
Medicaid is the largest public health insurance provider in the United States. As such, Medicaid policy has significant implications for the health of people with low incomes. One issue affecting access to care is Medicaid’s notably low reimbursement rates: health providers and institutions often spend more money caring for Medicaid beneficiaries than they receive in reimbursement. For example, in 2020 hospitals received only 88 cents for every dollar spent caring for Medicaid patients. This amounted to a $24.8 billion underpayment. Low reimbursement rates limit access to quality care and contribute to poor health outcomes for Medicaid beneficiaries, who are disproportionately people of color. Research suggests that increasing Medicaid primary care rates by $45 per service would reduce access-to-care inequities by at least 70 percent.
Using the Racial Equity and Policy (REAP) framework, a tool for assessing how structural racism is embedded in policy processes, this blog post outlines specific dimensions of the policy environment and broader key considerations around Medicaid reimbursement and racial equity.
Medicaid Reimbursement and the Policy Environment
First, we highlight key facets of the policy environment:
- Ideas. Identifying ideas around reimbursement rates can facilitate critical assessment of policy choices. For example, ideas about efficiency can operate in opposition to ideas about fairness and justice. Surfacing and confronting those tensions is crucial.
- Institutions. The Medicaid statute requires states to pay rates that ensure equal access for program beneficiaries. Yet, courts have rebuffed beneficiary and provider attempts to enforce this mandate. The courts point out that the Centers for Medicare and Medicaid Services (CMS), which has federal oversight of Medicaid, does not consider payment rates a metric of access to care. Seemingly racially neutral decisions by courts and federal agencies create conditions for an inequitable payment structure.
- Actors. The secretary of the Department of Health and Human Services (HHS) and the director of CMS are key actors who shape Medicaid reimbursement rates at the federal level. Actors at the state level can include coalitions of stakeholders and local networks of providers that have opinions and preferences about reimbursement rates. Federal and local actors can interact and even counter each other. In 2021, the National Association of Chain Drug Stores, Washington State Pharmacy Association, and National Community Pharmacists Association filed a lawsuit against the HHS secretary and the acting CMS administrator for approving Washington’s Medicaid State Plan Amendment. They claimed the reimbursement rates were so far below the cost of dispensing drugs to patients that they violated a 2016 CMS rule and put patients’ access to care at risk.
Considering Voice, Decentralization, and Disproportionality
We then emphasize three key considerations: voice, decentralization, and disproportionality.
Voice sensitizes us to who is at the decision-making table, who is heard, and ultimately who has the power to influence policy outcomes. Medicaid reimbursement rates are a distant issue that may be more salient to actuaries than to the people most affected by decisions. Yet, it is critical to pay attention to the voices with the most at stake — Medicaid beneficiaries. Examples from our interviews show that even when beneficiaries don’t directly discuss reimbursement, they provide valuable perspectives about access and reimbursement rates:
Daphne (Black woman, New York): I just know a lot of doctors on Medicaid, they know you’re on Medicaid and it’s like, well, you guys are lucky we’re even taking this. They’re just not as gentle with you. They’re really short and they come in for five minutes to see you and have you waiting for an hour or even more. So, I feel like the service is not as good. If I was probably wealthier, it would probably be a lot different.
Lucy (Black woman, Georgia): There’s a difference as far as people with private insurance. I think they get treated more; I think they get treated better. . . . It’s more time with the visit. . . . Whereas with Medicaid it’s like okay, you are on Medicaid, it is what it is, this is the only medicine I can give you. Let me hurry up and see you and get out.
Decentralization concerns the level of government through which a policy is designed or implemented. As in our Washington State example, decentralization of the Medicaid system added an additional layer of complexity for advocates concerned with the access-to-care issues of below-cost reimbursement rates. The Washington network of actors was forced to engage federal institutions to change state policy. Decentralization can be — but is not always — detrimental to racial justice efforts.
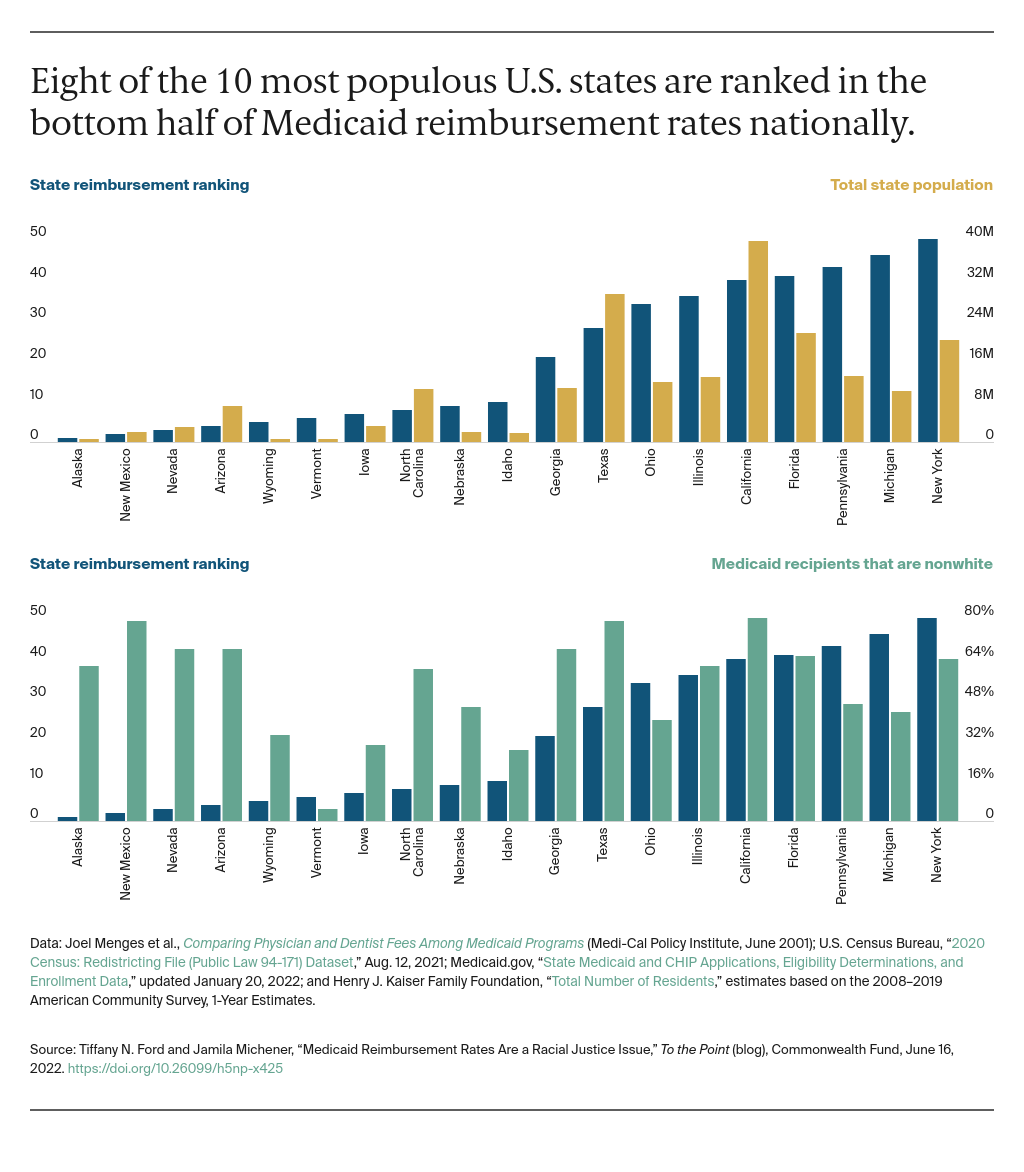
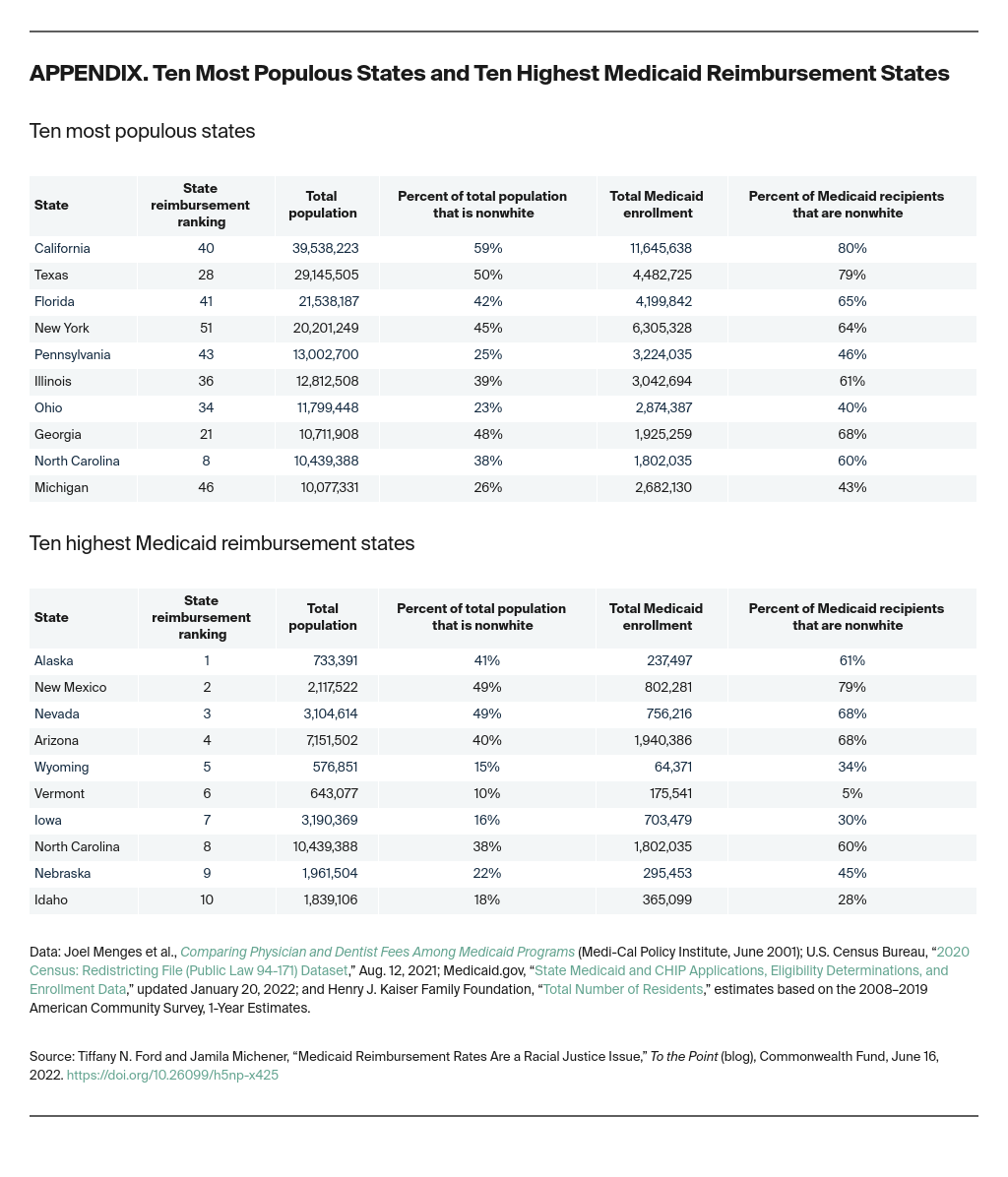
Disproportionality, or “the way policies differentially allocate benefits and burdens to racial groups,” is apparent in current Medicaid reimbursement rates. Eight of the 10 most populous U.S. states are ranked in the bottom half of reimbursement rates nationally. Many of these states have considerably higher nonwhite populations enrolled in Medicaid and relatively lower reimbursement rates. In contrast, many of the states with the highest reimbursement rates have proportionally fewer residents of color (Vermont, Wyoming, Iowa, Idaho, Nebraska).