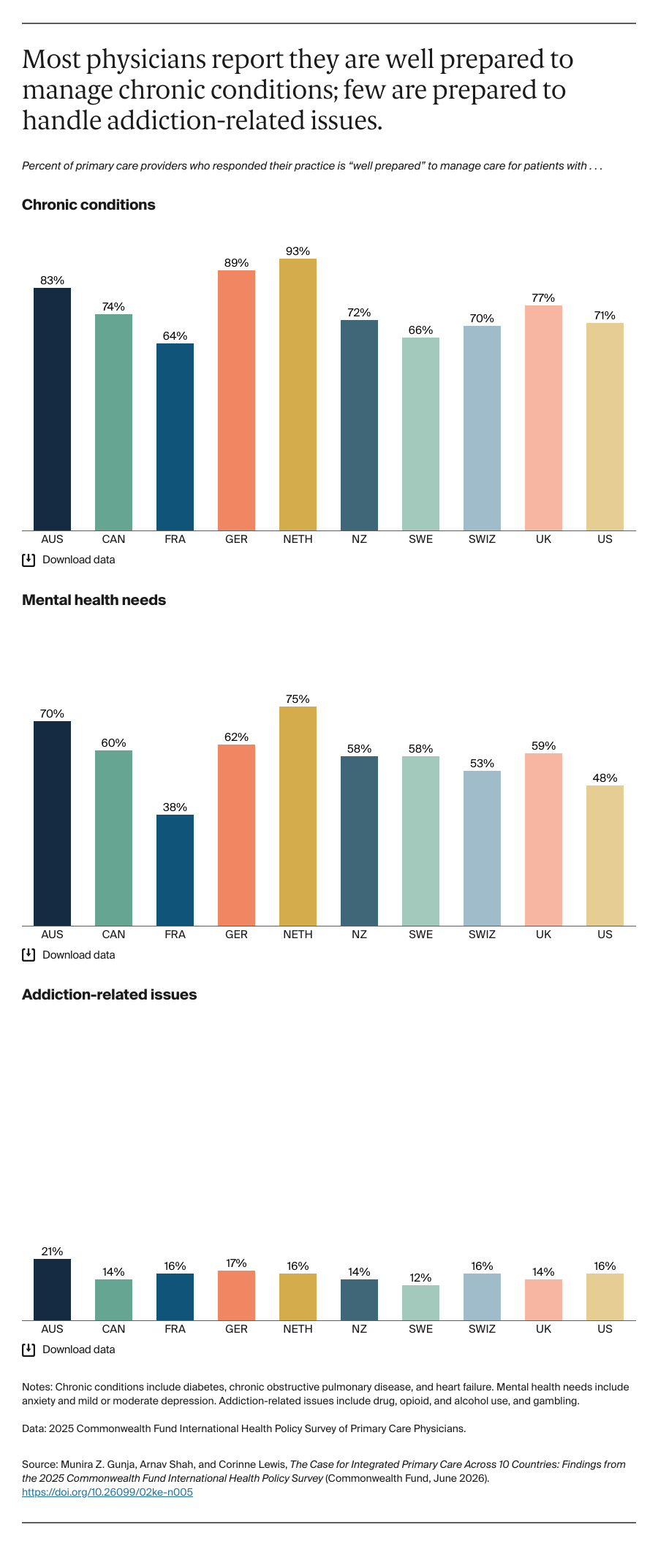
Despite differences in the composition of providers within primary care practices, a majority of primary care physicians in all 10 countries report feeling their practice is well prepared to manage care for patients with chronic conditions. This suggests the makeup of provider types is mostly sufficient to address these needs.
However, there is wide variation in how prepared physicians feel to address mental health needs. Less than half of physicians in France and the U.S. felt well prepared, while three in four physicians in the Netherlands reported feeling well prepared. Among physicians in all countries who reported feeling ill prepared, the most cited reason was a lack of available services or specialists to refer their patients to (data not shown).
When it comes to addiction-related issues, few physicians across countries feel adequately prepared to provide treatment. Among physicians in all countries who reported feeling not prepared, the most cited reasons for this were a lack of knowledge or skills needed to treat these conditions and a lack of services or providers to refer the patient to (data not shown).
Discussion and Conclusion
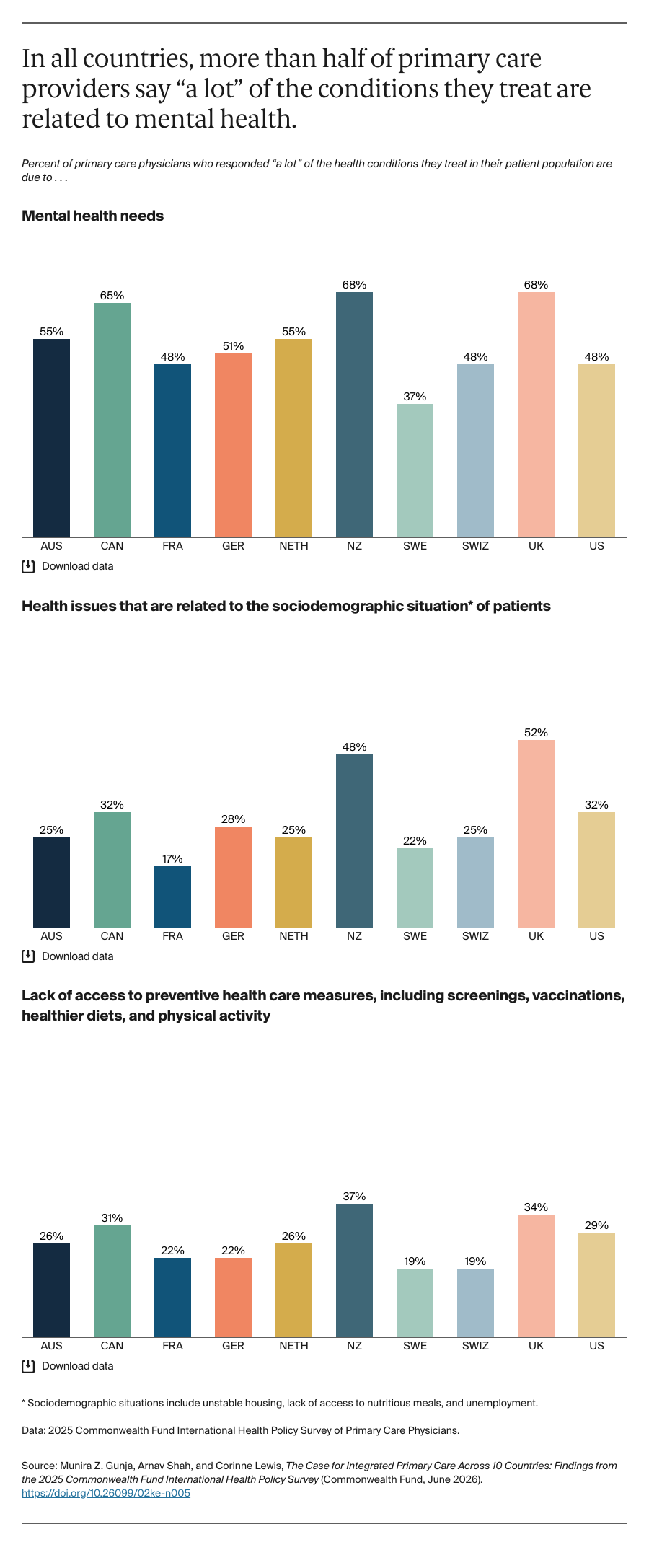
Across countries, a substantial amount of unmet patient health needs within primary care practices stems from insufficient preventive care and unaddressed mental health and social needs. Yet there is wide variation in how prepared physicians feel to address these needs. If primary care providers do not feel adequately equipped to provide this type of support, their patients may be less likely to receive high-quality, comprehensive, and continuous care. Additionally, providers may be more prone to burnout when forced to provide care beyond their capacity.
Expanding primary care teams can improve access and patient outcomes, and addresses workforce shortages. Extensive research shows that expanding primary care teams to include a broader mix of provider types can ease the pressure on physicians to manage all aspects of patient care. Expanding the role of highly trained nurse practitioners and physician assistants — who can provide care comparable to primary care physicians — can help address the growing shortage of primary care providers. Other countries have already moved in this direction. The Netherlands, for example, extended the autonomous scope of practice of nurse practitioners and physician assistants in 2018, while the United Kingdom gave nurses full prescribing authority in 2006.
Likewise, integrated primary care can also expand access to mental health and social services, particularly for racial, ethnic, and geographic minorities, improving overall health outcomes. In Germany, for example, where about half of providers reported that “a lot” of their patients have mental health needs, almost no primary care phycicians report that their practice includes mental health providers on their staff. In New Zealand and the U.K., where about half of physicians reported that “a lot” of their patients’ health issues stem from social and economic conditions, only about one-quarter of primary care physicians report that their practice includes social workers.
Efforts are underway to advance team-based primary care in the U.S. The decades-long Patient-Centered Medical Home Recognition program, developed by the National Committee for Quality Assurance, encourages practices throughout the country to employ a team-based approach to care through enhanced communication, task delegation, and coordinated care transitions and referrals. The Collaborative Care Model, when adopted by primary care practices, allows patients to receive care from their primary care team, a behavioral health care manager, and a consulting psychiatrist. Psychiatrists can therefore see more patients than in a typical one-on-one setting, and patients show better short- and long-term mental health outcomes, and are less likely to go to the emergency room. Community health centers, which provide care for underserved patients and communities, have long embedded behavioral health specialists and other providers in primary care to meet the needs of their patient populations. In 2024, Medicare expanded the types of providers that can bill for behavioral health services and began covering peer support specialists and community health workers.
Still, several barriers hinder the expansion and integration of primary care in the U.S.:
- Effective integration requires significant upfront costs to hire and train staff, implement shared health information systems that ensure strong communication and collaboration across the primary care team, and develop new quality improvement processes. This kind of infrastructure is generally not reimbursable and can have ongoing costs that may be difficult for practices to afford.
- By reimbursing providers for individual services rather than the whole-care experience, the country’s traditional fee-for-service payment model discourages integrated, team-based care.
- The growing underinvestment in primary care makes it difficult for practices to meet the comprehensive needs of their patients. Since 2019, investment in primary care has steadily declined across all health care payers.
- Twenty-three states still require physician supervision for nurse practitioners, rather than granting them the autonomy to diagnose, treat, and prescribe for a defined set of conditions without physician oversight.
In the United States, policymakers can support team-based care models by expanding and increasing payment for primary care to cover the full range of services delivered by interprofessional teams and increasing investment to attract more professionals to the field. Adopting value-based payment models, which pay providers based on the quality and outcomes of care they deliver, can also reward care integration. Finally, providing training for primary care professionals to strengthen team-based care and tracking progress over time are critical.
The composition of primary care teams varies widely between countries, and no country is fully prepared to meet patients’ needs across the spectrum of care. We know that expecting already-stretched physicians to deliver the full range of primary care services is not conducive to high-quality patient care. Ensuring primary care practices comprise diverse provider types — including behavioral health specialists equipped to handle mental health and social issues — is essential for meeting patients’ needs and alleviating some of the burden on overstretched physicians.