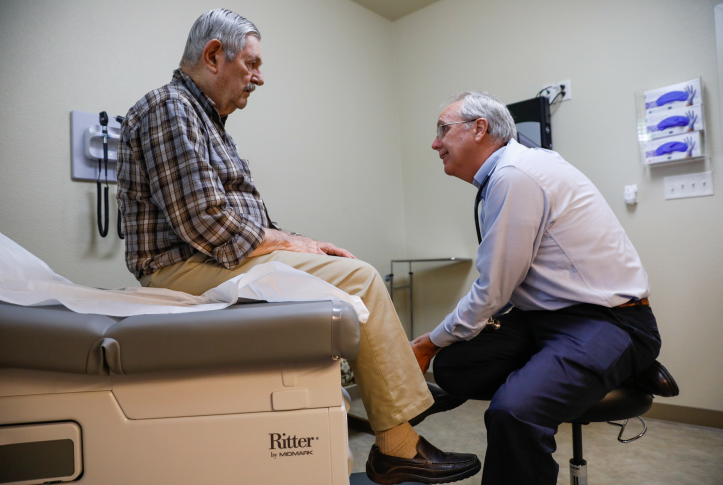



Primary care is associated with improved life expectancy and reduced health care disparities. It is the frontline of our health care system, and is critical for tackling the growing behavioral health crisis and addressing social needs of patients, particularly in the wake of the COVID-19 pandemic.
Despite its value, several indicators suggest that the sustainability and future of primary care is at risk. The percent of people reporting a usual source of care is declining and, compared to other high-income countries, U.S. patients report worse access to care and poor care coordination. Conditions are likely to deteriorate further as the supply of primary care physicians (PCPs) shrinks, particularly in rural areas, as a result of more physicians reaching retirement age, fewer physicians choosing to go into primary care, and growing burnout. As one of the country’s largest payers, Medicare can have a profound impact in addressing these issues and revitalizing primary care in the United States.
The National Academies of Sciences, Engineering, and Medicine (NASEM) 2021 report on primary care highlighted two factors contributing to the deterioriating state of primary care: decades of underinvestment and issues related to how we pay for care. The portion of health care dollars going to primary care is small and decreasing over time across payers; the U.S. spends an estimated 4 percent to 6 percent of total health care dollars on primary care. In Medicare, primary care represents roughly 3 percent of spending despite the greater needs of older and disabled adults for care coordination and management of chronic conditions.
Part of what accounts for the underinvestment in primary care is low reimbursement for primary care services, especially when compared to medical procedures and specialty care services. The Medicare process for updating payment rates is flawed and outdated, relying heavily on recommendations from a specialist-dominated committee that consistently undervalues the time and resources primary care clinicians need to evaluate and manage their patients. Primary care’s financial unsustainability is further constrained by its reliance on fee-for-service payment, a retrospective, piecemeal approach that leaves clinicians maximizing volume and rushing visits. It also discourages innovation, team-based care, and care coordination. These features are associated with better quality and greater patient satisfaction.
Changing how and how much we pay for primary care is a critical next step to reverse these trends and strengthen primary care, and a topic recently discussed by the Medicare Payment Advisory Commission (MedPAC). Medicare reforming the way it pays for primary care would have a profound effect on payment rates for all physician services, as many payers base their fees on Medicare.
Building on ideas generated by NASEM and MedPAC, the following are options Congress could consider to strengthen primary care through Medicare payment reform:
- Increase payment for primary care services. To address the undervaluation of primary care services, Congress could create two fee schedules: one for the evaluation and management of patients — everyday diagnosis, treatment, counseling, and patient or family support (known as E&M services) — and one for everything else. A dedicated E&M fee schedule would protect against payment for primary care–related services being decreased to accommodate fee increases for other specialty services, which is required to keep the overall fee schedule budget-neutral.
- Develop a partial capitated per-member per-month payment model. In addition to fixing the fee schedule, per-member per-month payments would provide clinicians a fixed amount per patient paid in advance, allowing clinicians to innovate, budget, and more easily integrate others kinds of care, like behavioral health or telehealth, into primary care. To ensure the payments are sufficient and address current undercompensation, they should represent a 30 percent to 50 percent increase in current revenues.
For this to work, Medicare will need data from patients about who they consider to be their primary care provider. As an incentive for patients to designate a primary care clinician, Congress could waive any cost sharing for office visits when patients indicate their primary care clinician on an annual basis. - Modernize the Medicare Physician Fee Schedule. Create a new expert panel that simplifies the Medicare Physician Fee Schedule, collapsing the current 8,000 service codes into “clusters” of related services (e.g., eliminate 21 different types of colonoscopies). Congress also can task the experts with identifying ways the Centers for Medicare and Medicaid Services (CMS) can determine rates using objective, empirical data rather than the current process, which relies on flawed estimates of clinician time and work.
- Increase overall spend on primary care. Congress could direct CMS to require its payers and plans to measure and annually report the portion of total spending going to primary care, with the goal of increasing that proportion over time.
Investing in primary care has the potential to yield high-quality, sustainable, and equitable primary care. Over the long term, changing how and how much we pay for primary care can be budget-neutral or generate savings. For instance, recent evidence shows that more primary care clinicians and E&M visits in an accountable care organization are associated with cost savings. Other analyses have shown a correlation between an increased supply of primary care physicians and lower total costs of health services, including in Medicare.
Primary care payment reform in Medicare can help restore balance to a health care financing system that is badly misaligned. As a long-term investment, restructuring primary care can address the workforce shortage, improve the health of the population, and create greater equity.


