



Racial and ethnic discrimination in health care settings contributes to poorer health outcomes in the United States and all over the world. In 2022, the Commonwealth Fund conducted two surveys, including qualitative components, to understand how U.S. health care workers view patient discrimination and explore potential solutions.
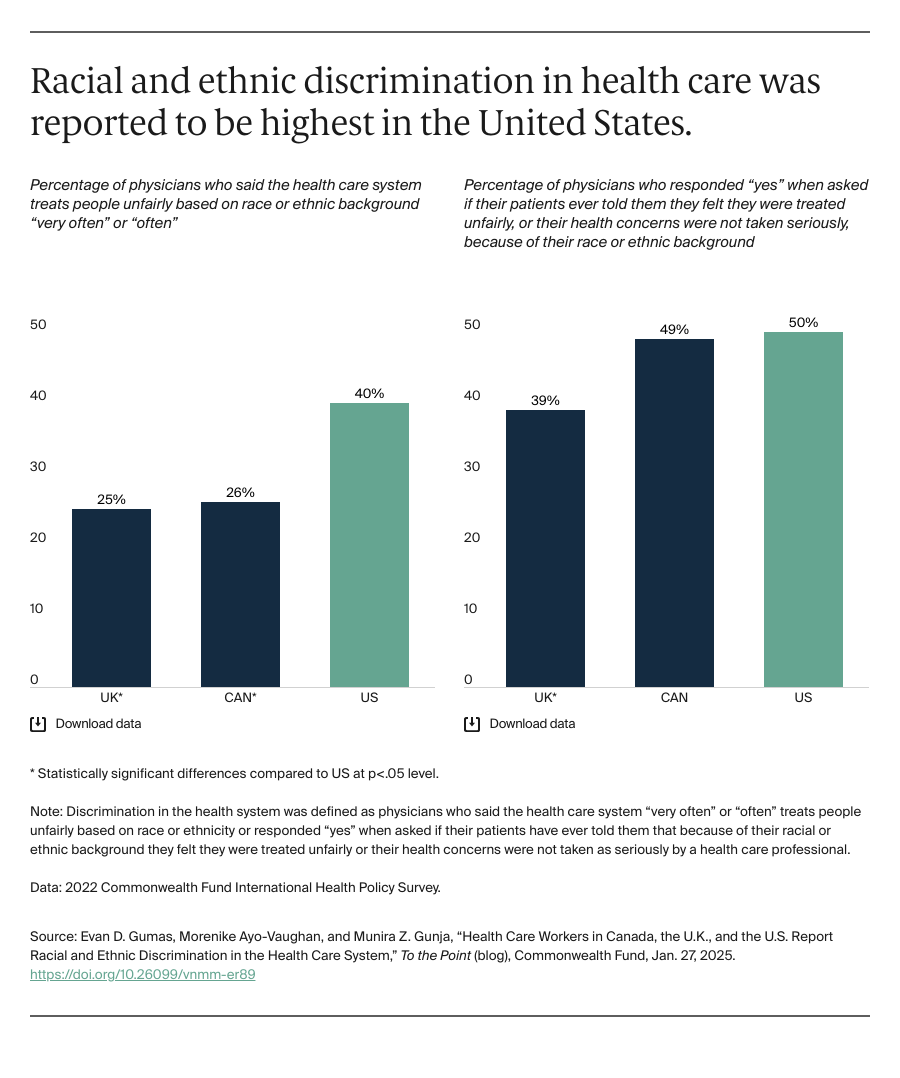
In the Commonwealth Fund’s international survey of primary care physicians, up to 40 percent of physicians in the U.S. reported that the health system treats people differently based on their racial or ethnic background, compared to 26 percent and 25 percent in Canada and the United Kingdom, respectively. In the second survey, a collaboration with the African American Research Collaborative, health workers said racism against patients is a major problem or crisis.
The survey findings highlight that discrimination in health care is a common problem, but not a uniquely American phenomenon. However, the negative impact discrimination has on the health of Americans is exceptional, as evidenced by our wide disparities in health and health care by race.
What Does Racial and Ethnic Discrimination Look Like in the Health Care System?
Differences in Treatment
Across the U.S., U.K., and Canada, health care workers reported that patients of color most often received inferior care or treatment that was different from what white patients received. In the U.S., Black and Latino health care workers indicated that discrimination directly affects the quality of care provided to patients of color. Examples of mistreatment include patients of color being less likely to receive pain medication compared to white patients and experiences of long wait times in the emergency room compared to white patients.
Language and Cultural Differences
Language and cultural differences are key determinants of discrimination for non-English speakers across the three countries. Most U.S. health care workers confirm that speaking languages other than English may lead to different treatment from health care providers. Likewise, all physicians in the U.K. and Canada noted language being the largest reason for discrimination aside from race or ethnicity, while also noting that language and race and ethnicity are often intertwined.
Solutions from Health Care Workers
Delivery System Reforms
A reformed delivery system should focus on enhancing equitable access, reducing dependence on emergency services, and addressing the root causes of health disparities. Both U.S. and Canadian physicians highlighted historical racism’s lasting effects on health care discrimination. A lack of trust in the system can cause missed diagnoses and preventable chronic disease progression.
In emergency room (ER) settings, where physicians noted decisions are made quickly, racial and ethnic biases can result in lower-quality care for some populations. In fact, 38 percent of U.S. health care workers reported witnessing care disparities due to racial or ethnic discrimination in these settings.
While there are also reports of racism in health care in both Canada and the U.K., their populations are guaranteed universal health coverage. Lack of universal coverage compounds these disparities in the U.S., where people of color and people from lower socioeconomic backgrounds are less likely to have comprehensive insurance. As a result, many are forced to seek care in ERs, placing them in environments where discrimination is more likely to occur. Addressing systemic issues that result in unequal treatment, particularly for marginalized groups, should be paramount in reforming the health care delivery system.
Education and Training
Diversifying providers (in terms of race, ethnicity, language, cultural literacy, etc.) to reflect the populations they serve is key to building trust in communities. Across all three countries, health care workers indicated they preferred evidence-based trainings that account for real-life experiences and involve all personnel, from physicians to administrative staff. A diverse health care workforce has been shown to improve several aspects of care including patient access, experiences during care, and outcomes, particularly for patients of color.
Across both surveys, health care workers emphasized the need for medical, nursing, and other health professional schools to include courses on discrimination, race, and racism and to make them required for all students.
Changing the Culture
At the health system level, leaders can provide an easy way for patients and health care staff to anonymously report experiences of racism or discrimination. Health care organizations should regularly conduct comprehensive reviews of their policies and procedures to ensure they are oriented toward equitable health care outcomes for patients of color as well as equitable treatment of health care workers.
Additionally, health care workers emphasize the importance of top-down changes, including increased access to health care or universal health care.


