


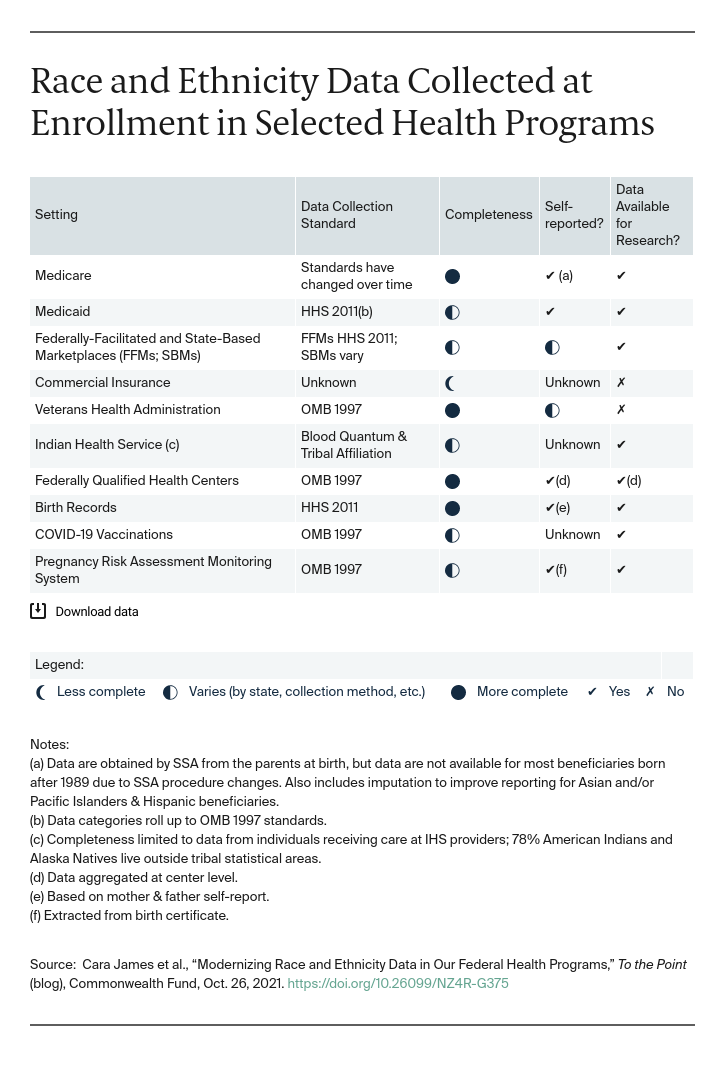
The COVID-19 pandemic exposed our long-standing inability to collect, share, and act on meaningful race and ethnicity data in health care. According to the Centers for Disease Control and Prevention, race and ethnicity data are not available for nearly 40 percent of people testing positive for COVID or receiving a vaccine. This situation is not unique to COVID-19. There are major concerns about the quality of Medicaid data in 22 states. In Medicare, data standards have varied over time. Data are incomplete in other federal and state programs.
These gaps limit our knowledge of health disparities and our ability to eliminate them. “We don’t know” is no longer an acceptable answer.
To move forward, Grantmakers In Health and the National Committee for Quality Assurance reviewed the literature and interviewed key informants from health care organizations, state and local health officials, actuaries, and consumers, to determine how race and ethnicity data are collected and used across federal and state health programs and to develop recommendations for improving the quantity and quality of the data. A recently published report identifies opportunities for immediate federal action; a second forthcoming report will provide intermediate and long-term recommendations for states and federal policymakers.
The report explores the reasons health programs do not have complete and accurate race and ethnicity data. Two of the biggest barriers are:
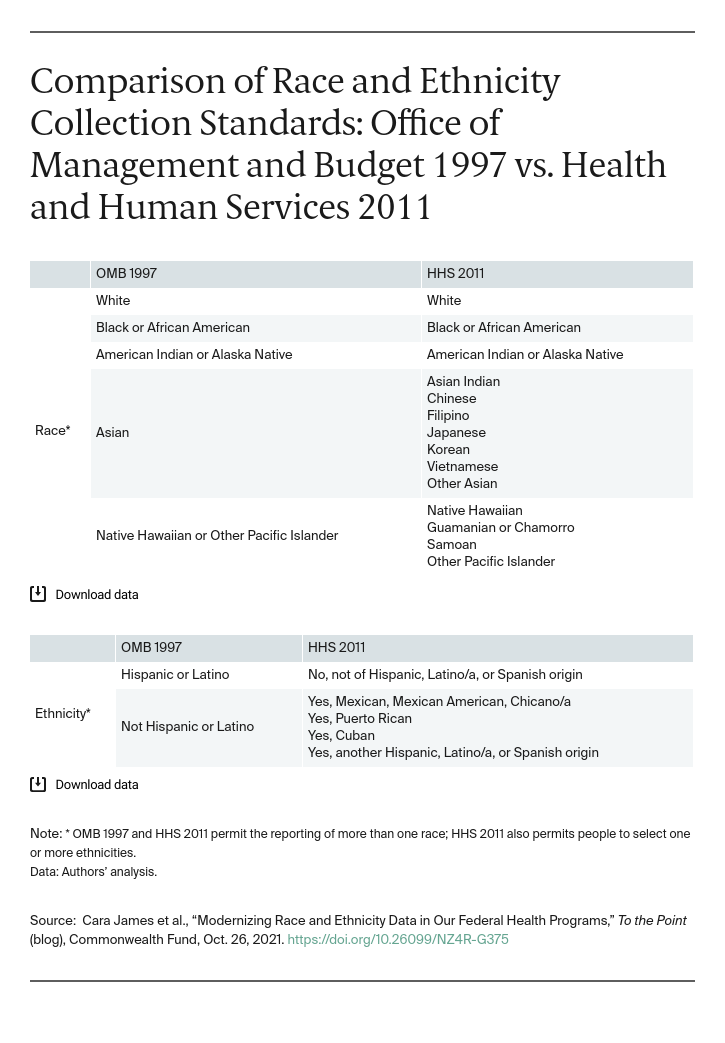
- Lack of a clear and sufficient federal standard. Within the U.S. Department of Health and Human Services (HHS), two standards are used. The first, finalized by the Office of Management and Budget (OMB) in 1997, includes five race categories and Hispanic as the only ethnicity. The second, finalized by HHS in 2011, includes these, plus additional categories within Asian, Native Hawaiian, and Other Pacific Islander and Hispanic. While the HHS group offers more categories, it is less commonly used; neither standard sufficiently represents the diversity of the U.S. population.
- Misconceptions and fear. Stakeholders noted common beliefs of legal restrictions on collecting race and ethnicity data. However, there are no federal limitations, and only a few states limit data collection in certain circumstances. Others noted that some individuals are unwilling to self-identify and providers and staff are reluctant to ask.
Swift Action by the Federal Government Can Fill Gaps
To overcome these barriers to high-quality, complete data on race and ethnicity, the report details 11 recommendations, including:
Updates to data standards and requirements for equity reporting. Building on the Biden administration’s executive order on advancing racial equity, the federal government can provide leadership and a vision for standardizing collection and analyzing and acting on data to reduce health inequities. Specifically, federal action is needed to: update OMB data-collection standards, standardize collection and reporting across federal data systems and programs for both patient and provider data, and require reporting on racial and ethnic health disparities for all federal program reports and audits, where practical.
Resources to support data collection and sharing. The federal government has many avenues for working with state and local agencies, as well as health care organizations, to support improvement efforts. The federal government should take the lead in raising awareness and developing educational resources to support data collection and sharing. These resources can allay fears and improve response rates by providing clear information on why data are being collected and how they will be used. In addition, the government can highlight the examples of leading organizations that have obtained nearly complete data. The federal government also could encourage states to use existing resources and provide additional resources as needed to help states improve their data infrastructure and to support data sharing.
Involving communities. Communities that have been historically marginalized and most impacted by health disparities need to be prioritized in the development of data standards and materials. Given past and ongoing discrimination and persistent inequities in treatment, experience, and outcomes, we must expect questions about how health care organizations will use the data. The federal government should support efforts to engage communities to collaborate on addressing these questions to ensure approaches that reflect the community.
Regulation to address real or perceived concerns about data sharing. Federal action is needed to review laws that address data sharing across federal programs while maintaining privacy protections. For example, Congress should review and consider amending the Health Information Portability and Accountability Act (HIPAA), the Family Educational Rights and Privacy Act, and the Affordable Care Act to encourage data sharing.
The pandemic revealed how the lack of race and ethnicity data thwarts efforts to serve our communities equitably. We cannot improve what we cannot see or fail to measure. Federal leadership and collective action by states, health care organizations, and communities are necessary to achieve health equity. The path to health equity starts with collecting complete, accurate, and reliable race and ethnicity data.


