Boston University School of Medicine students participating in an event commemorating lives lost to racism. Photo courtesy of Boston Medical Center
Toplines
What are academic medical centers doing to confront racism in health care? Efforts range from examining patient experiences and the use of race in clinical diagnoses to changing hiring, promotion, and recruitment policies
While academic medical centers’ efforts to confront racism in health care build on earlier diversity and health equity initiatives, what seems new is the explicit naming of racism as their target
In the past few years, amid a pandemic that has taken a disproportionate toll on Black and brown people and a national reckoning on racial justice, leaders from several U.S. health systems have named racism as a public health threat and pledged to identify and reverse racist policies and practices in their institutions. As an example, in an open letter published last Juneteenth, leaders from 36 Chicago hospitals said it’s “time for action” and promised to “double down” on efforts to reduce racial health disparities among their patients, create more equitable workplaces for their employees, and invest in communities of color where many of their patients and staff live.
To understand how health systems are following up on their proclamations, we spoke to physicians and administrators affiliated with eight academic medical centers about their early efforts. Because these centers tend to have more resources than other health systems and often serve large numbers of patients of color, it’s not a surprise they seem to be leading antiracism efforts. In several institutions, this work has been spurred by medical students or residents demanding change.
We found that in addition to examining how racism affects their patients, a number of academic medical centers are reviewing policies related to hiring and promotion and finding ways to better support staff of color. As part of strategies to build welcoming, inclusive workplaces, many are offering training courses on implicit bias and antiracism principles. Leaders are also looking at policy changes and new ways of tackling long-standing goals, like recruiting more medical students or clinicians of color.
While these efforts build on earlier diversity and health equity initiatives, what seems new is the explicit naming of racism as the target and the greater urgency to find and implement solutions.
Strategies for Combatting Racism in Health Care
Examining institutional policies with an equity lens
Establishing accountability frameworks such as equity scorecards
Auditing medical school curricula for erroneous references to race
Reviewing clinical algorithms that erroneously rely on race
Investing in scholarships for students of color interested in health professions
Training leadership and staff in diversity, equity, inclusion, and antiracism principles
Creating real-time reporting initiatives to track and respond to racist or other discriminatory behavior
Reviewing vendor relationships to support Black and other minority-owned businesses
Creating more equitable workplaces, including efforts to build wealth and opportunities for advancement
Listening to and learning from patients and health care professionals of color
Based on interviews with leaders from Massachusetts General Brigham, Northwestern University Feinberg School of Medicine, Ohio State University Wexner Medical Center, Penn Medicine, Rush University Medical Center, UCLA Health, University of Chicago Medicine, and the University of Pittsburgh School of Medicine.
Detecting Racism in Real Time
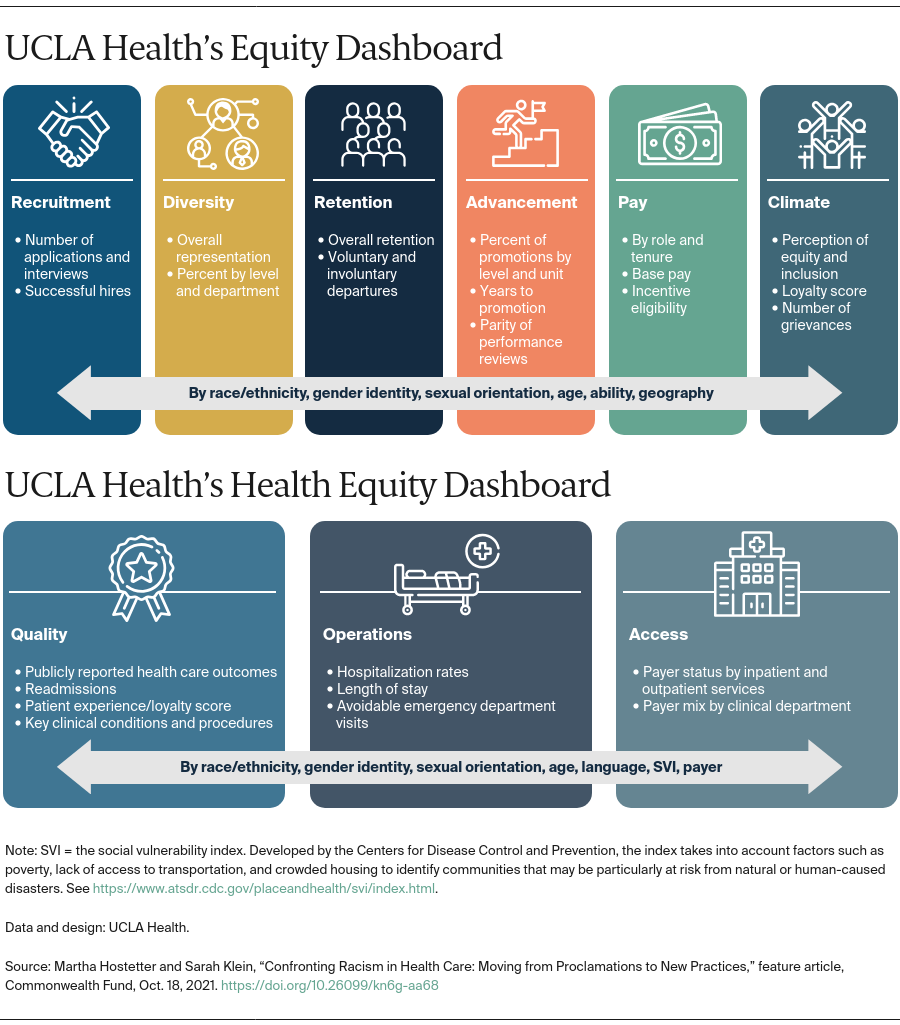
Several academic medical centers are developing tools such as equity scorecards and real-time reporting systems to identify racism in their policies and practices and to assess their effectiveness at addressing it. Leaders at University of California Los Angeles (UCLA) Health, for example, have created equity dashboards to detect variation in patients’ health care quality or outcomes by race, ethnicity, gender identity, age, sexual orientation, and community-level social vulnerability. The goal is to use the dashboards to identify inequities and find ways to mitigate them.
The dashboards also monitor variation in the health system’s hiring, promotion, training, and contracting practices. Among other metrics, they track racial and other differences in patient and employee grievances, promotions, and vendors providing goods and services. “We believe that inclusive excellence, equity, and justice should be intertwined into all of the practices, policies, and operations of the health system. It cannot be performative,” says Medell Briggs-Malonson, M.D., M.P.H., UCLA’s new chief of health equity, diversity, and inclusion. The dashboards will be reviewed every month by members of UCLA’s newly formed equity council, which includes Briggs-Malonson, the health system’s president, and 25 to 30 other leaders from across the system.
UCLA is also changing how race and ethnicity data are collected, asking patients to identify themselves rather than relying on staff to take their best guess. “We are taking steps to collect demographic data from patients based on the race and ethnicity categories they identify with, not on the standard categories defined by the government. Allowing patients to self-identify will bring greater accuracy and relevance to the data,” says Briggs-Malonson.
Leaders at Penn Medicine, meanwhile, are encouraging staff members who have witnessed or experienced racism in the workplace to recognize and report it. They are piloting a digital platform, Lift Every Voice, that will give staff at two emergency departments — including physicians, nurses, technicians, environmental service workers, and unit clerks — an easy way to make anonymous reports when, for example, managers treat Black employees unfairly or Black patients receive disparate treatment from staff. The goal is to create a mechanism for employees to have their concerns heard without filing a formal complaint with human resources.
The referenced media source is missing and needs to be re-embedded.
Eugenia South, M.D., M.S.H.P., assistant professor and vice chair for inclusion, diversity, and equity, emergency medicine at Penn Medicine
“We know that experiences of racism happen all the time. For some people, it’s daily and for others it is not as frequently as that, yet leaders often have a blind spot with regards to what is happening on the ground in the workplaces they oversee,” says Eugenia South, M.D., M.S.H.P., assistant professor and vice chair for inclusion, diversity, and equity, emergency medicine at Penn Medicine and one of the developers of the platform.
By encouraging anonymous reports and asking respondents not to identify the people involved in an incident, the team developing the prototype hopes to call attention to the behavior itself and identify patterns that can be discussed among employees during huddles and at monthly meetings of a department’s senior leadership team. “We want to see if sharing these stories publicly can help people identify things that they might not understand or realize are forms of racism and act upon them,” says Lauren Hahn, M.B.A., innovation manager at the Penn Medicine Center for Digital Health.
While formal human resources (HR) avenues to report racism exist, they are underutilized for reasons including fear of retaliation, uncertainty that reporting will lead to timely or meaningful change, high levels of friction impeding the process, and a sense that many experiences do not warrant HR involvement.
Eugenia South, M.D., M.S.H.P.
Assistant professor and vice chair for inclusion, diversity, and equity, emergency medicine, Penn Medicine
A two-week pilot of the tool involving 15 people in one emergency department generated nine reports, including examples of disparaging remarks made about a Black patient and an instance of a manager reprimanding a Black employee but not a white one who did the same thing. If larger pilots of the tool are successful, the plan is to use it in all clinical departments at Penn Medicine and eventually offer it to other health systems and employers. “We hope to build a tool that will be relevant and useful to any workplace,” South says.
Lift Every Voice: Prototype
Penn Medicine has partnered with local artists of color to illustrate some of the reported incidents of racism. The illustrations will be posted on an internal Instagram-like platform through which users can scroll and leave comments. The goal is to spark dialogue about how best to respond to incidents like these. The artists have taken some creative license with the illustrations to preserve anonymity of the people reporting the incidents and to capture several themes at once.
This illustration, by Philadelphia artist Jude Marks, conveys the judgment of staff who couldn’t reach the mother of an emergency department patient in the middle of the night. Rather than assume she was sleeping, a member of the care team suggested she was just trying to get rid of her son.
The referenced media source is missing and needs to be re-embedded.
Illustration by Jude Marks
At UCLA, leaders created a real-time reporting system for students, staff, and clinicians to report incidents of racist and discriminatory behavior. As part of training on equity, diversity, and inclusion principles for all staff, faculty, and students, UCLA Health trainers are teaching the appropriate steps to take when such behaviors occur. The Ohio State University Wexner Medical Center is developing a similar approach, called “Stop the Line,” to encourage patients, community members, students, and clinicians to speak up when they witness or experience racism. Massachusetts General Hospital recently created a patient code of conduct, which clarifies there is zero tolerance for discriminatory behavior toward staff and allows for termination of patients who repeatedly break this code. In addition to helping people feel heard, leaders say these tools will enable them to track what’s being reported, identify patterns, and respond with broader interventions to change the culture of their workplaces.
Listening to and Learning from Patients
Patient-reported outcome measures (PROMs) are another tool for identifying variation in health outcomes by race and ethnicity. PROMs are standardized questionnaires that measure patients’ perception of their symptoms, functioning, and quality of life that have been validated in studies of patients with particular conditions. Using PROMs makes it easier for clinicians to recognize when treatment decisions reflect bias, says Rachel Sisodia, M.D., senior medical director for specialty care and patient-reported outcomes at Massachusetts General Brigham. “It’s been proven over and over that Black women who have chest pain radiating down their arm are less likely to get referred for a cardiac catheterization than white men. When you have a validated tool where all patients answer the same questions about their symptoms, you impede a clinician’s ability to inadvertently hurt someone with implicit bias.“
PROMs can also uncover problems that might otherwise go unnoticed. When Mass General Brigham researchers began looking at outcome measures collected at a subset of clinics, they discovered Black patients in waiting rooms were given a tablet for reporting PROMs only 58 percent of the time while white patients received one 74 percent of the time. “The reason I know that this was due to implicit bias and not patient refusal is that it took one week to fix the problem once the front-desk staff were made aware of the discrepancy,” Sisodia says. “That’s how implicit bias works; we can hurt people without being aware we’re doing it.”
PROMs can also correct erroneous assumptions about the root causes of health disparities. Sisodia and colleagues found Black women receiving care at Mass General Brigham were significantly less likely to get knee replacement surgery, even for significant knee arthritis, than white men. This finding held true irrespective of patients’ health insurance status, socioeconomic status, age, or comorbidity. In addition to raising concerns about disparate treatment in medicine (e.g., that Black women may be less likely to be referred to specialists), the PROMs revealed that Black women had much less social support. Nearly half of the Black women surveyed said they “never” or “rarely” had someone to help them if they were bedbound, compared to less than 25 percent of white women. “Asking patients these questions allows you to get under the hood and understand inequities in ways we couldn’t before,” Sisodia says.
But there are challenges to using PROMs more broadly to detect disparate treatment. Most of these measures were developed among English-speaking populations, and most focus on the outcomes of surgical procedures, which offer clear before-and-after comparisons, rather than chronic conditions. “Many patients who have endured structural racism are not going to get their knee replaced but they are going to have a chronic kidney disease or diabetes,” Sisodia says. “We need more PROMs for diabetes, rheumatoid arthritis, heart failure, asthma, and chronic kidney disease, among others.” Sisodia and her colleagues’ efforts to build PROMs for non-English-speaking patients have been thwarted by the unwillingness of electronic health record vendors to build portals in other languages, she says.
Examining the Use of Race in Clinical Diagnoses
Many health system leaders are taking a critical look at how patients’ race or ethnicity are used in clinical algorithms — often prompted by medical students and residents who are surprised when they hear about these tools. Clyde Yancy, M.D., chief of cardiology and vice dean for diversity and inclusion at Northwestern University’s Feinberg School of Medicine, notes a measure of pulmonary function still in use today dates to the 19th century, when it was used by eugenicists and some physicians to argue that enslaved Africans “were biologically adapted for work and biologically flawed for cognitive pursuits.” The measure — which adjusts results of spirometer tests based on the assumption that Black people have naturally lower lung function than whites — could cause serious problems to be missed.
Clyde Yancy, M.D., chief of cardiology and vice dean for diversity and inclusion at Northwestern University’s Feinberg School of Medicine. Photo: John Boehm
Not only do these race-based formulas propagate the false view of race as a biological, rather than a social construct, they can perpetuate racial disparities in access to care. For example, two formulas used to estimate how well someone’s kidneys are functioning report higher values (i.e., better functioning) for Black than white patients who have the same creatinine measurements. This means that Black patients whose kidneys are deteriorating may get referred later than white patients for specialist care or transplants, potentially affecting their quality of life and health outcomes. One study of nearly 10,000 Black patients found removing the race “correction” from the estimated glomerular filtration rate substantially changed diagnoses: the prevalence of chronic kidney disease (CKD) increased from 14.9 percent to 18.4 percent, and 29.1 percent of those with existing CKD were reclassified to more severe stages of the disease.
Several health systemshave recently stopped using the race “correction” in kidney assessments; one is Massachusetts General Brigham, where leaders are also reviewing other instances of “racialized medicine.”
In 2020, the House Ways and Means Committee put out a request for information about the use of race in clinical decision-making. The 19 responses they received from medical specialty societies and individuals illustrate broad consensus that race is often misused in diagnoses and risk assessments. But they also reveal some disagreement about how to do better, including concerns about the potential unintended consequences of too precipitously removing race “correctors.”
“When you asked health equity experts about this issue, universally they said we need to stop race correction,” says Michelle Morse, M.D., then a Robert Wood Johnson Health Policy Fellow working with Committee Chairman Richard Neal and now chief medical officer and deputy commissioner at the Center for Health Equity and Community Wellness at the New York City Department of Health. “And then when you ask more mainstream professional societies, they tended to think, well, you know, removing these race corrections might do harm and more research is needed. But my feeling is that we know race is a social and political, not biological, category. It’s time to move on. We can create better tools that don’t normalize racial inequities.”
The Association of Black Cardiologists called for smarter approaches, such as broadening the pool of patients included in clinical algorithms and doing more to take into account ways that patients’ social and clinical circumstances affect their health.
While race may be a social construct, racism has devastating impacts on the bodies of people of color. It is more appropriate and accurate ‘that clinicians and researchers focus on genetics and biology, the experience of racism, and social drivers of health inequities — and not race — when describing risk factors for disease.’
From the American Medical Association’s recently published Organizational Strategic Plan to Embed Racial Justice and Advance Health Equity, 2021–2023
As more clinical decision-making leverages artificial intelligence (AI), critics worry that racist assumptions are getting baked into AI tools, too. A 2019 study found that one algorithm used by health plans and systems to comb through population health data to identify patients who may need extra supports, like nurse care managers or health coaches, relies on medical costs as a proxy for health needs. The problem: on average, Black and other patients of color with chronic conditions use fewer medical services than white patients with similar conditions — not because they aren’t as sick but because they lack health insurance, don’t trust the system, or face other barriers. Use of the algorithm could therefore worsen health disparities between Black and white patients. In a commentary, one of the author’s studies suggests health systems should designate staff members to be stewards of how clinical algorithms and AI tools are used, regularly auditing their impacts to ensure accuracy and fairness.
Building Racially Diverse Leadership and Boards
In recent decades, manyhealth systems hired chief diversity officers to help recruit and promote more clinicians and leaders of color. But there’s clearly work to be done. In 2019, when Black and other racial minority groups made up about 39 percent of U.S. residents, they comprised only 19 percent of hospital boards and 16 percent of executive leadership roles.
Last year, leaders at University of Chicago Medicine changed their leadership recruitment approach: instead of just asking recruitment firms to identify minority candidates, they put out a request for information for search firms that had succeeded in placing diverse candidates. They eventually hired two new firms and, in fiscal year 2020–21, increased the percentage of senior leaders of color from 22 percent to 23 percent. By fiscal year 2025, the health system expects that 35 percent of senior leaders will be Black, Indigenous, or other people of color.
After recruiting a diverse pool of applicants, the health system took steps to reduce unconscious bias. Hiring decisions are now made using a blind process in which applicants’ names and other details not related to their experiences and qualifications are removed. University of Chicago Medicine also introduced unconscious bias training for managers who conduct job interviews. “One of the key problems in the process of promoting or hiring people of color is bias in the interview, from inconsistency in questions and using bias to make decisions to judging people based upon who’s more like me,” says Brenda Battle, M.B.A., R.N., senior vice president of community health transformation and chief diversity, inclusion, and equity officer at University of Chicago Medicine. To encourage promotion of internal candidates, the health system tied financial incentives for vice presidents to their success in achieving diversity recruitment, development, and promotion metrics.
Brenda Battle, M.B.A., R.N., senior vice president of community health transformation and chief diversity, inclusion, and equity officer at University of Chicago Medicine. Photo: John Boehm
Some health systems have created systemwide equity councils or workgroups in an effort to make antiracism efforts part of their clinical, educational, and research enterprises. Last year, Penn Medicine increased the number of vice chairs for inclusion, diversity, and equity from four to 18, representing all clinical departments. “The goal of deputizing these individuals is to help ensure that antiracism becomes a part of culture and that there’s a point person responsible for tracking metrics and being engaged,” says Raina Merchant, M.D., M.S.H.P., professor of emergency medicine at Penn Medicine’s Perelman School of Medicine. Each vice chair is determining the steps their departments will take to achieve the health system and medical school’s joint Action for Cultural Transformation. For example, the emergency department will be tracking results of a new program in which residents and fellows from racial or ethnic groups that are underrepresented in medicine receive mentoring from faculty peers.
Uncovering Racism in Workplace Policies and Empowering Staff
In many communities, health systems are among the largest employers, and careers in health care can be a way to lift people out of poverty. Several academic medical centers have recruitment programs that target residents in their neighborhoods, which are often home to many low-income families and people of color. MetroHealth, a public health system in Cleveland, Ohio’s Cuyahoga County, even has a magnet high school that offers students four years of hands-on training with health care staff.
But the health care industry is still broadly segregated along racial lines, with people of color, often women, performing the bulk of direct care (e.g., as home caregivers or nursing assistants) as well as doing the cleaning, cooking, and other housekeeping while earning far less than clinicians and executives. And the promise of employment at health systems as a pathway out of poverty is not always borne out.
Some academic medical centers are promoting educational opportunities and new career pathways for their staff. In 2016, Rush University Medical Center launched an effort to create wealth-building opportunities for employees as part of its health equity strategy. Community health needs assessments, listening sessions, and an employee survey had revealed that many employees, particularly Black and Latina women, were struggling. In 2017, one of five employees living in Garfield Park, a low-income neighborhood near the hospital, experienced financial distress, including evictions, wage garnishments, and other problems. And their jobs — some in maintenance, food services, and security — weren’t leading to better things, says David Ansell, M.D., M.P.H., senior vice president for community health equity at Rush. “People came in poor and left poor 30 years later,” he says.
David Ansell, M.D., M.P.H., senior vice president for community health equity at Rush University Medical Center. Photo: John Boehm
In response, Rush raised entry-level wages to $15 an hour and opened 15 job application hubs, many in the low-income, predominantly Black, West Side neighborhoods that surround the academic medical center. Leaders also created pathways for advancement for incumbent employees interested in moving from unskilled to skilled positions, including fully funding training for staff interested in becoming certified as medical assistants. Rush has also promoted retirement savings by automating enrollment in 401k programs upon hire, a practice that from 2019 to 2021increased the percentage of employees saving for retirement from 68 percent to nearly 80 percent.
Much of Rush’s health equity strategy is aimed at closing the almost 20-year life expectancy gap between residents of the West Side and wealthier parts of the city. As part of this work, Rush helped found West Side United — a coalition of health care institutions, educators, faith-based organizations, and government agencies that works with area residents to promote economic and physical health, including by offering loans to small businesses and organizations addressing health-related community needs.
During the summer, staff from Rush University Medical Center join community residents in the “West Side Walk for Wellness.” The events are an opportunity to talk about health and wellness, as well as careers in the health professions. Photos: John Boehm
Rush also formed a 10-member employee resource group made up of staff who live on the West Side to learn about their experiences working at Rush and hear what supports they wanted from the health system. From the group and other employee surveys, Rush leaders learned that some employees felt invisible to white doctors who passed them by without saying hello.
Redia Holman, a patient navigator at Rush who grew up on the West Side, is a member of the employee resource group. She says she’s been pleased by the health system’s responses, which include holding town hall meetings for employees to air their concerns. She is also proud of Rush’s approach to community outreach during the pandemic but says there is much more to be done to address the health disparities laid bare by COVID-19 and those plainly visible in her work as a navigator. “When people ask me what I want, I say I want everyone on the West Side and every single, solitary human being to get those 20 extra years. It’s totally unfair that one group gets them and another doesn’t and I don’t think it’s unreasonable to hold health care systems accountable,” she says.
Redia Holman, a patient navigator at Rush University Medical Center. Photo: John Boehm
MetroHealth’s “Healing Begins with Listening”
As part of systemwide efforts to promote antiracism, MetroHealth, a public health system in Cleveland, Ohio’s Cuyahoga County, created a series of videos of employees describing racist experiences they’ve had in the workplace and elsewhere.
Reforming Medical Education and Recruiting More Medical Students of Color
To undo racist policies and practices in health care, academic medical centers are also trying to reform medical education. Along with race-based clinical algorithms, medical students are often taught about differences in disease prevalence among races without learning about their social or historical contexts, perpetuating the misconception of race as a biological construct. And as of 2017, only 40 percent of the nation’s medical schools had incorporated content on racial health disparities into their curricula.
Leaders in academic medicine are calling for dedicated, longitudinal training not just on health disparities but on the role of racism in health and how to combat it. They say training should be part of undergraduate and graduate medical education, as well as professional board certifications and continuing education. It should include didactic content as well as practical strategies for asking patients about their experiences in health care and being comfortable talking about racism.
Much of this work is being fueled by medical students themselves. At Boston University School of Medicine, students spent more than a year combing through syllabi, lecture slides, course documents, and exam questions to identify how racist assumptions have been baked into the curriculum and reviewing curricular reform efforts taking place at 12 other medical schools. Students then put out a 137-page report that proposes ways to incorporate learning opportunities about racism and health throughout medical school.
Boston University School of Medicine students participating in an event commemorating lives lost to racism. Photo courtesy of Boston Medical Center
Health system leaders have also called for greater efforts to increase the numbers of Black, Hispanic, American Indian, and other minority students in training programs for the health professions to ensure their representation at least matches the general U.S. population. In particular, the percentage of Black male physicians has not increased in 80 years. Among other efforts, leaders have called for tuition-free medical schools and less reliance on MCAT scores, following trends taking place in undergraduate college admissions. Critics have pointed to the long legacy of the 1910 Flexner Report, which demanded higher standards for medical schools but didn’t provide the resources to meet them. In its wake, five of the nation’s seven Black medical colleges closed and rising tuitions and other requirements made it harder for people without wealth and privilege to attend medical school. An American Medical Association study estimated that there are now 30,000 to 36,000 fewer Black physicians as a result.
Last June at the University of Pittsburgh, a group of Black medical students petitioned the new dean to make several changes to address racial inequities at the medical school, including recruiting Black students from the community. “Pittsburgh is around 23 percent African American, but it’s been a while since we actually recruited a Black trainee into the medical school from the community,” says Utibe Essien, M.D., M.P.H., assistant professor of medicine at the University of Pittsburgh and a core investigator at the Center for Health Equity Research and Promotion at the VA Pittsburgh Healthcare System. In addition to creating two full annual scholarships for Black medical students and two college scholarships for Pittsburgh high school students, the medical school formed a working group to explore how best to support Black members of its community. “After match day last year, many programs tweeted about having recruited ‘the most diverse class ever,’” Essien says. “But I don’t think it starts with those who have the resilience and grit to make it into medical school. It starts all the way back with our undergrads, with our high schools, and middle schools. And that’s why I think that community investment matters.”
At The Ohio State University (OSU) College of Medicine, where 25 percent of students come from underrepresented racial or ethnic groups, members of the medical school admissions committee are asked to take the race implicit association test (IAT). This test seeks to reveal people’s unconscious biases by asking them to quickly sort images of Black and white faces along with words that have either positive or negative associations; test takers who more quickly assign “good” words to white than Black faces are thought to have stronger implicit preferences for white people.
In 2013, the first year the IAT was offered, all 140 committee members at OSU completed the test, including 43 faculty members and 97 medical students (among whom were 21 people who identified as being from a minority group that is underrepresented in medicine). A study found that all groups (i.e., men, women, students, and faculty) had some level of unconscious bias in favor of whites, but the bias was strongest among men and faculty members and lowest among women and medical students. Citing other studies that have also found both Black physicians and nonphysicians tend to have little or no bias on the race IAT, the researchers suggested that to reduce racial bias in medical school admissions, committees should include more Black members as well as more women and medical students.
The medical school class that matriculated the first year after the IAT was given was the most racially diverse in Ohio State’s history. That was not because more candidates of color were accepted overall, but because more of those who were accepted chose to attend — perhaps because they felt greater connections with admissions committee members.
“What we think has happened is that when the interviewers become aware of their own implicit biases, they can check those at the door, and then it becomes more of a conversation in which they can learn how a candidate’s life experiences will prepare them for medical school,” says Leon McDougle, M.D., chief diversity officer at OSU Wexner Medical Center, associate dean for diversity and inclusion at the College of Medicine, and one of the study authors. “And we’re thinking that the person being interviewed is feeling welcomed into a conversation.”
Lessons
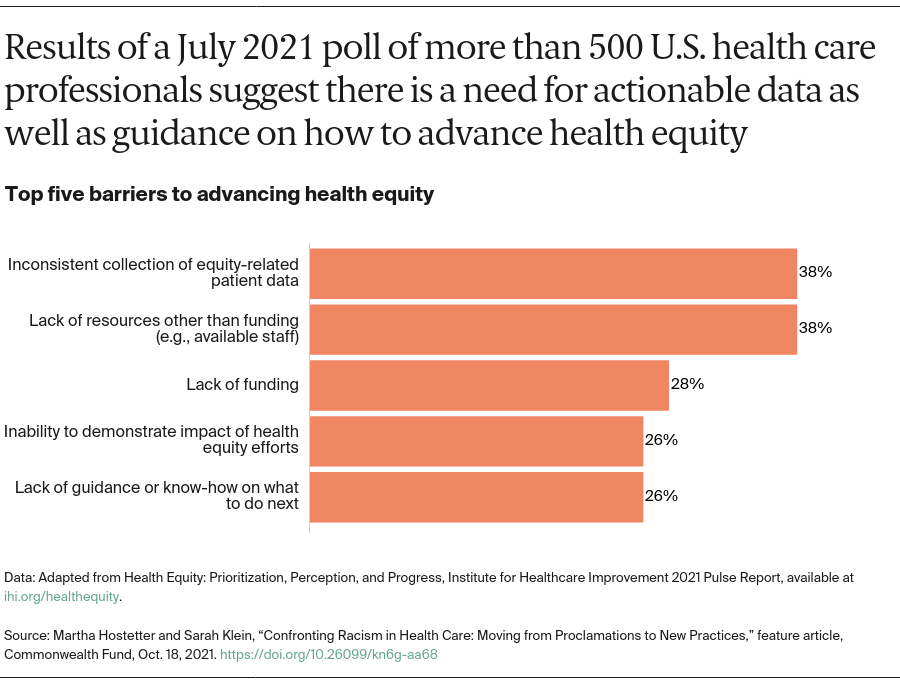
For now, academic medical centers working to promote racial equity have focused on issues over which they have direct control, including patients’ experiences of care, hiring and promotion practices, and community investments. Their early efforts may offer guideposts to others embarking on this work. According to a July 2021 poll conducted by the Institute for Healthcare Improvement among 500 U.S. health care professionals, health equity has emerged as a top priority for more than half of health care organizations (58%), up from one-quarter in 2019. But respondents said they face several barriers, including not having relevant, consistent data about their patients and not having dedicated staff or other resources to do this work.
In addition to gathering actionable data and dedicating resources to this work, academic medical leaders say it matters how racial equity initiatives are conducted. Most important, efforts to identify racist policies and practices must be coupled with commitments to change them. Otherwise, those who have borne the brunt of discrimination — as patients and professionals — will remain justifiably skeptical of proclamations to do better. “We’re tired of words,” says Battle of the University of Chicago Medicine. “Everybody’s tired of words.”
Leaders note that the weight of this work should not be borne on the shoulders of those who’ve experienced racism. “We know that we need to be antiracist and that racism is a public health issue, but how do we do this work other than asking an overwhelmed, busy, usually person of color to volunteer?” says Essien of the University of Pittsburgh. The University of Pittsburgh took the step of paying medical students for the time they’ve spent advocating for reforms. In addition to valuing the work, it’s important to involve health system staff from a wide range of departments and roles in antiracism activities.
Measuring and reporting progress toward institutional goals — recruiting more leaders of color, for example— can drive progress within organizations. But health systems also should be held accountable by health plans, accreditation agencies, and consumers for advancing health equity.
The Lown Institute has started to rank hospitals on measures of racial inclusivity — attributing higher scores to hospitals that serve a greater proportion of nonwhite Medicare beneficiaries than reside in their surrounding communities. Lown found the most and the least racially segregated hospitals are within blocks of one another. The Illinois Health and Hospital Association, meanwhile, is piloting the Racial Equity and Healthcare Progress Report to assess efforts by the state’s hospitals to promote racial equity. It’s modeled on an existing tool that assesses hospitals’efforts to welcome LGBTQ+ patients and raises expectations for performance each year.
And faculty from Johns Hopkins University’s Bloomberg American Health Initiative and the Center for Health Equity recently partnered with IBM Watson Health to develop new measures of hospitals’ contributions to community health, with a focus on racial equity. When the measures were incorporated into IBM Watson Health’s 100 Top Hospitals ranking rankings for 2021, 37 of the 100 hospitals moved into different positions.
Such accountability tools will be needed if we are to track whether the racial justice movement is measurably changing rich and powerful health care institutions. “As a scientist,” Penn Medicine’s Merchant says, “what’s interesting is thinking about how we measure if we made a difference and whether this was an actual inflection point.”
Publication Details
Date
Contact
Martha Hostetter, Consulting Writer and Editor, Pear Tree Communications
Martha Hostetter and Sarah Klein, “Confronting Racism in Health Care: Moving from Proclamations to New Practices,” feature article, Commonwealth Fund, Oct. 18, 2021. https://doi.org/10.26099/kn6g-aa68