Medicaid, the public health insurance program covering more than 72 million people with low income, is jointly funded by states and the federal government. Medicaid spending totaled around $890 billion in the 2023 federal fiscal year, with the federal government paying 69 percent and states paying 31 percent.
States administer their own Medicaid programs within broad parameters set by the federal government. In the same way that each state’s program has significant variation in who is covered, what is covered, and how much is paid for care, there is variation in how the program is funded at the state level. The federal government’s contribution also differs from state to state.
How is the federal share of Medicaid funding determined?
The federal share of Medicaid funding — typically called the federal match or the federal medical assistance percentage (FMAP) — is expressed as the percentage of state spending matched by the federal government. The base federal match, FMAP for health services for the traditional Medicaid population, varies by state, ranging from 50 percent to 77 percent in the 2023 federal fiscal year. The exact rate is determined by a formula set in law that uses state per capita income relative to national per capita income; states with lower per capita income receive a higher share of federal funding. By law, this base FMAP cannot exceed 83 percent or fall below 50 percent.
Specific services and eligibility groups have their own FMAP rates set in statute. Administrative costs, including day-to-day operations and oversight of managed care contracts are matched at 50 percent, while technology updates to eligibility and enrollment systems are 75 percent or 90 percent. Federal funding for Medicaid has grown over time as new groups and types of services were authorized by Congress, for example optional and then mandatory coverage of pregnant women up to the federal poverty level in the 1980s. Most recently, in states that expanded Medicaid eligibility as authorized by the Affordable Care Act, the newly covered population has an enhanced FMAP of 90 percent.
How do states finance their Medicaid programs?
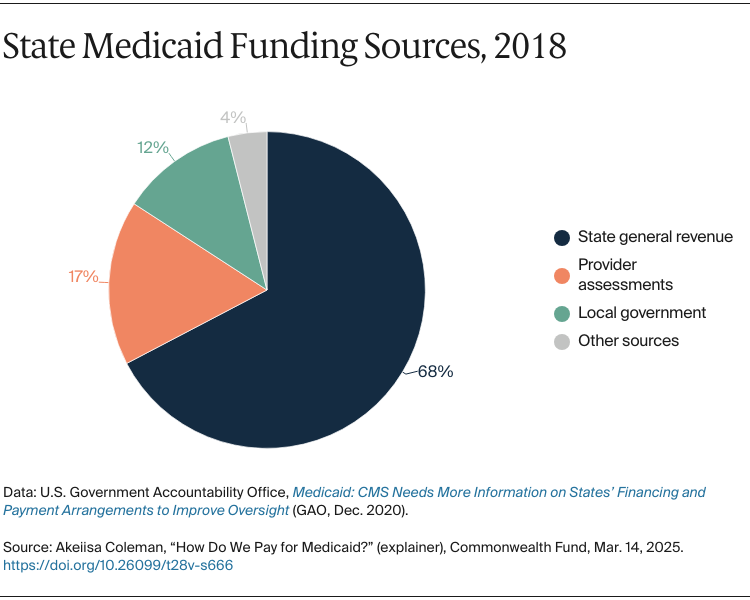
States primarily pay their share of the Medicaid program through general revenue, including taxes and other monies collected by the state. Medicaid is typically the second-largest state expense behind K–12 education, and the largest source of federal funding. Counties and local governments may also contribute, but states must pay at least 40 percent of the nonfederal share of Medicaid expenditures. Local government funding can involve intergovernmental transfers or direct spending on Medicaid services or program administration, known as certified public expenditures.
States have multiple methods for financing their share of Medicaid funding. Provider assessments, commonly in the form of taxes on hospitals, nursing homes, or managed care organizations are a major source of funding. Every state except Alaska has at least one provider assessment, and this funding mechanism has been allowed since the inception of the Medicaid program in 1965. Other state funding sources may include cigarette taxes; settlement funds, such as the tobacco master settlement agreement; pharmaceutical rebates; insurance premium taxes, including funds formerly used to support state high-risk pools; and sales taxes, such as in Utah, which increased sales tax 0.15 percentage points to fund its Medicaid expansion.
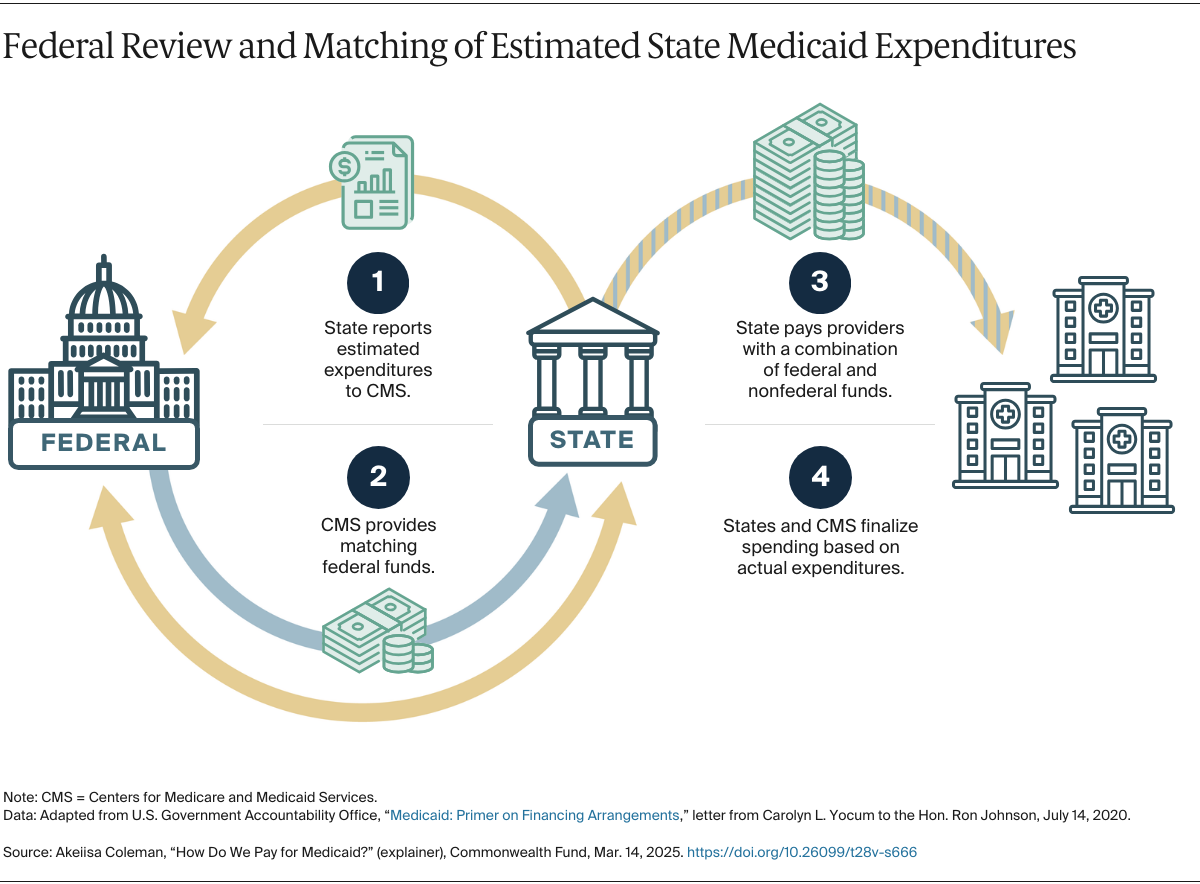
How does federal funding flow to states?
State Medicaid agencies report how much they have spent on covered services to the Centers for Medicare and Medicaid (CMS), which then matches these funds at the regular or enhanced FMAP based on the enrollment group of the beneficiary or type of service. Expenditures are confirmed by claims data after payments to providers are made, and they’re often adjusted to correct coding or billing errors, among other reasons. Following a reconciliation process, states may return overpayments, receive funds to offset underpayments, or be asked to provide additional information to verify provider or enrollee eligibility.
The federal match for administration works similarly. States report to CMS how much they have spent over a specified period, and CMS then matches this based on the FMAP for the types of administrative services claimed.