As part of 2025 budget reconciliation, Congress is expected to consider unprecedented cuts to Medicaid funding, with several House members stating their intention to “fix flaws in the program that divert resources away from children, seniors, individuals with disabilities, and pregnant women.” But to find places to save, in the face of massive federal funding losses, states will be forced to consider cutting any parts of the program that are not federally required. With everything on the table, children whose eligibility is not required by federal law are at risk of losing coverage.
Today, every state covers populations and services that go well beyond Medicaid’s minimum standards regarding which populations and services must be covered. Over the past four decades, as Congress has expanded Medicaid, states have been given important options for covering children and no group has seen more gains than children.
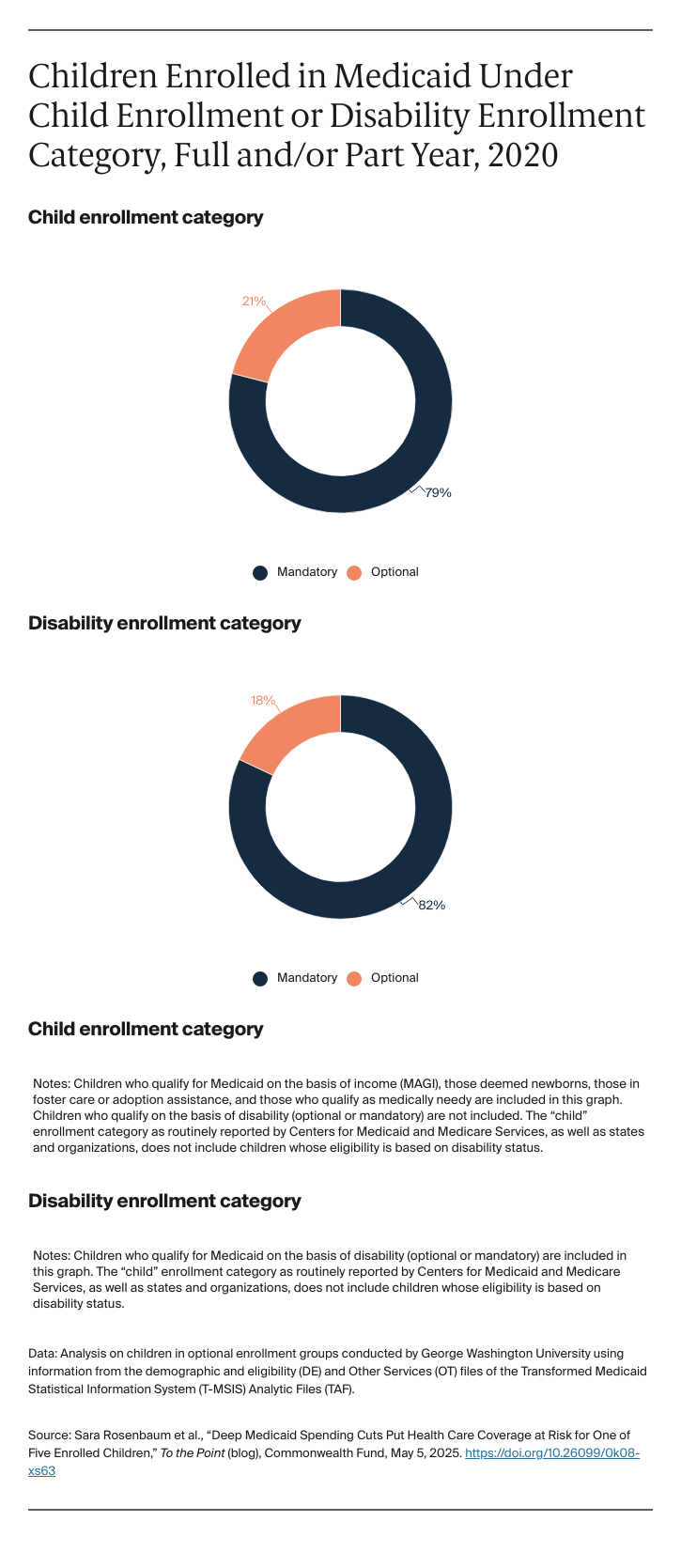
For children, state Medicaid coverage flexibility falls into three basic categories: children who live in families with low incomes (although higher than the minimum standard of 138 percent of the federal poverty level, or FPL — $36,777 for a family of three in 2025); children with severe disabilities who do not receive Supplemental Security Income (SSI) benefits but are at risk of being institutionalized and whose families face overwhelming medical bills for their care; and children in foster care or those whose families receive services aimed at keeping them at home, but are not poor enough to fall into Medicaid’s mandatory child welfare eligibility group. Coverage of these groups is optional, and at any time, states can change their Medicaid plans to drop coverage of children who fall into optional groups. For example, if a state covers children living in families with incomes up to 200 percent of FPL, it can eliminate children with incomes between 138 percent and 200 percent of FPL without risking loss of federal funding for children whose families have incomes at or below 138 percent of FPL. Similarly, a state can eliminate coverage for all children with severe disabilities other than those who receive SSI without jeopardizing its eligibility for federal funding for children who receive SSI (and whose coverage is mandatory).
One way to roll back coverage of even nonoptional (or mandatory) children is to do so indirectly; that is, by eliminating coverage of their parents. This would happen if states ended coverage of working-age adults made eligible under the Affordable Care Act (i.e., adults ages 19 to 64 with family incomes up to 138 percent of FPL). This group includes millions of previously ineligible parents who could not qualify under their state’s often alarmingly low eligibility rates for parents and caretakers. For example, Idaho’s mandatory parent eligibility group limits assistance to parents with incomes only up to 19 percent of FPL, about $3,000 for a family of three. Research shows that when parents gain coverage, their children do too. The converse is also true; as parents lose coverage, so do children, even if eligible. Children’s recent experience during the post-COVID Medicaid unwinding period shows how even eligible children can lose coverage during large-scale state reduction efforts. These inadvertent coverage losses can happen when states fail to separate out still-eligible children as they roll back coverage for their parents. Furthermore, because termination notices are so difficult to read and navigate, parents may not understand that their children remain eligible and may assume that the entire family has lost benefits.
States can also affect children’s coverage directly, by reducing or eliminating optional eligibility groups. Even though children are inexpensive to insure, their sheer numbers add up. Half of all children under age 18 are enrolled in Medicaid and the Children’s Health Insurance Program (CHIP). Furthermore, while most children are healthy, those with complex health care needs represent some of Medicaid’s costliest beneficiaries, especially when they need extensive care to remain at home. They are sometimes called “Katie Beckett” children, after a girl with severe disabilities who needed Medicaid to remain home with her family but could qualify only if institutionalized. This advance in coverage of children with disabilities, originally championed by President Ronald Reagan, has become a staple of modern state Medicaid programs
As of 2025, every state covers “optional” children. Furthermore, nearly all children insured through Medicaid, whether mandatory or optional, are entitled to comprehensive benefits known as Early and Periodic Screening, Diagnostic, and Treatment (EPSDT), which covers primary care and all medically necessary diagnoses and treatments that can be considered “medical assistance,” regardless of whether those services are covered for adults. To cover children, states use funds available through Medicaid and CHIP. This includes children in households with incomes above 138 percent of FPL and children in the child welfare system. States also can supplement EPSDT using Medicaid’s special waiver authorities to provide social and other supportive services that EPSDT does not cover, such as special equipment or building modifications (e.g., ramps) that may be needed to adapt a home to a child’s special needs.
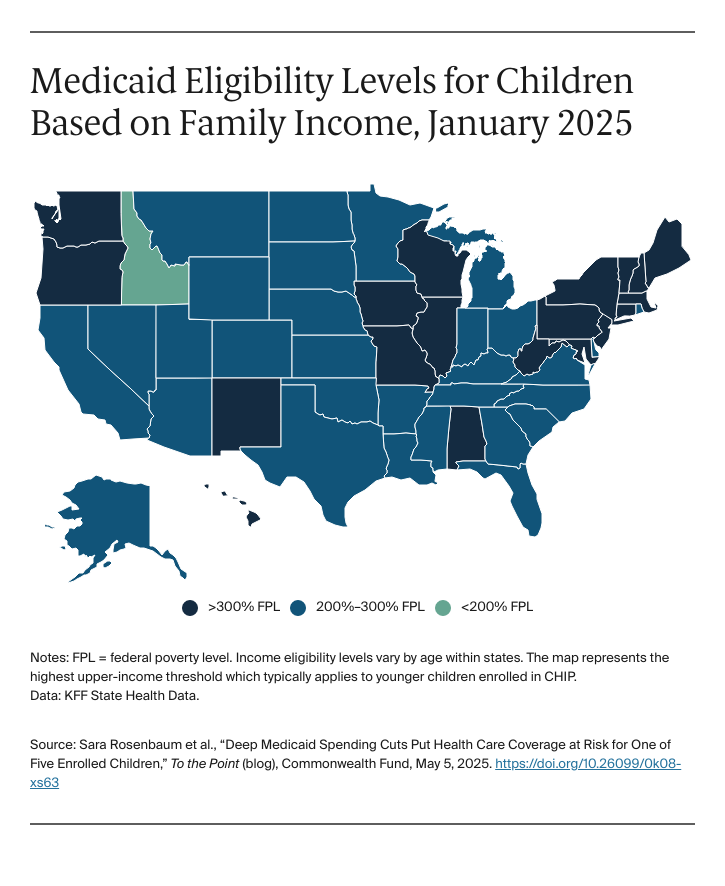
States go well beyond Medicaid’s minimum eligibility levels. In every state but Idaho, children in households with incomes at 200 percent of FPL ($53,300 for a family of three) are eligible. In more than a dozen states, children are eligible in households with incomes at 300 percent of FPL ($79,950 for a family of three). Using Medicaid and CHIP funds, in 2025, states set 217 percent of FPL as the median income level for infants and children ages 1 to 5 and 168 percent of FPL for children ages 6 to18. Children who are eligible based on disability may have higher household incomes, since even solidly middle-class families face extraordinary costs linked to long-term services and supports.