way of expanding its capacity to serve patients with complex needs, including the uninsured. Both Oregon and Washington have introduced APMs for FQHCs. Oregon’s program was the first in the nation; it started with a pilot in 2013 and now involves 18 of the state’s 32 health centers. Washington State followed suit, introducing an APM in 2017 that now involves 17 of the state’s 27 health centers.
Oregon’s and Washington’s APMs are similar: health centers receive capitated payments for each assigned Medicaid beneficiary (per member per month, or PMPM) and additional payments to cover care management activities. Portions of the payments are adjusted based on health centers’ performance on five measures, which are changed each year. In Oregon, Medicaid providers are paid through regional coordinated care organizations, while in Washington, FQHCs still contract with Medicaid managed care organizations (MCOs). In addition, Yakima for several years has participated as an accountable care organization (ACO) in Medicare’s Shared Savings Program. In all, about 130,000 of its patients are covered by some type of APM.
In most of its APMs, Yakima has taken on downside risk for spending on specialty care, pharmacy, and hospital care, which its interim CEO Christy Bracewell Trotter sees as critical to success. The investment has paid off: in a given year, Yakima’s additional revenue from quality incentives and shared savings can be upward of $10 million — a substantial segment of Yakima’s $250 million operating budget, according to Bracewell Trotter.
The additional revenue from the APMs has enabled the FQHC to build new facilities and offer extra services for all its patients, including the 47,000 who do not have health insurance. To manage patients’ chronic conditions and help them avoid complications, Yakima has hired clinical pharmacists as well as physicians, diabetes educators, and nurses. It also runs a mail-order pharmacy and brings specialists, including cardiologists, to see patients at their clinicsand enables providers to have electronic consults with specialists at any time.
The APMs helped the FQHC weather the financial challenges COVID presented. “We didn’t suffer cash flow problems because we were getting our PMPM on a regular basis,” Bracewell Trotter says.
Toppenish Medical Dental Center is one of 42 clinics Yakima Valley Farm Workers Clinic operates in Oregon and Washington. Before the pandemic, it often held community health fairs with a focus on the needs of seasonal and migrant farmworkers.
Source: https://www.youtube.com/watch?v=eGzYxVaDe_o
Mosaic Medical
Mosaic Medical is an FQHC serving 27,000 patients in 15 clinics in Central Oregon, including those in rural communities as well as the city of Bend. It has been part of Oregon’s APM since 2013. Like Yakima Valley, Mosaic has taken on some downside financial risk — albeit more limited — for its 16,000 attributed Medicaid patients.
Mosaic Medical fields a mobile outreach team to provide care to individuals experiencing homelessness and at-risk youth. The team travels to shelters, food banks, and other locations. Pictured here are Mosaic’s mobile outreach coordinator, Casey Sadahiro; Kerry Gillette, a physician assistant; and Galina Asher, a medical assistant.
Photo credit: Mosaic Medical
According to CEO Megan Haase, F.N.P., shifting away from visit-based payment has necessitated “lots of culture work.” Among other changes, care team members have had to learn that patient care can happen beyond the exam room. “The construct of a traditional, in-person visit is so hard-wired in primary care, that it’s a learning curve to let go of that and do things differently and make sure you’re still providing value,” Haase says. The state requires Mosaic and other health centers to track the various ways in which they support patients, known as “care steps.” These steps “could be a MyChart message from a clinician, or a community health worker connecting a patient to housing assistance, as well as clinical services that may not be billable, like a nurse helping a patient fill out a health questionnaire,” says Marshall Greene, M.S., director of value improvement.
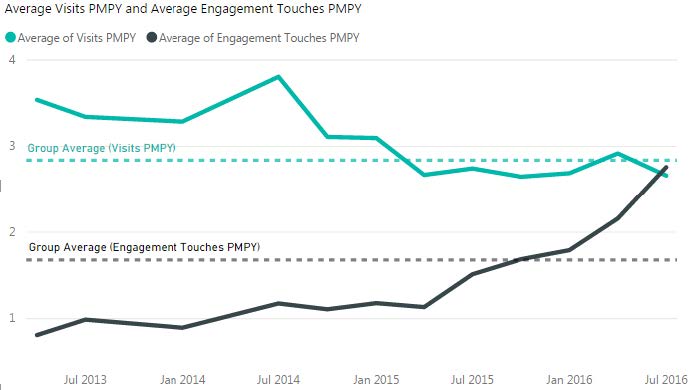
Across Oregon, since the adoption of alternative payment for FQHCs, the number of medical visits to health centers has declined while the number of engagement touches or “care steps” — including supports to help patients understand their medical conditions and navigate the health care system — has increased.
Source: Health Management Associates.
Note: PMPY = per member per year.
Since 2014, care teams have had access to clinical pharmacists, who work with patients with conditions like hypertension or diabetes to review their medications and make sure they understand how to take them. And community health workers now use a standardized tool to screen patients for unmet social needs and track their progress in helping them find supports.
In recent years, Mosaic was able to increase preventive screenings and chronic care management. From 2018 to 2019, the number of patients whose diabetes was under control increased from 73 percent to 80 percent. And last year, Mosaic mailed colon cancer screening kits to any patients who were overdue for these screenings, contributing to a 10 percent increase in the number completing the test from the previous year. During the pandemic, Mosaic also offered drive-up vaccinations, blood draws, and blood pressure checks. “We had the financial stability to pivot and function in a new way,” Haase says.
AltaMed Health Services
AltaMed Health Services is the nation’s largest independent FQHC, serving more than 354,000patients, the majority of them Hispanic/Latino, across 43clinics in Los Angeles and Orange counties. About 17 percent of patients are uninsured. Over the past several years, AltaMed’s leaders have increasingly embraced APMs and taken on greater financial risk for the costs of patients’ specialty and acute care.
In 1996, AltaMed launched the first Program of All-Inclusive Care for the Elderly (PACE) in Southern California, assuming full financial risk for patients 55 and older who are deemed to need nursing home–level care. Through 11 sites, the program provides medical care, meals, day care, and transportation to 3,600 patients.
In 2008, AltaMed created an independent practice association (IPA) to enable the health center to take on risk for primary care and better coordinate primary care, specialty care, and hospital use for its patients. The IPA now carries full risk to manage the medical care of 80,000 Medicaid patients covered by the MCO L.A. Care. The contract covers primary and specialty care services, as well acute and postacute care (behavioral health services and pharmacy are carved out). AltaMed shares in some portion of the capitated payments the IPA receives from L.A. Care and receives PPS wraparound payments from the state. “Going into these full-risk contracts allows us to reinvest some of those dollars to holistically take care of patients,” says Efrain Talamantes, M.D., AltaMed’s chief operating officer. “Under the old payment model, if the patient isn’t seen within the four walls, we don’t get paid.”
Among other efforts, AltaMed has hired promotores de salud (community health workers) who, along with clinicians, make home visits to support patients with heart failure, chronic obstructive pulmonary disease, and diabetes. Staff also offer health education classes and help patients manage transitions from hospitals or other care settings. Like Yakima Valley, AltaMed occasionally brings in specialists to meet with patients with complex conditions such as heart failure, using the APM revenue to subsidize the cost.
Nurses from AltaMed Health Services, including Timmie Nichols, R.N., make home visits to vulnerable elderly patients to help manage their chronic conditions.
Photo: AltaMed Health Services
Banding Together
Community Care Cooperative
In some regions, FQHCs have banded together to build a critical mass of patients and leverage shared resources to participate in APMs. One such network is Community Care Cooperative, a group of 18 Massachusetts FQHCs including large health centers like East Boston Neighborhood Health Center and small health centers with just a few providers. The network formed in 2016 to launch the first Medicaid ACO led by FQHCs.
Community Care Cooperative received $19.8 million in startup funds from the state and federal government to pay for population health staff and software. This has enabled the ACO to build a system that tracks where patients are getting care by ingesting each health centers’ patient records and combining them with medical and behavioral health claims and data feeds on hospital admissions and emergency department visits. (Working directly with the state, instead of managed care organizations, has made this feasible.) The software also incorporates information on patients’ social circumstances garnered through care teams’ assessments, and stratifies each patient by their likely clinical risks. Community Care Cooperative then deploys field staff including community health workers to help patients make medical appointments, create care plans, and find social supports.
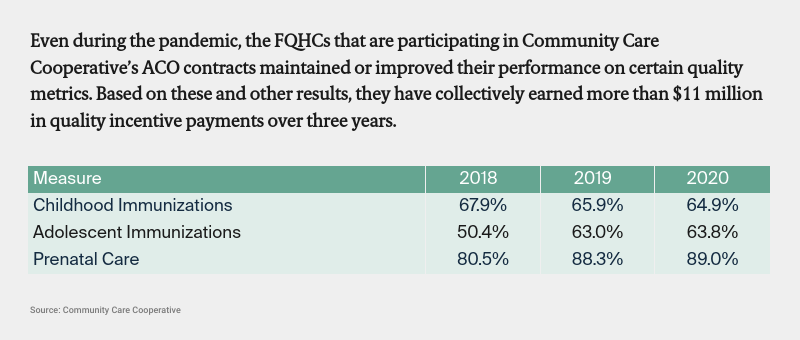
Today, Community Care Cooperative’s health centers care for 163,000 Medicaid beneficiaries. The cooperative contracts directly with the state to receive PMPM payments for these patients, which it distributes to member health centers. The health centers then receive shared savings or losses based on their performance on a set of quality metrics, as well as their attributed patients’ total costs of care, including behavioral health, specialty services, and hospital services (with some exceptions, e.g., for very high-cost drugs). This arrangement enables the health centers to take on varying levels of financial risk, depending on their financial reserves and comfort level. Total gains and losses are capped at 3 percent of the capitated budget. The ACO underwrites the whole enterprise and shares savings and losses with the state.
“We haven’t lost any money. We’ve either broken even or earned surplus each year,” says Christina Severin, M.P.H., president and CEO of Community Care Cooperative. Most important, she says, is what the ACO has helped practices do for patients: “Bringing together community health centers to share best practices has been very impactful on clinical practice.”
Banding together across FQHCs has also helped secure greater collaboration with hospitals, according to Severin.“In the past,it was difficult for our health centers to get the attention of hospitals,” she says. “But scaling them up and saying to hospital leaders, ‘We want to do business differently, and we have choices,’ has been really helpful.”
Severin estimates that half or more of the revenue the health centers will receive by January 2023 will be through an APM, whether through Medicaid, Medicare, or Blue Cross Blue Shield of Massachusetts, the state’s largest commercial insurer.
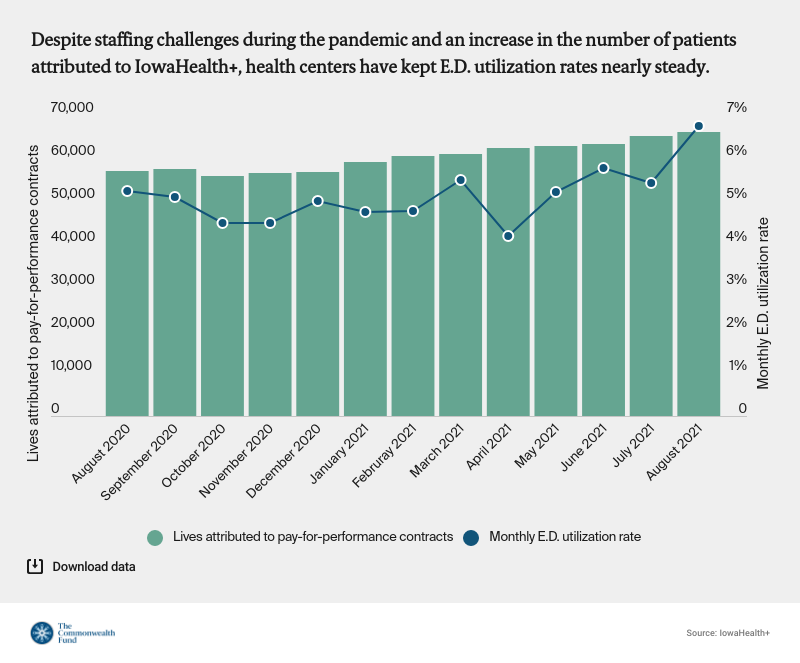
Iowa Primary Care Association
Another FQHC network formed in Iowa, where small and midsize FQHCs have come together under the auspices of the Iowa Primary Care Association. In 2012, the association spun off a company, IowaHealth+, to contract with payers on behalf of 11 health centers to advance value-based care and payment. The network is held accountable for health care quality and utilization measures and can earn pay-for-performance bonuses and/or shared savings for reducing the total cost of care on a per capita basis.
Aaron Todd, M.P.P., CEO of the Iowa Primary Care Association and IowaHealth+, says his members don’t have the capacity to take on risk on their own.“They’re too small and so they need to band together to spread risk,” he says.
The MCOs also provide upfront payments to IowaHealth+ so staff there can help health centers build capacity to manage population health. Health center staff receive hands-on support from process improvement coaches and meet regularly to share best practices. For example, to reduce unnecessary emergency department visits, health centers have expanded their hours and begun offering same-day appointments for urgent needs.
Thus far, the additional revenue from the APMs across the 11 health centers have been in the millions some years, according to Todd, and IowaHealth+ has not had any financial losses.
Providence Community Health Centers
Like FQHCs in Massachusetts, Providence Community Health Centers in Rhode Island is working under a state-led model to shift to APMs. With eight medical clinics and 60,000 patients, the health center serves one of every three residents of Providence, R.I., and the majority (70%) are Hispanic/Latino.
Since 2018, Providence has been one of the state’s accountable entities, which are similar to ACOs and aim to help primary care and other providers eventually assume responsibility for the health care outcomes and total costs of care for Medicaid beneficiaries. The accountable entities, which contract with Medicaid MCOs, earn incentives for achieving population health and utilization goals set by the state. Providence is one of seven accountable entities, of which four are led by FQHCs; the latter can but are not required to take on downside financial risk.
Since 2018, Rhode Island has also given Providence and other accountable entities funds from its Delivery System Reform Incentive Payment program. These funds, ranging from $1 million to $3 million a year for each accountable entity, support infrastructure projects selected by the providers in partnership with the state and its MCOs. The payments are contingent on meeting performance targets. The accountable entities must also commit to using 10 percent of the infrastructure dollars to establish partnerships with community-based organizations.
Providence Community Health Centers has used the infrastructure payments to test innovations, including a “fast pass” program that offers immediate appointments to patients who might otherwise go to the emergency department for non-urgent matters. It also piloted a diabetes management program to support patients with uncontrolled diabetes. And leaders have used some of the infrastructure payments to partner with organizations that place patients experiencing homelessness into housing and provide legal help to those struggling with landlords over services such as heat and water. “That’s one of the best outcomes of this whole thing. Those partnerships are now stronger,” says Merrill Thomas, M.B.A., Providence Community Health Centers’ CEO.
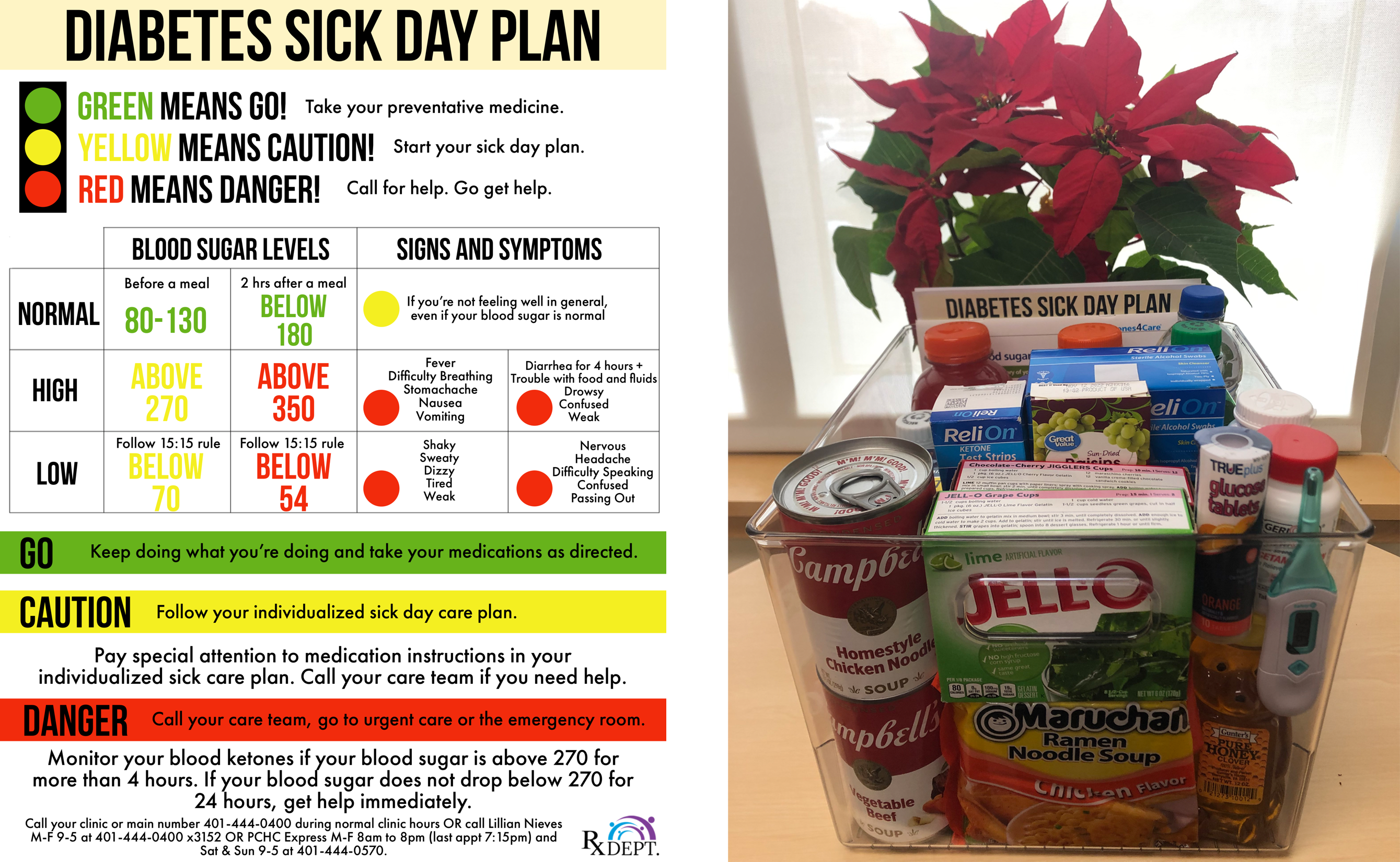
As part of a diabetes management pilot at Providence Community Health Centers, Lillian Nieves, Pharm.D., a bilingual clinical pharmacist and certified diabetes educator, teaches patients to have a “sick box” ready, stocked with sugar and non-sugar replacements as well as testing supplies, to help them manage fluctuations in their blood sugar levels. She creates an individualized “sick day” plan and helps patients experiencing problems adjust their medications. A pilot of the program involving 20 patients found participants had fewer emergency department visits, lower hemoglobin A1c levels, simpler medication regimens, and better blood pressure control in the six months following their engagement with the program.
Thomas says the shared savings component of the accountable entity program has been much less gratifying. The state has been slow to share data and has changed the parameters it uses to calculate savings, making it difficult to plan. Worse, it has asked MCOs to assign high-need patients, including those who need dialysis, patients with serious mental illnesses, and those with HIV/AIDS, to the accountable entity though the patients don’t use the FQHC for primary care. Staff conducted extensive outreach to find and engage patients who were “attributed but unseen” with minimal success. These assignments led to wild fluctuations in spending and the loss of any shared savings. “We feel like we’re playing against a stacked deck,” Thomas says. He says the FQHC will not assume downside risk with the state until these issues are resolved. But it is partnering with Neighborhood Health Plan of Rhode Island and United Healthcare Community Plan of Rhode Island to develop a special clinic for patients with multiple chronic conditions. Nurse case managers will be on site, along with a clinical pharmacist and a behavioral health specialist.
Providence has found greater financial success as part of an ACO in the Medicare Shared Savings Program. “We know that there’s potential when you coordinate care to bend the cost curve,” says Thomas.
Lessons
Like so many other areas of health care, COVID may be catalyzing change. During the pandemic, contracts that involve PMPMs or other fixed payments helped sustain some FQHCs as they curtailed in-person services and invested in telehealth and other tools. But shifting more health centers to APMs will require technical assistance as well as culture change, collaboration among providers, and customized payment models.
Shifting FQHCs to APMs may require a stepped approach.
Many of the health centers featured here received external supports — from the federal government, states, health plans, or health center networks — to participate in APMs.
Without such supports, FQHCs may struggle to develop the data analytics and financial forecasting tools needed to predict the cost of caring for populations with complex medical and social needs. “In many cases, they don’t have the capacity for it. They may have the staff with the skills to perform analytics, but not the resources to acquire software systems and hire dedicated staff to perform these functions,” says Rob Houston, M.B.A., M.P.P., director of delivery system and payment reform for the Center for Health Care Strategies.
Given variation in health centers’ resources and expertise, transitioning them to APMs may require a stepped approach that involves upfront funding for smaller FQHCs (or networks of them) and more flexibility for advanced FQHCs to run pilots and share lessons with others. “Without such support, a typical standalone health center with a $15 million budget that took on risk would be throwing their money to the winds of fate,” says Curt Degenfelder, a consultant who specializes in advising community health centers on strategy.
Some FQHCs are now being held accountable for health care costs as well as care quality and outcomes. Moving forward, it will be important to assess how new payment models are affecting racial disparities among their patients — and to reward approaches that promote health equity.
FQHCs need reliable partners.
In Rhode Island, Neighborhood Health Plan, which manages benefits for more than half of the state’s Medicaid beneficiaries, has worked with FQHCs including Providence Community Health Centers to help them reach population health goals. Founded by FQHCs, the health plan has helped finance nutrition programs for patients living in food deserts and purchased a sport utility vehicle as part of a mobile health initiative (paramedics use the vehicle to ferry patients to medical appointments in an effort to decrease unnecessary ED visits.) Both initiatives have produced cost savings. Neighborhood has also purchased data from Boston-based Algorex Healthcare Technologies to help identify members whose unmet social needs put them at risk for higher medical spending. “We’re giving the accountable entities the raw data such as claims and social determinants of health risk scores, as well as analysis on all of their patients, and we’re helping them learn how to use it,” says Beth Marootian, M.P.H., Neighborhood’s director of strategy and business development.
But in other respects, relationships with managed care organizations can be difficult, according to FQHCs. MCOs may take up to six months to credential new providers, compelling health centers to pay new hires without any means of billing for their services — even retroactively. Health plans may attribute people to health center contracts whom providers have never seen. Outreach campaigns to bring “attributed-but-unseen” Medicaid beneficiaries into primary care are notoriously unsuccessful. One strength of Oregon’s program is that it bases capitation rates on a health center’s existing patients, not health plan members. This approach may give providers confidence they are being held responsible for the care they’re actually providing.
To build effective partnerships, health plans and health centers need to agree on shared goals and a strategy for reaching them, a process that takes time and relationship building, says Aaron Todd of Iowa. “We need to find areas of agreement so we can work together,” he says. “It can be hard to get health plans to the table to do that.”
At minimum, Providence Community Health Centers would like to see payers acknowledge not all patients are willing and interested in traditional primary care despite providers’ best attempts to engage them. Meeting their preferences for urgent care rather than preventive care “requires a different reimbursement model and different expectations around quality,” says Jonathan Gates, M.D., the FQHC’s medical director of integrated care.
FQHCs need to be able to collaborate with other health care providers.
FQHCs’ success in lowering total medical costs hinges in part on helping patients access specialty care services that are outside the scope of what FQHCs are authorized to provide. Finding specialists willing to treat Medicaid beneficiaries is not easy in some communities, and FQHCs may also find it hard to partner with hospitals to improve care transitions. Oregon’s Medicaid program is structured to promote collaboration. Mosaic Medical for example works closely with the local hospital and other members of the Central Oregon Health Council, a coordinated care organization, to integrate care for Medicaid beneficiaries. The health council promotes transparency around contracting, encouraging hospitals and medical and behavior health providers to reach agreement on how Medicaid payments will be divided to achieve community health goals. To align incentives, the hospital shares the savings that are achieved by reducing hospitalizations with outpatient providers, including Mosaic Medical.
Payment models must cover all patients.
Large health centers like AltaMed have taken a portfolio approach to APMs, gradually shifting into contracts that hold them accountable for their Medicaid, Medicare, and dually covered patients. But such an approach leaves out the uninsured, forcing health centers to rely on grant funds and additional revenue from APMs to meet their needs. “The uninsured still tend to be left out of the conversation when it comes to rethinking payment,” says James Sinkoff, deputy executive officer and chief financial officer of Sun River Health, the largest FQHC in New York State with 245,000 patients; 25 percent of patients are uninsured. Sun River, which already serves as a Medicare ACO, is developing plans to take financial risk for Medicaid patients and participate in PACE. But leaders say it would help to have custom payment models for their uninsured patients, many of whom are migrant farm workers or homeless. “We’d really like to see the Health Resources and Services Administration use quality incentives to improve outcomes for these groups. We could offer them care management services, including specialist coordination, with a more flexible model,” says Anne Nolan, Sun River Health’s CEO.
Moving Forward
Achieving a cohesive, multipayer approach to FQHC payment that brings down spending will require greater cooperation among providers, payers, and policymakers. But many who have worked closely with FQHCs says it’s worth the investment.
“Primary care is really the backbone of an efficient health care system,” says Neighborhood’s Marootian. “There is an opportunity to take a deep breath post-COVID and spend some time thinking about how to change payment to alter the way primary care is delivered.”
Publications of Note
The Financial Burden of COVID-19 Looms Large for Patients
In a commentary in the Journal of the American Medical Association, three faculty from Vanderbilt University School of Medicine recommend a variety of interventions to protect patients with COVID-19 and long COVID from medical debt once the public health emergency is lifted and other provisions that make testing and care accessible to the uninsured are discontinued. Already nearly all major insurers have reinstated cost-sharing provisions for COVID-19 treatment. Hospitals receiving support from the federal Provider Relief Fund have been prevented from billing patients out-of-network rates; once the relief payments are exhausted, out-of-network charges may become common in surge regions, the authors say. John A. Graves, Khrysta Baig, and Melinda Buntin, “The Financial Effects and Consequences of COVID-19: A Gathering Storm,” Journal of the American Medical Association 326, no. 19 (November 2021):1909–10.
Requiring Drug Companies to Prove the Value of Experimental Cancer Drugs
In a commentary in the Journal of the American Medical Association, Richard G. Frank, Ph.D., and Ezekiel J. Emanuel, M.D., Ph.D., suggest that the Center for Medicare and Medicaid Innovation test a new model of paying for cancer drugs that receive accelerated approval from the U.S. Food and Drug Administration. The approach is designed to restrain prices for drugs that have been approved for use to treat serious or life-threatening illnesses until their manufacturers demonstrate they yield a clinical benefit. Under the model, payments for medications approved under the accelerated pathway would be randomized, with half reimbursed at 76 percent of the average sale price of already approved drugs and the other half receiving the prevailing payment under Medicare Part B. Once clinical trials establish a meaningful clinical outcome (e.g., increases in overall survival rates), those randomized to the lower rate would receive full payment. Physicians prescribing new drugs would continue to receive the same administrative fee as before. Richard G. Frank and Ezekiel J. Emanuel, “Paying for Cancer Drugs That Prove Their Benefit,”Journal of the American Medical Association 326, no. 16: 1579–80.
Hospitals Acquired by Private Equity Firms More Likely to Add Profitable Service Lines and Drop Others
Researchers found that relative to hospitals that have not been acquired by private equity firms, those that have are more likely to add certain profitable service lines, including interventional cardiac catheterization, hemodialysis, and labor and delivery. They are also more likely to add profitable technologies (e.g., robotic surgery and digital mammography) and freestanding or satellite emergency departments. Private equity acquisition was also associated with an increased probability of providing services that were previously categorized as unprofitable but have become areas of financial opportunity such as mental health services. Hospitals that have been acquired by private equity firms were less likely to add or continue to offer services that have unreliable revenue streams such as adult day care programs. Marcelo Cerullo et al., “Private Equity Acquisition and Responsiveness to Service-Line Profitability at Short-Term Acute Care Hospitals,”Health Affairs 40, no. 11 (November 2021):1697–1705.
Racial Disparities in Access to Primary Care Evident in Medicare Advantage Hospitalization Rates
Researchers found hospital admissions for ambulatory care–sensitive conditions were substantially higher for Black beneficiaries in Medicare Advantage plans compared with Black beneficiaries in traditional Medicare (221.2/10,000 beneficiaries vs. 209.3/10,000). White beneficiaries in both programs had similar rates for ambulatory care–sensitive admissions (163.7 per 10,000 Medicare Advantage beneficiaries vs. 162.2 in traditional Medicare). The researchers found the racial disparity was prevalent across almost all hospital referral regions, suggesting disparities in access to high-quality primary care. Sungchul Park, Paul Fishman, and Norma B. Coe, “Racial Disparities in Avoidable Hospitalizations in Traditional Medicare and Medicare Advantage,” Medical Care 59, no. 11 (November 2021):989–96.
One in Seven Asian-American Deaths Attributable to COVID-19
Researchers found that while Asian Americans make up a small proportion of COVID-19 deaths in the U.S., compared with whites, they experienced significantly higher excess all-cause mortality (3.1 times higher) and case fatality rates (as much as 53% higher) in 2020. The percentage of deaths attributable to COVID-19 was 2.1 times higher among Asian Americans than whites. The authors say lower testing rates, greater disease severity at care presentation, socioeconomic factors, and racial discrimination all contribute to the observed disparities. Brandon W. Yan et al., “Death Toll of COVID-19 on Asian Americans: Disparities Revealed,” Journal of General Internal Medicine 36, no. 11:3545–49.
Average Cost of a COVID-19 Hospitalization in Fee-for-Service Medicare Nearly $22,000
A study of Medicare beneficiaries in the fee-for-service program found that between April and December 2020, 4.2 percent (or 1.2 million people) sought medical care for COVID-19. Of them, nearly one-quarter (23%) had an inpatient stay and 4.2 percent died. The majority were female (57%), white (79.6%), and residents of an urban county (77.2%). The average hospitalization cost was $21,752, with higher costs for patients needing a ventilator ($49,441). Patients age 75 and older were more likely to be hospitalized, but their hospitalizations were associated with lower costs than younger patients. Being male and non-white was associated with a higher probability of being hospitalized and incurring higher medical costs. Yuping Tsai, Tara M. Vogt, and Fangjun Zhou, “Patient Characteristics and Costs Associated With COVID-19–Related Medical Care Among Medicare Fee-for-Service Beneficiaries,”Annals of Internal Medicine 174, no. 8 (Aug. 2021):1101–9.
Complications for Low-Risk Births Higher at Hospitals Serving Black and Hispanic Women
Compared with white or Asian-American women, Black and Hispanic women were more likely to deliver their babies in hospitals that had high complication rates for low-risk births. The study examined discharge data from 40 New York City hospitals and found the unexpected complication rate varied from 25.3 per 1,000 births to 162.8. The researchers found one-third of Black and Hispanic women gave birth in hospitals ranking in the highest-morbidity tertile compared with 10 percent of white and Asian-American women. The results suggest the need for targeted quality improvement campaigns. Kimberly B. Glazer et al., “Hospital Quality of Care and Racial and Ethnic Disparities in Unexpected Newborn Complications,” Pediatrics 148, no. 3 (September 2021):e2020024091.
Models for Improving Perinatal Mental Health Care in the U.S.
In a Health Affairs article, Adrienne Griffen, executive director of the Maternal Mental Health Leadership Alliance in Arlington, Va., and associates identify gaps in the screening and treatment of perinatal mental health conditions, particularly among parents who may lack access to culturally appropriate mental health care. The authors describe recent federal and state policy efforts to ameliorate these gaps, highlight successful models of care, and offer recommendations for integrating perinatal mental health care into postpartum care. Adrienne Griffen et al., “Perinatal Mental Health Care in the United States: An Overview of Policies and Programs,”Health Affairs 40, no. 10 (October 2021):1543–50.
The Hazards of Using Serious Mental Illness as a Policy Construct
In this Health Affairs article, Jeffrey A. Buck, a former senior advisor for behavioral health with the Centers for Medicare and Medicaid Services, questions the practice of focusing mental health policies around patients with serious mental illnesses (SMI). He says the problem with doing so is that there is little consensus around the definition of the term and insufficient data on the diagnostic makeup of the population. Before implementing policies for such an ill-defined group, he suggests policymakers ask themselves several questions: Does the proposed policy address an issue that is unique to the SMI population, or is it shared by people with less severe disorders? Would it increase problems of stigma for those it is intended to help? Would a diagnostic-specific approach be more effective? Would the policy create undesirable incentives for providers or other negative consequences that would be lessened if it were not focused on SMI? Jeffrey A. Buck, “Problems With ‘Serious Mental Illness’ as a Policy Construct,”Health Affairs 40, no. 12 (December 2021):1953–60.
Despite National Declines in Kidney Failure Incidence, Disparities Widened Between Low- and High-Poverty Counties
A study examining trends in the incidence of kidney failure at the county level found disparities between high- and low-poverty counties widened between 2000 and 2017, a period when the national incidence of kidney failure was declining. The magnitude of the disparity increased from 42.8 more incident cases per million in high-poverty counties during the years 2000–05 to 100.1 more in the years 2012–17. Achieving the U.S. Department of Health and Human Services’ objective of reducing kidney failure cases by 25 percent by 2030 will require deliberate efforts to prevent it in counties with higher poverty rates, the authors say. Kevin H. Nguyen et al., “Despite National Declines in Kidney Failure Incidence, Disparities Widened Between Low- and High-Poverty U.S. Counties,” Health Affairs 40, no. 12 (December 2021):1900–8.
Three-Year Pilot of the Oncology Care Model Produces No Net Savings
The use of the Oncology Care Model, an alternative payment model for providers that seeks to improve care quality and coordination for Medicare beneficiaries undergoing chemotherapy, was associated with modest payment reductions during six-month episodes of care. But the savings — $297 per beneficiary — were not sufficient to offset care coordination and pay-for-performance bonuses to practices. Researchers also found no statistically significant differences in measures of utilization, quality, and patient experiences for patients receiving care at practices participating in the model when compared with patients of nonparticipating practices. The study looked at utilization and payments for hospitalizations, emergency department visits, office visits, chemotherapy, supportive care, and imaging. Nancy L. Keating et al., “Association of Participation in the Oncology Care Model With Medicare Payments, Utilization, Care Delivery, and Quality Outcomes,”Journal of the American Medical Association 326, no. 18 (November 2021):1829–39.
Strategies for Improving Chronic Disease Management in the U.S.
In a commentary in the New England Journal of Medicine, Marshall H. Chin, M.D., M.P.H., a professor of health care ethics at the University of Chicago and a member of Transforming Care’s editorial advisory board, outlines several strategies for improving chronic disease management in the U.S. They include leveraging payment to promote a team-based approach to care, one that integrates in-person and virtual care and allows for remote monitoring and coaching. Chin also calls on delivery systems, payers, and policymakers to prioritize health equity by investing in disease management approaches that benefit marginalized populations. Marshall H. Chin, “Uncomfortable Truths — What Covid-19 Has Revealed about Chronic-Disease Care in America,”New England Journal of Medicine 385, no. 18:1633–6.
Editorial Advisory Board
Special thanks to Editorial Advisory Board member Marshall Chin for his help with this issue.
Jean Accius, Ph.D., senior vice president, AARP
Anne-Marie J. Audet, M.D., M.Sc., senior medical officer, The Quality Institute, United Hospital Fund
Eric Coleman, M.D., M.P.H., director, Care Transitions Program
Marshall Chin, M.D., M.P.H., professor of healthcare ethics, University of Chicago
Timothy Ferris, M.D., M.P.H., CEO of Massachusetts General Physician Organization and professor of medicine at Harvard Medical School
Don Goldmann, M.D., chief medical and scientific officer, Institute for Healthcare Improvement
Laura Gottlieb, M.D., M.P.H., assistant professor of family and community medicine, University of California, San Francisco, School of Medicine
Martha Hostetter and Sarah Klein, The Perils and Payoffs of Alternative Payment Models for Community Health Centers (Commonwealth Fund, Jan. 19, 2022). https://doi.org/10.26099/2ncb-6738