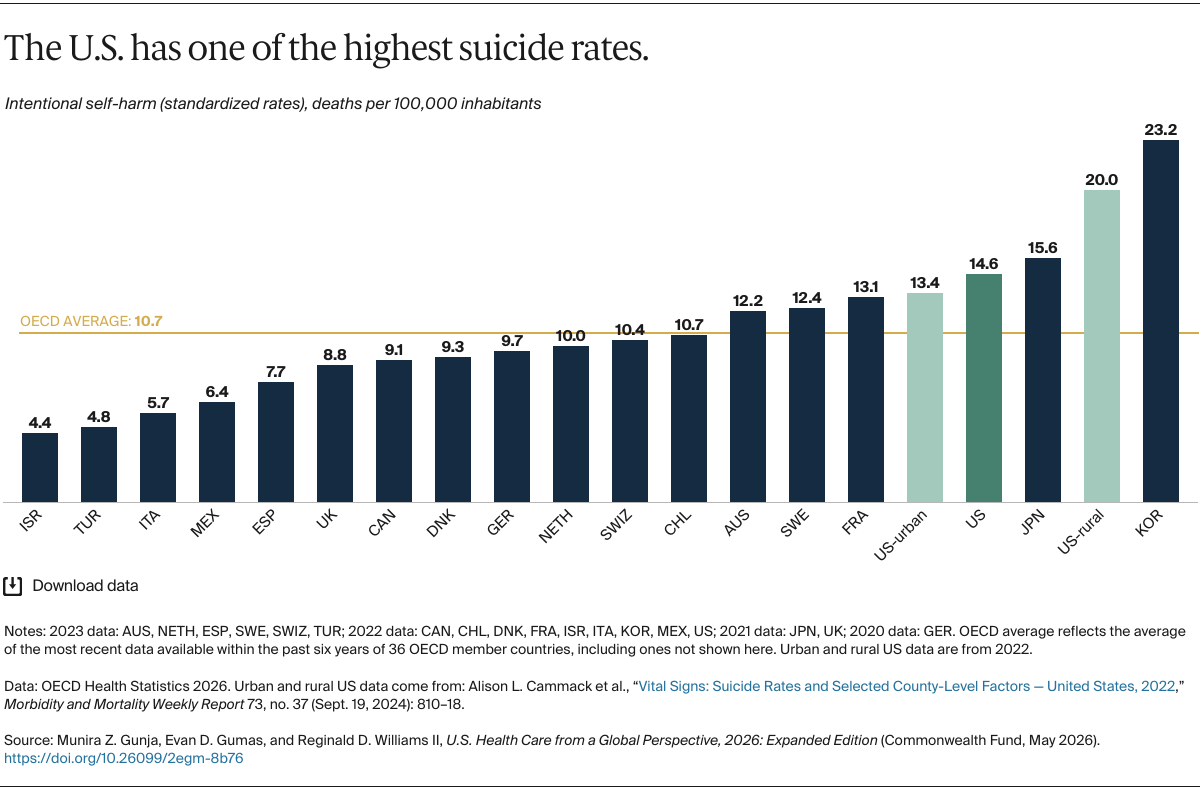
Elevated suicide rates can indicate a high incidence of mental illness. The U.S. has the third-highest suicide rate. Rates in Korea, which are the highest, are the result of cultural factors like high alcohol use and a stressful work culture.
Suicide is a leading cause of death in the U.S. Rates are consistently higher, and rising faster, in rural areas than in urban areas: Americans in rural communities are one-and-a-half times more likely to die by suicide than their urban counterparts. Regardless of demographic characteristics, rural Americans are less likely to have access to adequate physician and mental health services and are more likely to experience challenges such as depression and loneliness.
Discussion
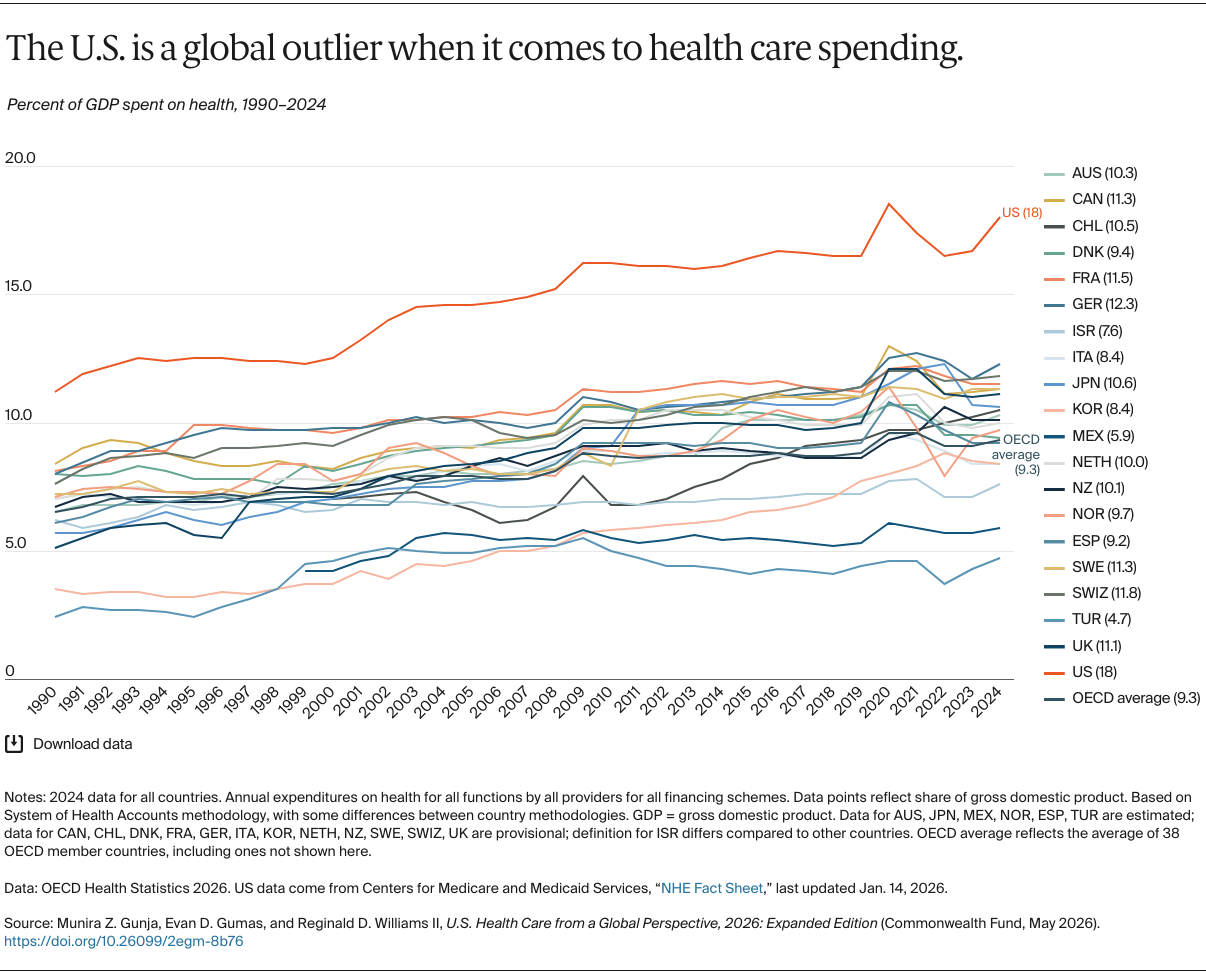
Although the United States spends more on health care than any other country, it consistently underperforms. If the U.S. is to achieve health outcomes on par with its international peers, it will be critical to closely monitor changes in access, affordability, care delivery, and inequities in outcomes and to continue tracking health system performance against other nations.
Insurance Coverage and Access to Care
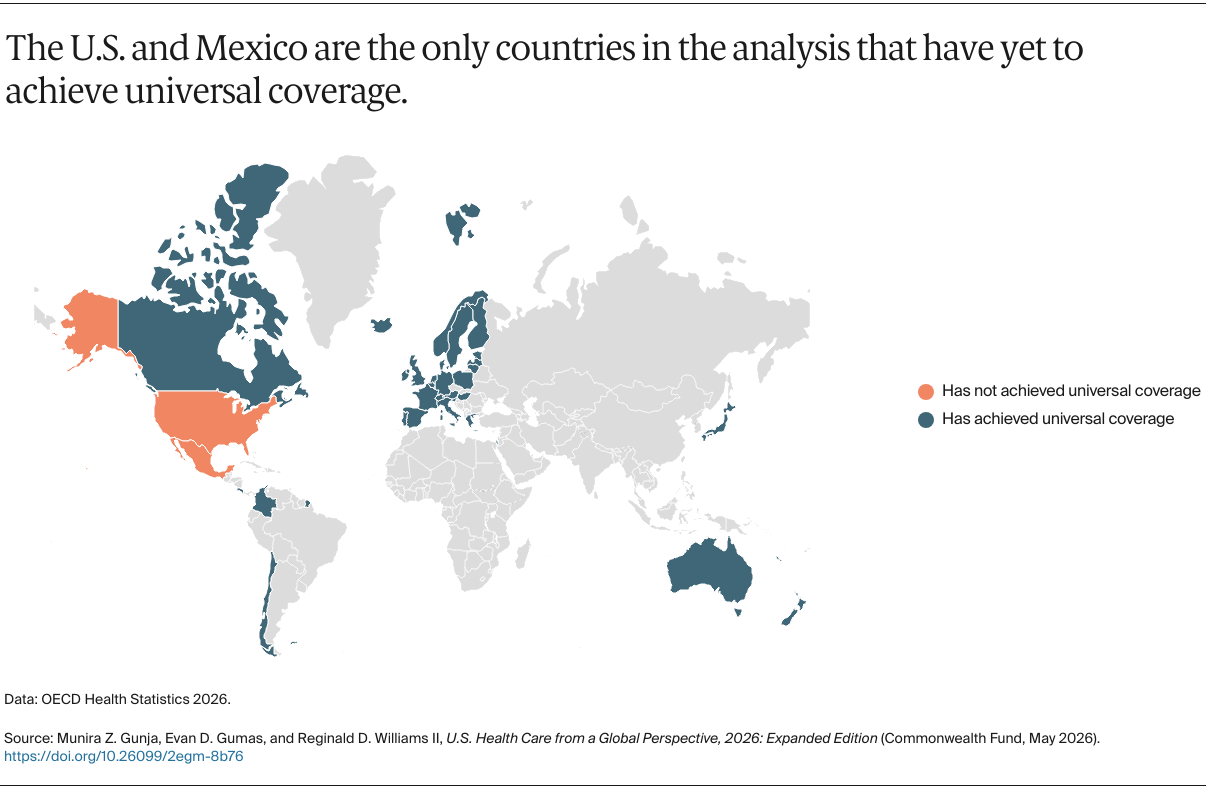
Except for the U.S., all countries in our study have achieved universal health coverage or are on the path to achieving it. While benefit packages vary across these countries, each provides comprehensive coverage for essential services, including preventive, primary, pharmaceutical, and maternity care. These services are fundamental to early disease detection, prevention, and long-term care management. The U.S. is one of the only countries to have enacted policies that reduce coverage. Other nations have implemented reforms over time aimed at expanding and strengthening coverage. For example, this year, Mexico established the Servicio Universal del Salud (Universal Health Service), which will gradually allow residents to get free care at any public health institute, starting in 2027.
Recent policy changes enacted by the Trump administration and Congress will push the U.S. even further away from universal coverage. After years of progress in increasing access to comprehensive health insurance through the Affordable Care Act (ACA) marketplaces and expanded eligibility for Medicaid, new changes to the marketplaces and substantial cuts in federal funding for state Medicaid programs are projected to increase the number of uninsured Americans by an additional 17 million by 2034. This will effectively return the nation to pre-ACA coverage levels and could potentially lead to over 50,000 additional preventable deaths annually. Marketplace enrollment is projected to decline by at least 17 percent in 2026 compared to 2025.
To ensure greater access to coverage, as a starting point U.S. policymakers could expand Medicaid eligibility in the 10 states that have not yet done so. This would at least ensure that the 1.4 million people with the lowest incomes have access to comprehensive health care.
Affordability of Care
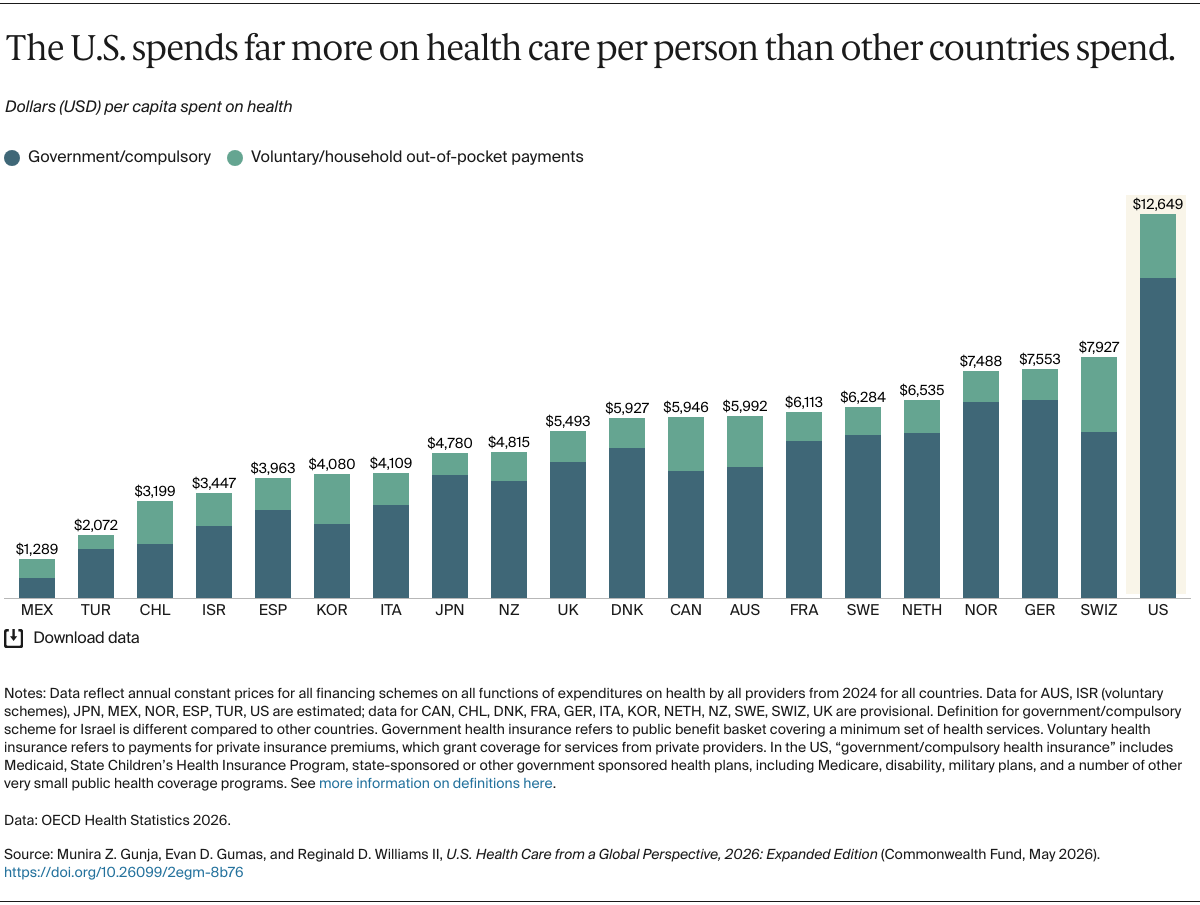
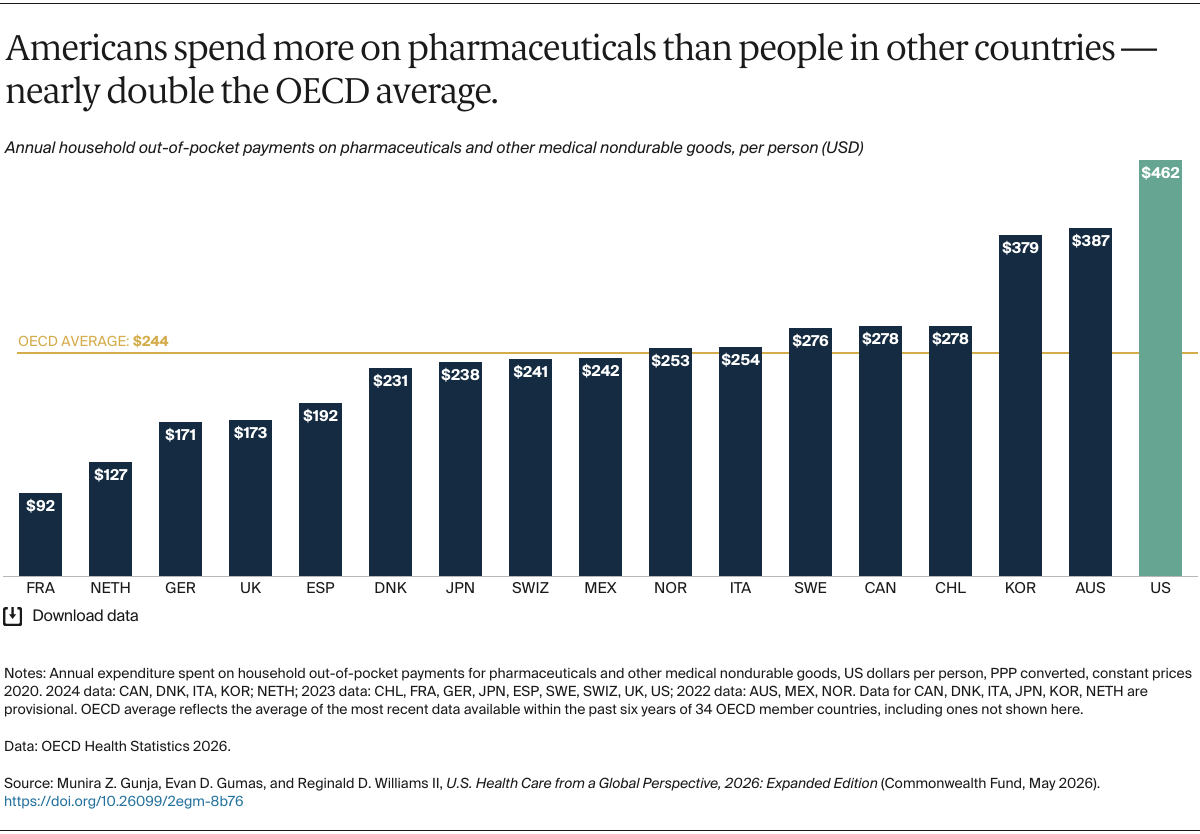
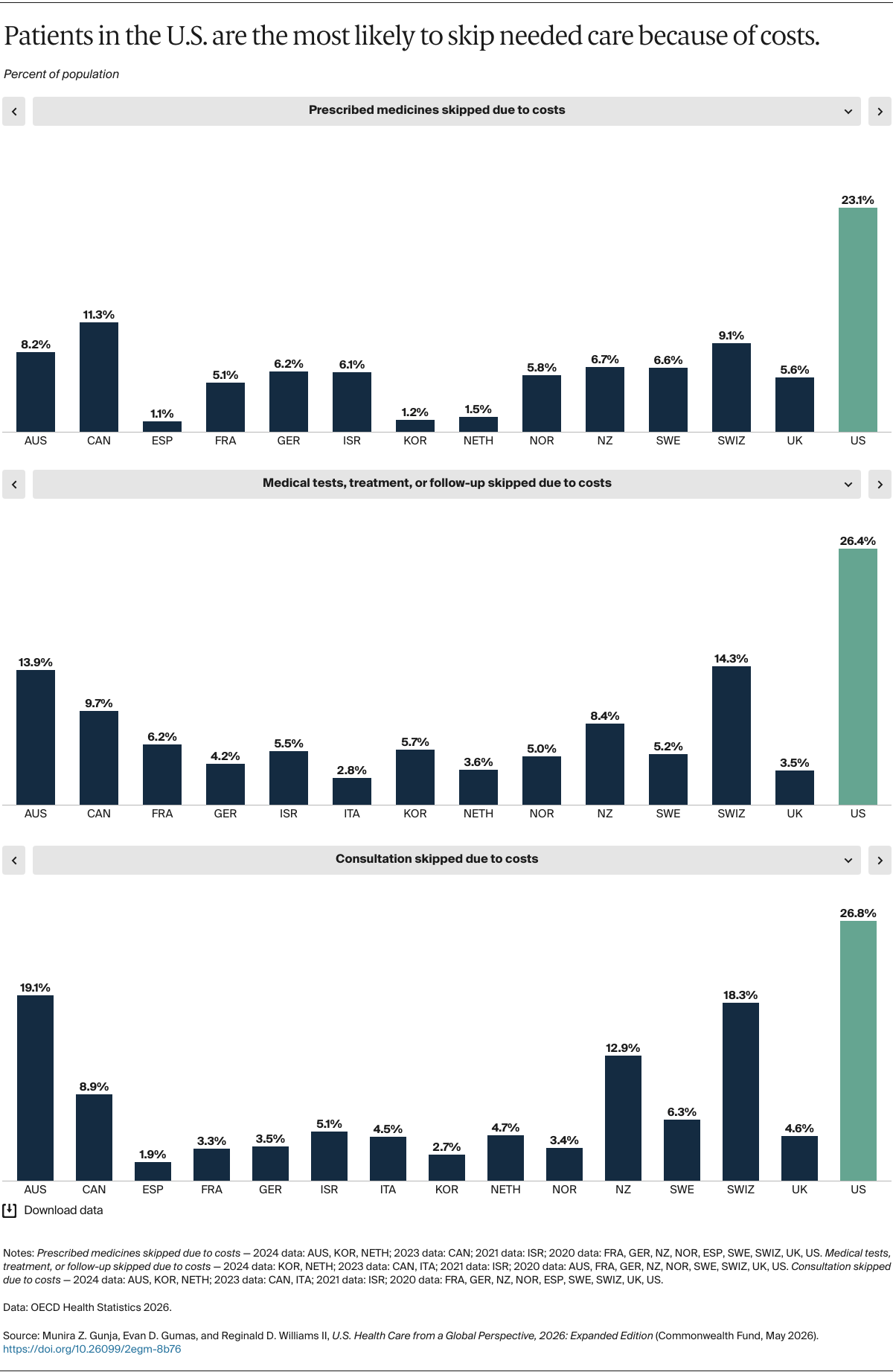
U.S. health care is likely to continue to underperform until policymakers and health care leaders address the rising cost of health services. Despite high levels of government spending per person, Americans face the highest out-of-pocket costs for health services and prescription medications. These costs lead more people in the U.S. to forgo needed care than in other high-income countries.
The U.S. can increase access to affordable health coverage by reducing deductibles and out-of-pocket costs for ACA marketplace plans, including by extending cost-sharing reductions to middle-income individuals. In addition, the introduction of new public plan options and limits on prices set by commercial insurers could curb growth in health care costs.
Although the Inflation Reduction Act caps Medicare beneficiaries’ annual out‑of‑pocket drug costs, and cut the price of the first round of 10 negotiated drugs, the Trump administration’s “Most Favored Nation” proposal, which ties U.S. drug prices to those paid abroad, cannot replace the institutional processes used to assess value and negotiate prices.
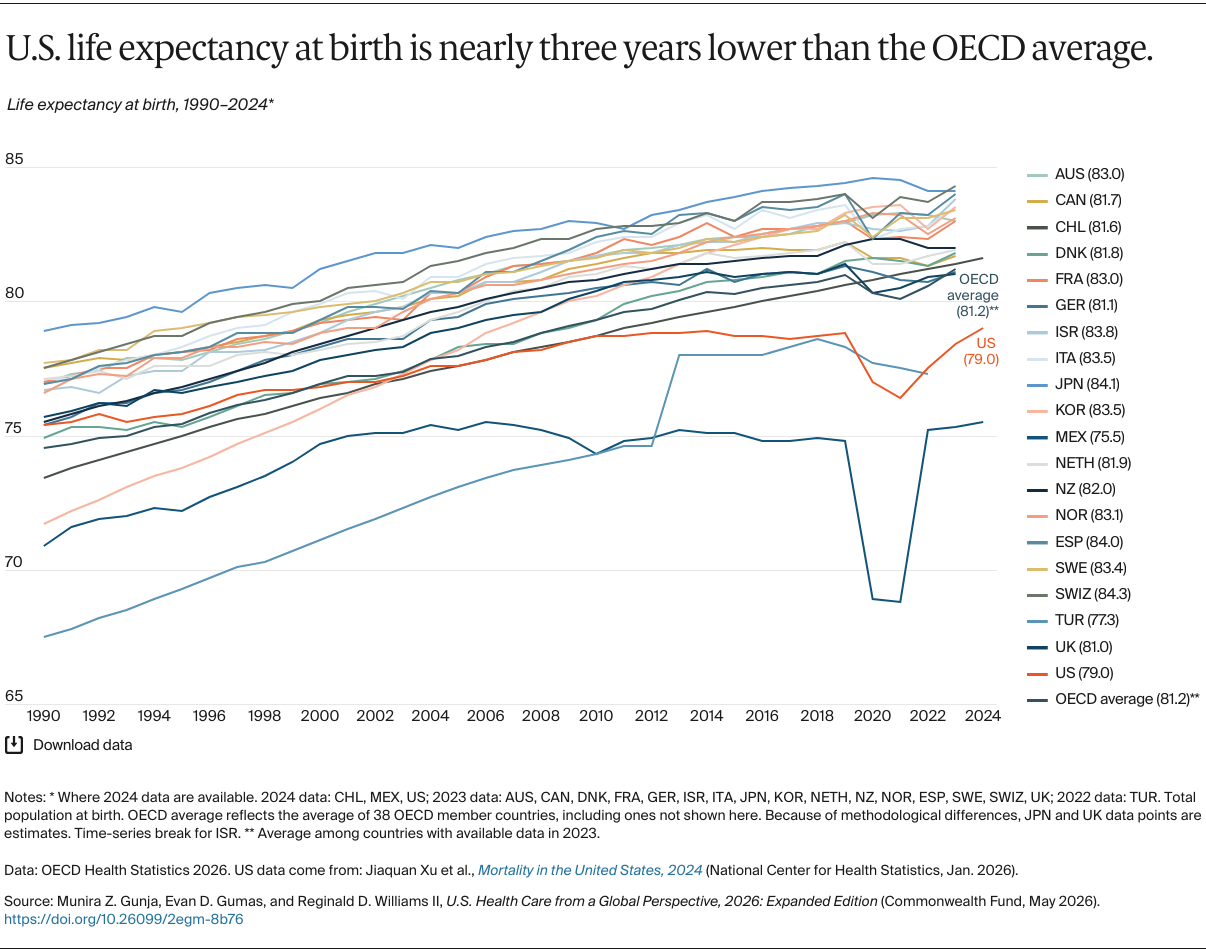
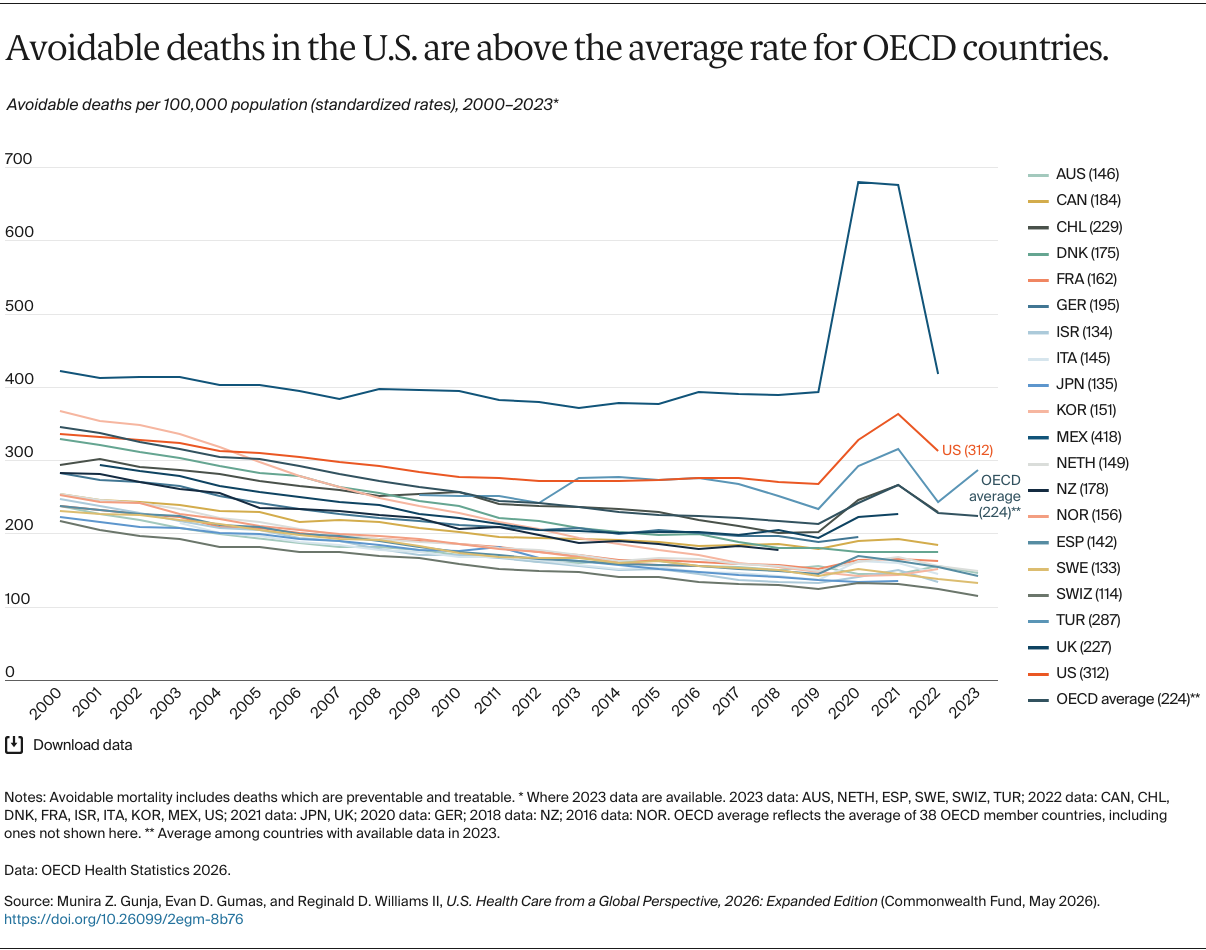
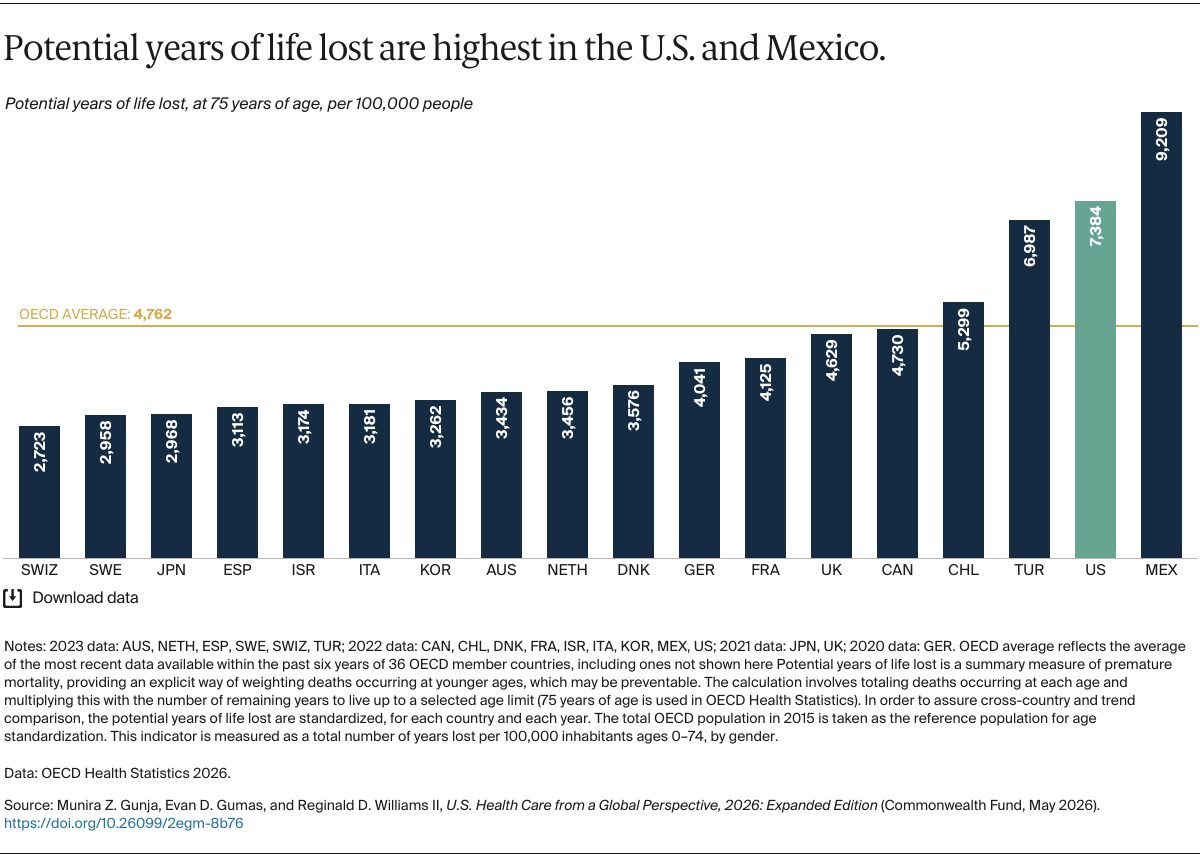
Many nations have implemented strategies to contain costs, even as health care spending has risen globally. Spain, for example, spends far less on health care than the U.S. yet achieves some of the best health outcomes in the world, including high life expectancy and a low rate of avoidable deaths. Its decentralized health system contains health spending by allowing the country’s autonomous communities to manage the planning, budgeting, and purchasing of health care within defined funding allocations. In this way, the government promotes targeted spending aligned with regional needs.
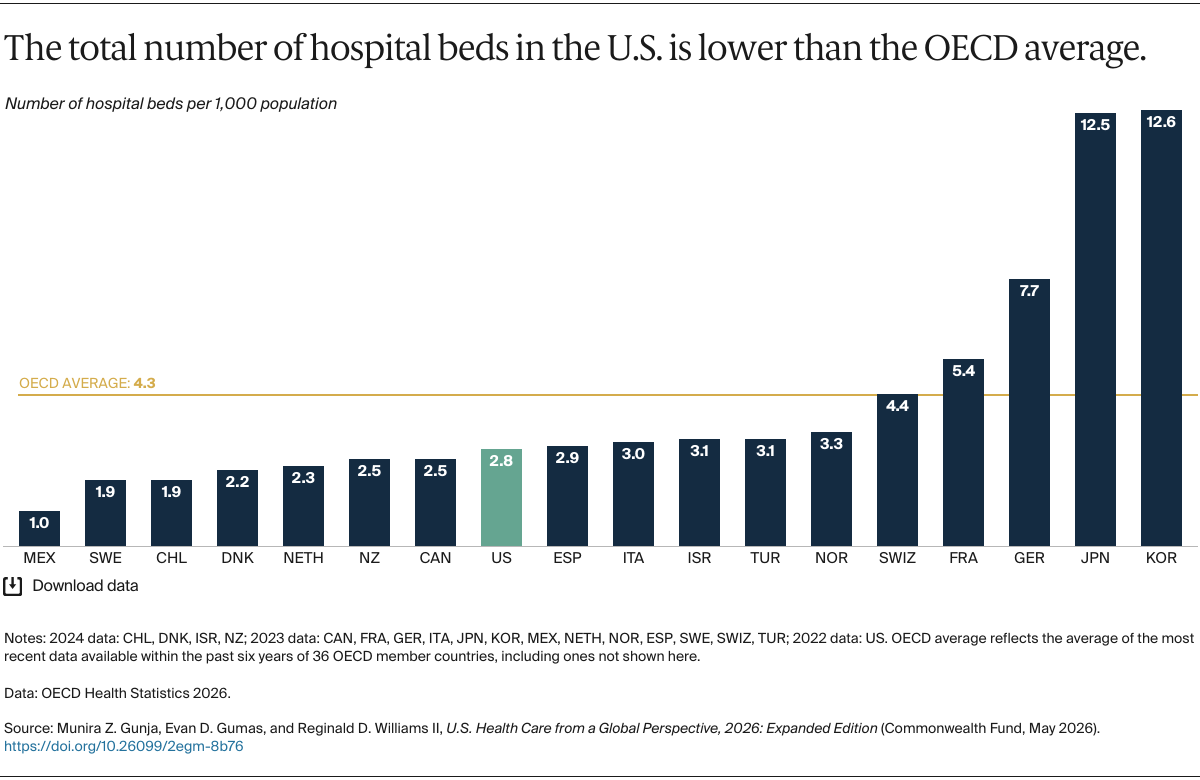
Similarly, Denmark sets spending global budgets for regions and municipalities. The government also incentivizes shifting from inpatient to outpatient care. Additional efforts include value-based payment models that emphasize patient outcomes rather than service volume, as well as integrated care models that foster collaboration among primary care providers, specialists, and hospitals. Together, these approaches reduce fragmentation in care delivery, limit duplication of services, and help control costs without compromising quality.
Delivery of Care
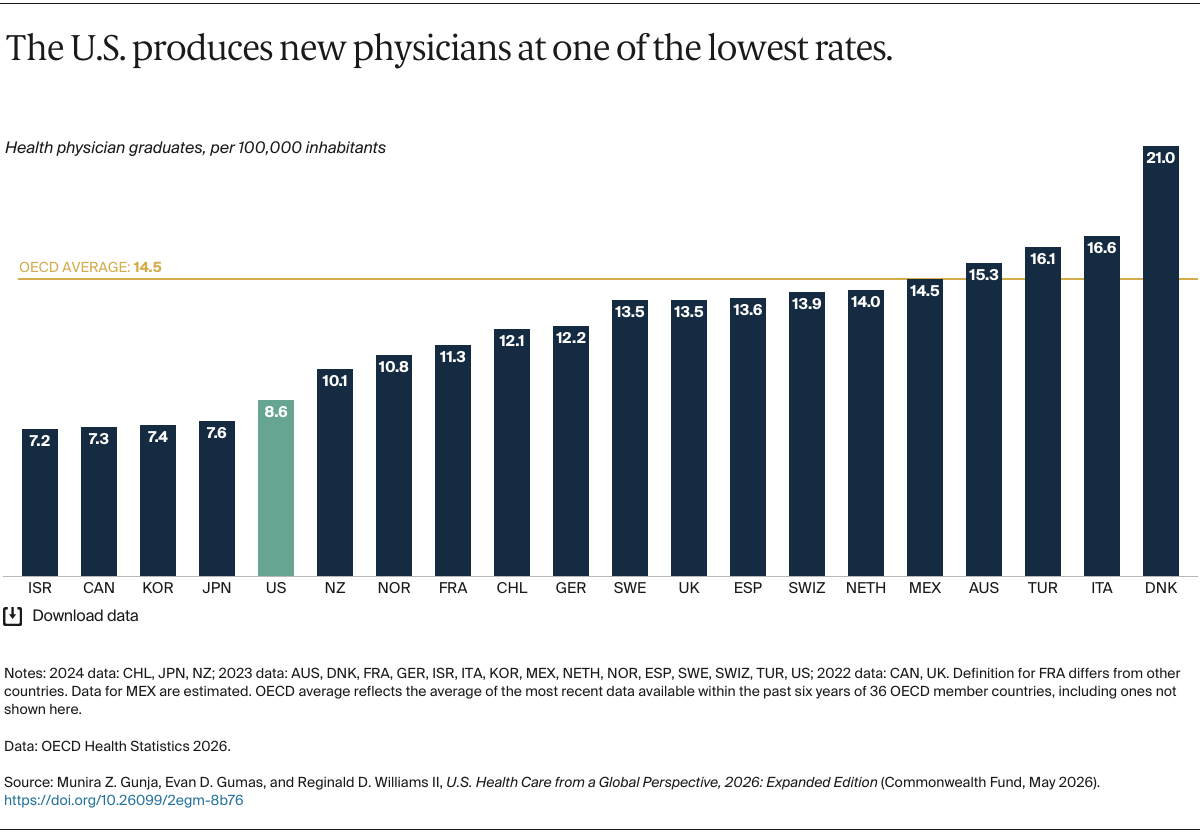
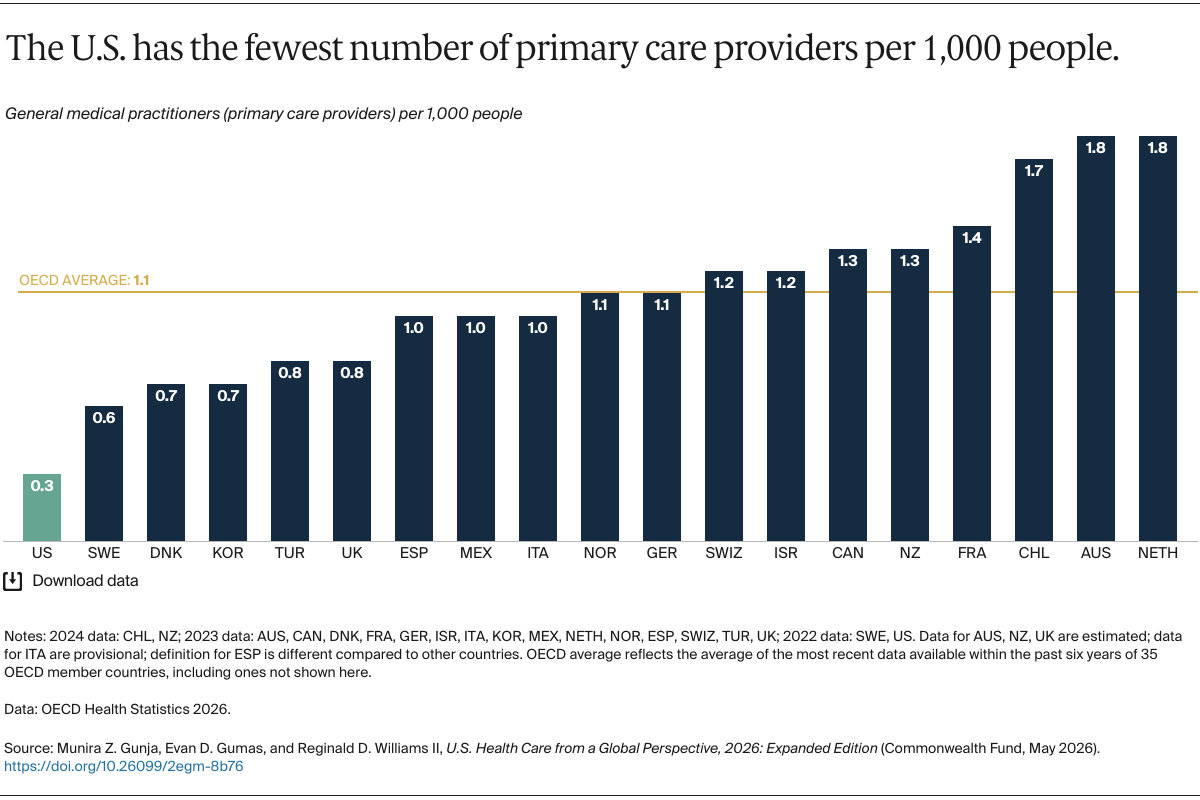
Decades of underinvestment in primary care, coupled with an insufficient supply of primary care providers, have constrained Americans’ access to effective primary care. One hundred million people — nearly one-third of the U.S. population — are considered medically disenfranchised, meaning they lack a regular place to go for primary care. This can be a result of provider shortages, hospital closures, or unaffordable costs.
The U.S. needs to invest in, and improve, its primary care. Growing and retaining the workforce will require enlisting additional types of health professionals to meet the nation’s primary care needs, as well as catalyzing uptake of innovative, evidence-based models, including team-based, person-centered primary care. This also extends to appropriate use of technology, including artificial intelligence; the integration of behavioral health into primary care to meet substance use and mental health needs; and broad access to comprehensive reproductive and maternal care.
Chile is a country that has made substantial progress in delivering primary care to its people. On the supply side, the nation has one of the highest numbers of primary care physicians per capita. Since 1990, Chile has added more medical schools and increased enrollment, strengthening its physician pipeline. About a quarter of the health care workforce receives its training internationally, with many providers coming from neighboring countries to fill workforce gaps. Chile’s supply of physicians is projected to expand to six per 1,000 people — above World Health Organization benchmarks.
Since 2005, Chileans have received their primary care through the Comprehensive Family and Community Health Care Model, which emphasizes person‑centered care. This approach to care not only meets patients’ physical and mental health needs but also takes into account their cultural background, family dynamics, and community environment.
Equity of Outcomes
On several of the health system measures we examined, the U.S. has some of the widest demographic and regional disparities in health outcomes, while Sweden has some of the smallest disparities. To help ensure equitable access to medical services, Sweden’s investments in digital health, especially telemedicine, have helped bridge gaps in sparsely populated northern areas by reducing travel burdens and improving access to primary and specialist care. While disparities are less pronounced in Sweden, the country may still be falling short in achieving its goal of eliminating avoidable inequalities by 2048.
Conclusion
Findings from this international comparison highlight a persistent failure of the U.S. health system: Americans pay more for health care, get less in return, and remain far more exposed to illness, debt, and insecurity than their peers. Recently enacted and proposed federal policies fail to address this contradiction head on. Instead, they sharpen it, leaving more Americans uninsured and exposed to costs they cannot afford. Over the next several years, it will be important to measure the impact of these policies against progress internationally. Yet comparison alone is insufficient: the U.S. must build a system that delivers care rather than financial ruin.
Other nations have made different choices. What’s remarkable is not that alternatives exist, but that the United States has failed to pursue them.