
More than 68 million people rely on Medicare for their health coverage, including 55.5 million adults enrolled in prescription drug coverage under Medicare Part D. In 2023, Part D drug spending totaled nearly $145 billion.
The Inflation Reduction Act, signed into law by President Biden in 2022, for the first time authorized the federal government to negotiate the prices that Medicare pays for selected prescription medications. Previously, Medicare played no role in determining drug prices, relying instead on commercial prices negotiated by pharmacy benefit managers and health insurers.
How does the Medicare Drug Price Negotiation Program work?
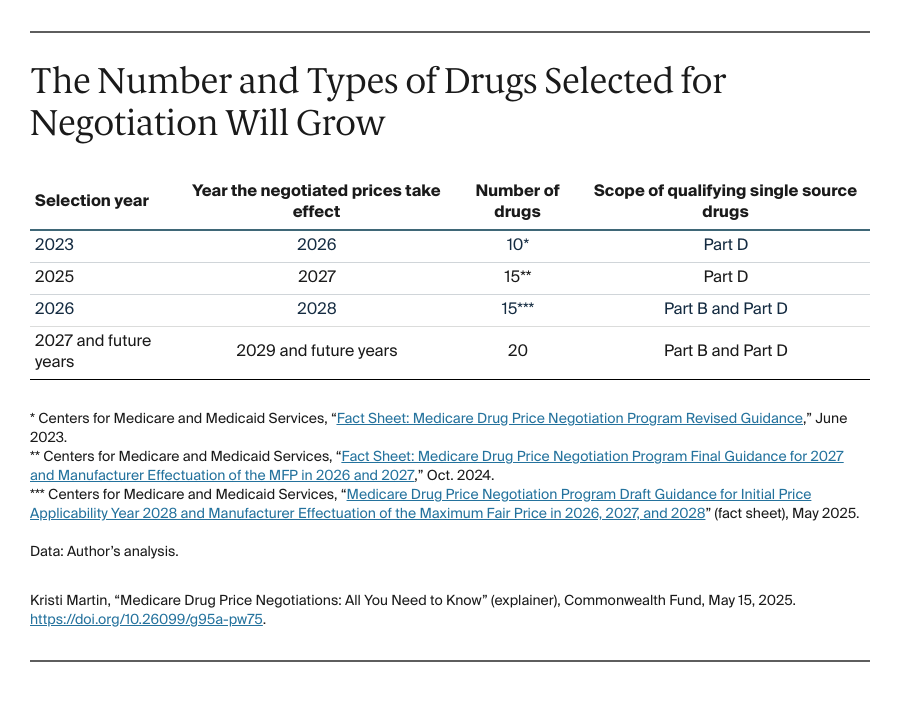
Under the Medicare Drug Price Negotiation Program, the Secretary of the U.S. Department of Health and Human Services works directly with pharmaceutical manufacturers to negotiate the prices Medicare will pay for medications — specifically, those that account for a large portion of the program’s drug spending. The law provides specific instructions for Medicare, including how many drugs should be selected for price negotiations each year, what information should be considered in negotiations, and the timeline for negotiations.
In 2023, the Centers for Medicare and Medicaid Services (CMS) initiated the first negotiations for 10 drugs covered under Medicare Part D. These include such commonly prescribed medications as Januvia (for treating diabetes), Eliquis (for blood clots), and Entresto (for heart failure).
In 2024, CMS reached agreement on “maximum fair prices” for these drugs with the companies that make them. The new prices are slated to take effect in January 2026.
Why didn’t Medicare always negotiate drug prices?
Before the IRA took effect, the Medicare program was prohibited from negotiating prices directly with drug companies. When the Part D program was established by Congress in 2003, it included a provision called the “noninterference clause,” which prohibits CMS from interfering with negotiations between Part D plan sponsors and manufacturers or pharmacies.
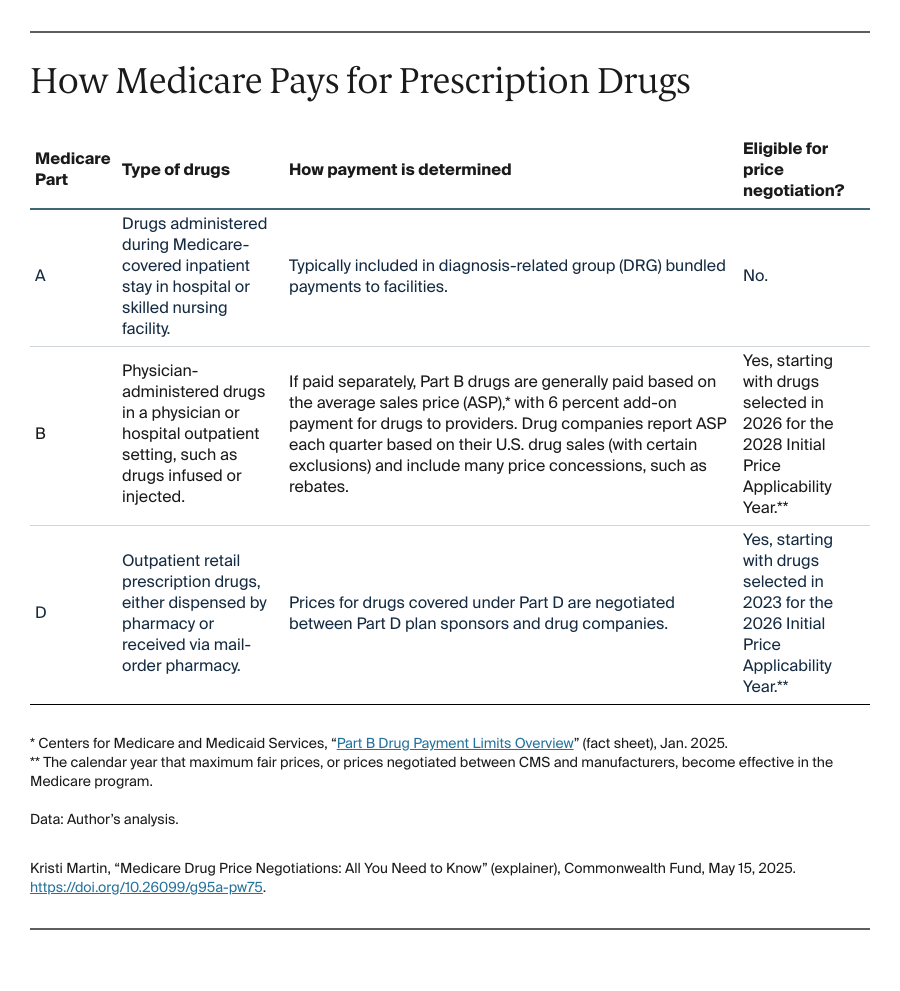
Payment rates and terms for drugs covered under Medicare Parts A, B, and D are set in statute (see table). For drugs not selected for negotiation, Medicare continues to pay for them under the existing payment systems.
How are drugs selected for negotiation?
By law, CMS negotiates prices for drugs that Medicare spends the most on and that have no generic or biosimilar competition. Each year, CMS begins by determining which drugs are eligible for negotiation, known as Qualifying Single Source Drugs (QSSDs).
To be a QSSD, a small-molecule drug must have received its first approval from the Food and Drug Administration (FDA) at least seven years prior to being selected for negotiation and must have no generic competition. Small-molecule drugs are made of chemical compounds; they include brand-names such as Eliquis, Entresto, Farxiga, Jardiance, and Ozempic.
To be a QSSD, a biologic therapy must have been approved by FDA at least 11 years prior to being selected and must have no competition from biosimilar drugs. Generally speaking, biologics are either 1) large, complex molecules derived from sugars, proteins, or nucleic acids, or complex combinations of these substances, or 2) living entities such as cells. Examples of brand-name biologics include Enbrel, Novolog/Fiasp, and Stelara.
Once the list of QSSDs is determined, CMS applies certain exclusions to remove “low spend” drugs (those accounting for less than $200 million of Medicare spending); orphan drugs, defined as drugs with one designation and approval for a rare disease; and plasma-derived biologic products derived from human whole blood or plasma.
Also left off the negotiation-eligible list are drugs previously selected for negotiation, those deemed highly likely to face biosimilar competition, and those meeting the criteria for a small biotech drug.
Of the drugs that remain, the ones with the highest Medicare gross spending are selected for negotiation. (See this CMS fact sheet for more on the selection process.)
How does the negotiation process work?
The process begins with drug companies signing agreements with CMS to kick off negotiations and submitting information to the agency in February. By statute, CMS must consider the following information as part of the negotiations:
- Drug-specific information submitted by drug companies: research and development (R&D) costs, costs of production and distribution, prior federal financial support for R&D, information on pending and approved patent applications, and U.S. sales and market data.
- Information on the selected drug’s “clinical benefit” submitted by the public (such as consumer and patient organizations, researchers, providers, other drug companies): the extent to which the selected drug represents a therapeutic advance compared to existing alternatives, FDA-approved prescribing information and therapeutic alternatives, comparative effectiveness and therapeutic alternatives for specific populations (such as people with disabilities, older adults, people with terminal illness, and children), and whether the selected drug addresses an unmet medical need.
Once CMS receives this information by March each year, officials issue an initial price offer to the drug company no later than June 1 and begin a back-and-forth negotiation process which concludes by November 1. At any time during this process, CMS and the drug company may come to an agreement on a negotiated price, also known as the maximum fair price. If no agreement is reached, CMS provides the drug company with a final offer no later than October 15. The company must respond to that offer before November 1, the end of the negotiation period.
What are the key controversies surrounding drug price negotiation?
Too many drugs are excluded. Under CMS’s current selection criteria for price negotiation, two-thirds of drugs covered under Medicare Parts B and D are not eligible, one study estimates. Instead of narrowing the universe of drugs that are eligible for negotiation, some say that Medicare should be negotiating prices for more drugs in order to further lower drug spending and patient costs.
Pharmaceutical innovation may suffer. Since passage of the Inflation Reduction Act, the pharmaceutical industry has kept up a steady drumbeat that the price negotiation program would result in loss of innovation. In 2021, the Congressional Budget Office estimated that it could lead to 9 percent fewer new drugs entering the market over 30 years.
However, there does not appear to be evidence of any measurable impact on R&D since that time. It’s important to understand that R&D for prescription drugs is a complex ecosystem that includes investment by both public and private entities. Until recently, the primary engines for public investment in pharmaceutical R&D — the National Institutes of Health, Advanced Research Projects Agency for Health, and National Science Foundation — saw increases in their budgets to support innovation. Meanwhile, R&D spending by private industry has actually increased since 2022.
There also is little evidence of a reduction or disruption in merger-and-acquisition activity, another measure of innovation in the pharmaceutical industry. Early-stage product development, including for small-molecule drugs, continues at a steady pace. In fact, many of the companies making drugs that have been selected for negotiation have noted in their shareholder reports that negotiation won’t materially impact revenues.
Industry incentives will cause a shift away from small-molecule drug development. A related but more nuanced argument concerns the structure of the law and when drugs are eligible for negotiation. As noted above, a small-molecule drug is eligible for selection seven years after its first FDA approval, and a biologic product is eligible 11 years after its first FDA approval. Critics refer to the difference in the criteria as the “pill penalty”: they say the discrepancy creates a disincentive to develop small-molecule drugs, since there is a shorter timeframe for recouping R&D costs.
But the Medicare Drug Price Negotiation Program already takes into consideration differences in R&D costs, as well as the time drug manufacturers need to recoup these costs. Under FDA rules, brand-name small-molecule drugs have five years of market exclusivity before a generic version can be approved, while biologics have 12 years of market exclusivity before biosimilars can be approved.
These windows of market exclusivity are prefaced on the well-documented differences in the costs and complexity involved in commercializing these products. For example, one recent study showed that the average cost for developing a small-molecule drug was $2.1 billion, compared to $3 billion for a biologic product.
What does the future hold for the Medicare Drug Price Negotiation Program?
Litigation continues. Ongoing legal challenges related to Medicare drug price negotiation fall into two categories of claims: statutory and regulatory authority. To date, CMS has withstood these challenges, but the pharmaceutical industry is expected to continue filing litigation to narrow the government’s authority to implement the program.
Lawmakers advance proposals to limit or expand the program. Bills have been introduced to limit as well as expand the price negotiation program. In terms of limiting the program, amendments to the law have been proposed to: 1) increase the time post–FDA approval until which a small-molecule drug would be eligible for negotiation, from seven to 11 years; 2) expand the scope of drugs eligible for the orphan drug exclusion; and 3) extend and expand the exception for products developed by small biotech firms to include additional drugs.
Other lawmakers have proposed expanding the program. They seek to: 1) extend the price negotiation to the commercial market; 2) increase the number of drugs that CMS can select for negotiation each year; 3) shorten the number of years for drugs to be eligible for negotiation; and 4) lower the ceiling for negotiating maximum fair prices.
The program enters rulemaking in 2026. CMS recently issued its last round of guidance as stipulated by the Inflation Reduction Act. In the first three years of the program, CMS was required to issue guidance and voluntarily solicited public comment. Starting in 2026, CMS will begin formal rulemaking for the program, which will inform the fourth cycle of drug selection and price negotiations.


