Congress has until the end of the year to extend several expiring health care provisions, including COVID-19 telehealth flexibilities and funding for community health centers. But the parties will have to agree to policies that could help pay for these “must-do” items, perhaps by advancing bipartisan health policy priorities to help offset the extensions. The potential lame-duck health package could move with government funding due December 20. In this blog post, we highlight health policies that are primed for consideration this year.
“Must-Do” Items
Medicare
Several Medicare programs, waiver flexibilities, and temporary reimbursement increases expire December 31. Among these are a boost to Medicare physician payments that helped offset a more than 3 percent cut for 2024 and upward payment adjustments for low-volume and Medicare-dependent hospitals. Temporary telehealth flexibilities and the Acute Hospital Care at Home waiver, which were put in place during the COVID-19 public health emergency and have been extended multiple times, also expire at the end of the year. Congress is expected to again at least partially offset the anticipated 2.8 percent payment cut for Medicare providers in 2025, as it has for the last four years, and maintain the policies noted above for at least two years.
Health Care Safety Net
Congress is also expected to reauthorize funding for health care safety-net programs, such as community health centers, which expire at the end of the year. Similarly, Congress is likely to postpone Medicaid payment reductions to safety-net hospitals set to take effect in January.
Other Policy Priorities
Health Care and Drug Costs
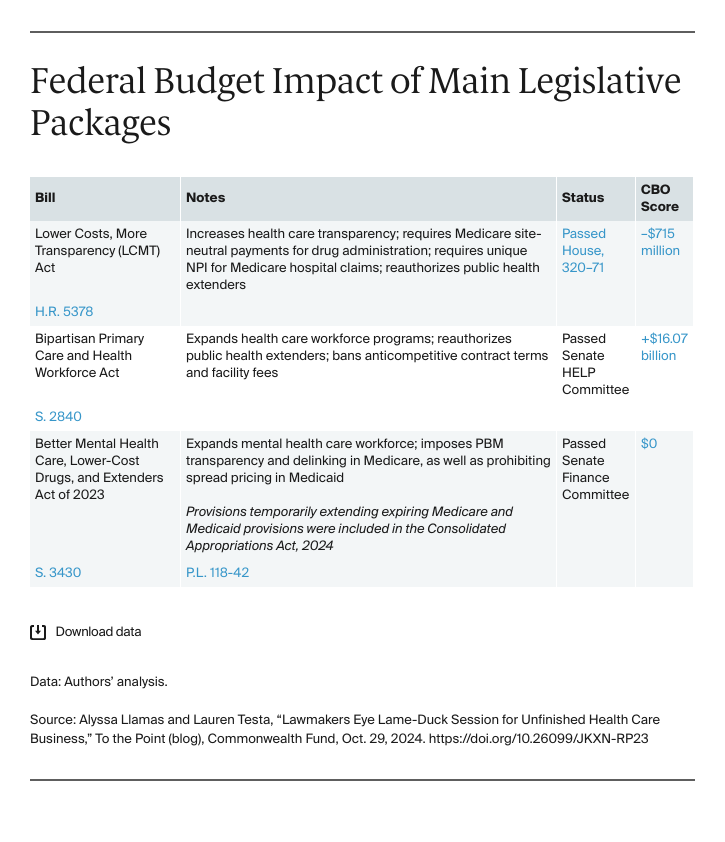
Despite differing views on the role of the federal government in health care, Republicans and Democrats agree on a narrow set of provisions to lower health care and drug costs. The House-passed Lower Costs, More Transparency (LCMT) Act (H.R. 5378) is a likely starting point for negotiations. The bipartisan bill includes measures to strengthen price transparency requirements for hospitals, insurers, and pharmacy benefit managers; increase access to lower-cost generic medications; and require the same Medicare payment for physician-administered drugs regardless of whether the service is performed in an off-campus hospital outpatient department (HOPD) or a doctor’s office. Additionally, it includes a requirement for each off-campus HOPD to file Medicare hospital claims with a unique national provider identifier (NPI) rather than the NPI for the main hospital campus. This would disclose the specific location of care, which could facilitate future reforms to lower payments for medical procedures delivered in lower-cost settings to reduce overall health care spending. The Senate has not passed a comparable health package but has several similar bills that closely mirror proposals in the LCMT Act.
The enhanced premium tax credits (PTCs) expire at the end of 2025; Democrats are pushing for a one-year extension. They will advocate for making the policy permanent before expiration, but a short-term fix is necessary to provide health insurers with certainty and avoid severe premium increases for plan year 2026. Health insurers need to know by spring 2025 whether to account for the presence or absence of enhanced PTCs in setting premium rates for 2026. Such unpredictability makes it difficult for health insurers to anticipate the level of risk, and health care costs, of enrollees. Republicans strongly oppose a permanent extension, citing budgetary concerns.
Public Health
Partisan disagreements have stymied the reauthorization of key programs on substance use disorder prevention and treatment and pandemic preparedness. The SUPPORT Act and the Pandemic and All-Hazards Preparedness Act (PAHPA) expired on September 30, 2023. Several of these programs continue to get funded through annual appropriations, but they have not been updated to reflect lessons learned over the past five years.