Our Scorecard ranks every state’s health care system based on how well it provides high-quality, accessible, and equitable health care. Read the report to see health care rankings by state.
Community Health Centers Seek to Prepare Medicaid Beneficiaries, and Themselves, for the Risks Ahead
Tamika Reliford helps patients with insurance enrollment at Swope Health's central facility in Kansas City, Mo., in March 2023. Almost half of Swope's patients are covered by Medicaid or the Children's Health Insurance Program. Federally qualified health centers care for roughly one of six Medicaid beneficiaries and are expected to play a pivotal role in identifying people at risk of losing their coverage, helping them stay enrolled, or assisting them in finding other insurance. Photo: Arin Yoon via The New York Times
Tamika Reliford helps patients with insurance enrollment at Swope Health's central facility in Kansas City, Mo., in March 2023. Almost half of Swope's patients are covered by Medicaid or the Children's Health Insurance Program. Federally qualified health centers care for roughly one of six Medicaid beneficiaries and are expected to play a pivotal role in identifying people at risk of losing their coverage, helping them stay enrolled, or assisting them in finding other insurance. Photo: Arin Yoon via The New York Times
Toplines
With the suspension of continuous enrollment causing many Medicaid beneficiaries to lose their coverage, community health centers are working to help their patients stay insured
Federal pandemic relief funds and regulatory changes — like a loosening of restrictions around staff credentialling — have also enabled health centers to experiment with new care models and reach people struggling to access care
Toplines
With the suspension of continuous enrollment causing many Medicaid beneficiaries to lose their coverage, community health centers are working to help their patients stay insured
Federal pandemic relief funds and regulatory changes — like a loosening of restrictions around staff credentialling — have also enabled health centers to experiment with new care models and reach people struggling to access care
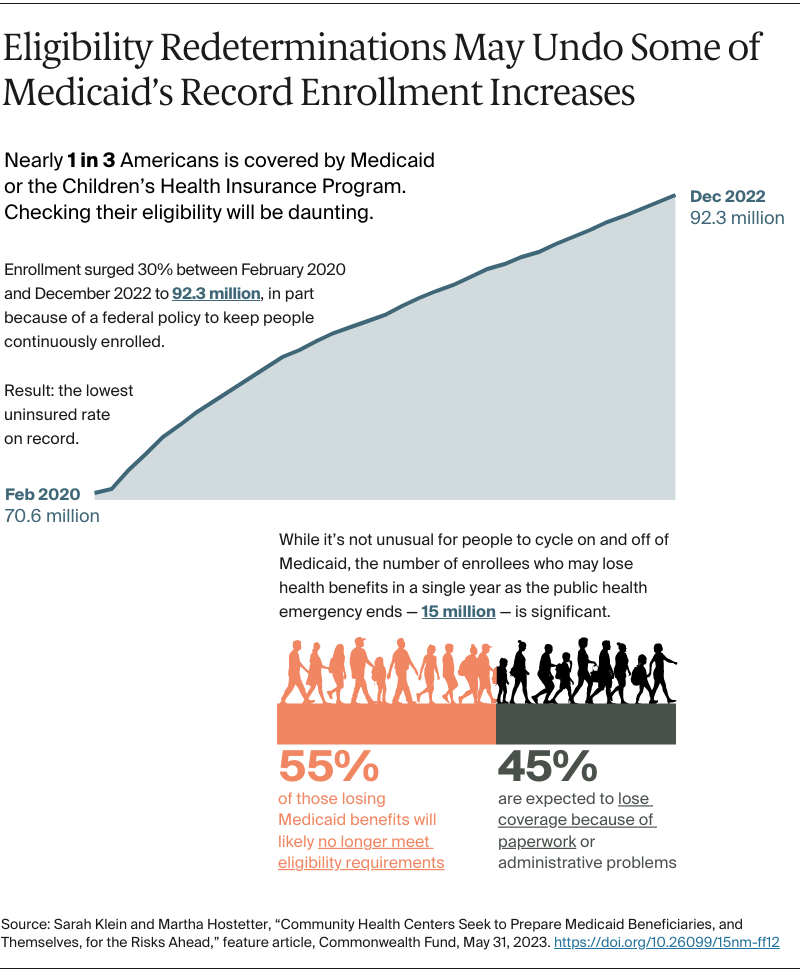
All 50 states have begun the monumental task of determining whether 92.3 million Americans are still eligible to receive Medicaid benefits based on their age, income, and disability status. These “redeterminations,” usually done annually, were suspended during the COVID-19 public health emergency to ensure that people at high risk of poor outcomes from the disease were able to stay continuously covered.
It's estimated that 15 million people will lose Medicaid benefits over the next 13 months as the redetermination process unfolds. Some will no longer meet their state’s eligibility requirements, while others are likely to be disenrolled because of administrative and paperwork errors. Among them will be people who miss notices of the redetermination process and, with that, miss deadlines for enrolling in a low-cost marketplace plan or for applying for coverage through an employer.
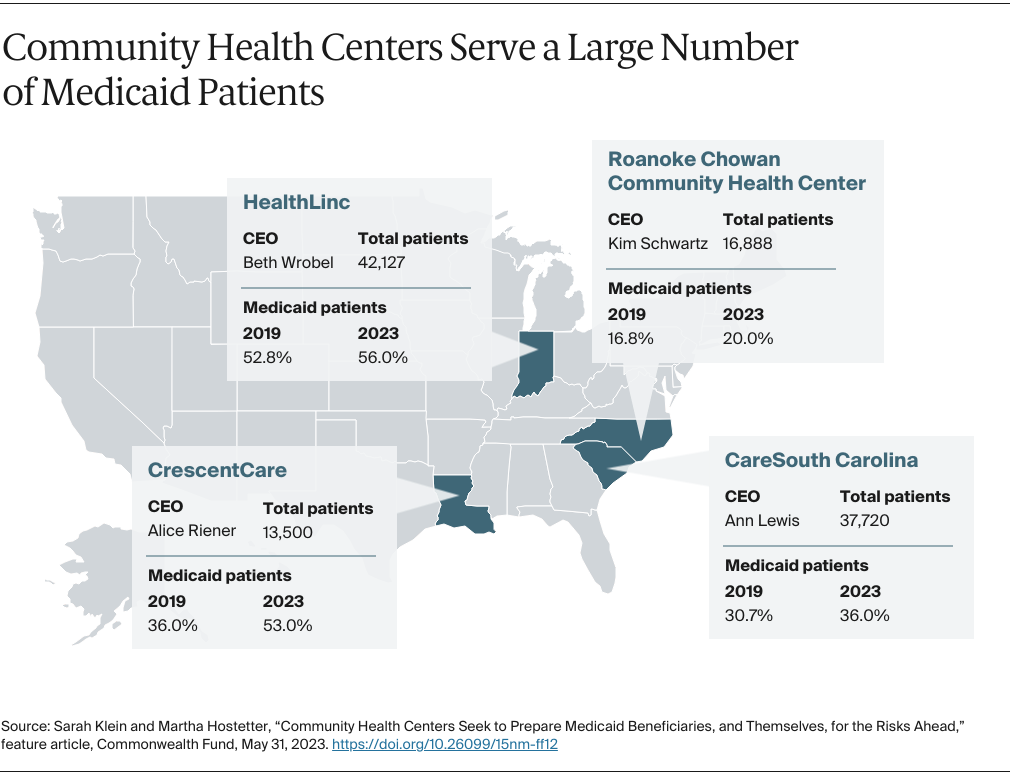
Federally qualified health centers (FQHCs), which care for roughly one of six Medicaid beneficiaries, are expected to play a pivotal role in identifying people at risk of losing their coverage, helping them stay enrolled, or assisting them in finding other insurance. To understand how FQHCs are approaching the challenge, we reached out to CEOs of four community health centers: two in states that, prior to the pandemic, expanded Medicaid eligibility to cover more adults with low incomes (Indiana and Louisiana) and two in states that didn’t expand Medicaid (South Carolina and North Carolina, the latter of which has since approved expansion but has not yet implemented it).
We also asked how their health center operations have been changed by an infusion of federal funds from the Coronavirus Aid, Relief, and Economic Security (CARES) Act as well as increased regulatory flexibility during the pandemic, including payment for audio-only telehealth visits and loosened restrictions around staff credentialling. We learned that the flexibilities and new funding spurred a number of innovations with the potential to improve patient care and lower its cost. But without policy changes at the federal and state levels, some of these will be hard to sustain.
Planning for Turbulence Ahead
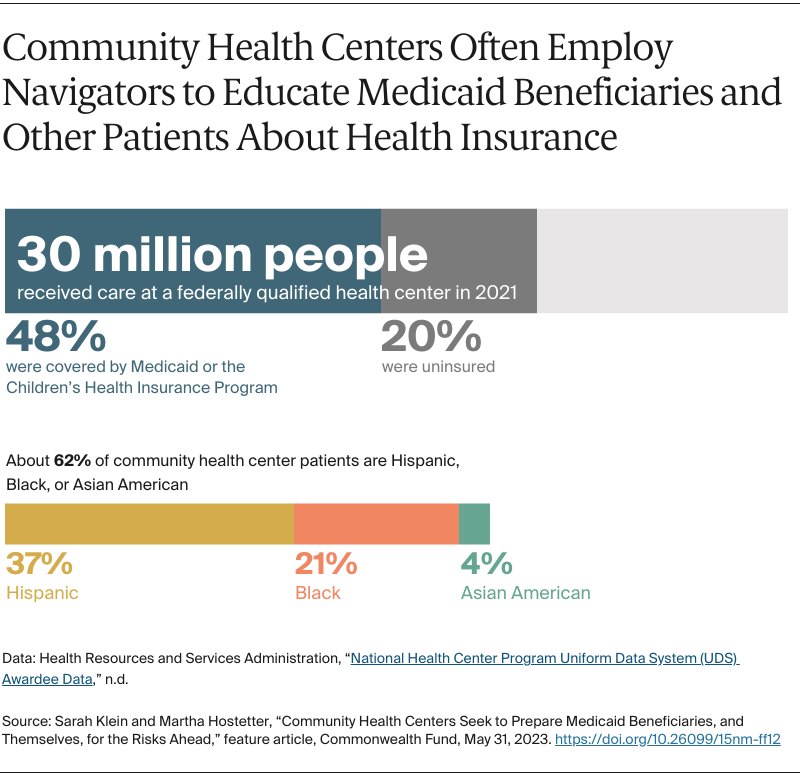
Medicaid covered nearly half of FQHC patients in 2021. The highest concentration was in states that expanded their programs to cover more adults with low incomes. As safety-net health care providers, FQHCs also treat 6.1 million people without insurance.
Beth Wrobel, CEO of HealthLinc
Each of the FQHC leaders we spoke with has launched campaigns and leveraged staff to notify patients of the risks they face. Clients are being encouraged to collect records proving they’re still eligible for benefits and/or to inform Medicaid agencies and managed care plans of address changes. Beth Wrobel, CEO of HealthLinc, an FQHC with 12 sites in northern Indiana serving more than 42,000 patients, says the state has warned that up to a quarter of the people now covered by Medicaid could be dropped from the program within a year.
The FQHC has already begun to see changes in enrollment. In January, the percentage of patients covered by Medicaid fell by 2 percent while the number covered by commercial insurance increased by the same amount, suggesting people who have access to employer-sponsored coverage made an early switch.
To reach other Medicaid-covered clients, HealthLinc has deployed 20 navigators and trained more than 500 staff members to answer questions about upcoming eligibility reviews, which Indiana will stagger over 12 months. The state also has asked the Medicaid managed care companies (MCOs) that provide health insurance coverage to notify their members and the members’ providers about the reviews. But Wrobel is concerned about the accuracy of forthcoming reports from MCOs on Medicaid enrollment: in the past, only 25 percent of the patients that the health plans attributed to her clinic were actual HealthLinc patients, she says.
Ann Lewis, CEO of CareSouth Carolina
CareSouth Carolina, which operates 14 clinics serving nearly 38,000 patients in South Carolina’s Pee Dee region, has also launched a campaign to notify patients of upcoming changes. In addition to warnings posted to its website and social media channels, the FQHC has created a script for front-desk staff to use when clients ask about Medicaid coverage. Staff can make referrals to the FQHC’s 30 community health workers, whom clinics are deploying to help people work through the review process. “It can be a heavy lift for each application because there’s so much uncertainty about the personal information the state has and may request,” says Ann Lewis, CareSouth Carolina’s CEO. One of her biggest fears is that the addresses in the state’s database are outdated. “This is a population of patients that moves around quite a bit,” she says. “Ultimately, people are going to fall through the cracks.”
Alice Riener, CEO of CrescentCare
Louisiana, which also will be staggering its reviews over the course of a year, has touted its ability to verify income information electronically. But Alice Riener, CEO of CrescentCare, an FQHC that treats 13,500 patients annually, remains concerned. She is particularly worried about patients with serious medical conditions who lack the bandwidth to navigate the process, as well as people without a stable address or phone number. Hurricane Ida displaced many individuals in 2021, and she suspects others moved after eviction moratoriums and pandemic-era housing supports were withdrawn.
CrescentCare has been sending texts to patients and has staff on hand to help with enrollment. It also provides office space, as well as partial reimbursement, for a Medicaid agency employee who serves as a liaison. Still, Riener expects they may not hear from some patients until they run out of medication or slip into crisis. “It’s kind of like watching a train coming down the tracks,” she says. “It will hurt the most vulnerable.”
The Pandemic’s Silver Linings
It remains to be seen whether the federal government’s continuous Medicaid coverage policy has improved enrollees’ health. A Commonwealth Fund survey found that adults with continuous Medicaid coverage reported significantly fewer cost-related access problems compared to people who experienced a coverage gap. Another study found continuous Medicaid coverage was associated with better access to preventive services and reduced unmet needs for specialty care for children.
Several FQHC leaders reported that, without patients having to cycle on and off Medicaid as their income levels fluctuate, measures of care quality and health outcomes have improved. HealthLinc, for example, saw measures of diabetes and hypertension control increase to 80 percent and76 percent, respectively, in 2022, up from 76 percent and 74 percent in 2019. And the health center’s retention rate — the percentage of patients who return from one year to the next — reached 81 percent in 2022, up from 68 percent in 2019. CareSouth Carolina, meanwhile, was able to increase the share of adolescent patients with well-child visits from 40 percent in 2019 to 78 percent in 2022, as telehealth use expanded and clinicians’ time was freed up from seeing fewer kids with viruses and colds.
During the public health emergency, many FQHCs also got a reprieve from the challenges of credentialling new providers. Anticipating a surge in demand for medical staff during the pandemic, several states simplified the process, facilitating the enrollment of out-of-state providers in managed care networks. Without these flexibilities, FQHCs and other providers serving Medicaid populations can wait months for managed care plans to add new hires to their networks, compelling clinics to pay for staff without any means of billing for their services — even retrospectively. Not only did the public health emergency put a stop to that practice, it enabled some of the FQHC leaders we spoke with to hire providers they might not otherwise have recruited.
Kim Schwartz, CEO of Roanoke Chowan Community Health Center
During the pandemic, Roanoke Chowan Community Health Center, which operates five clinics in the Inner Banks of North Carolina, a rural area that’s one of the poorest in the state, was able to hire physicians who were credentialled in other states to provide psychiatry services as well as primary care. Kim Schwartz, Roanoke Chowan’s CEO, says the family practice doctor she hired from Minnesota mostly worked remotely but also came on site to provide staff training on patient activation techniques.
“With an expedited process, it took weeks instead of months for us to get a qualified provider credentialled,” Schwartz says. “Now that we know this is possible and that the outcomes were outstanding, we really need to adopt some of these learnings and apply them, especially in the rural service areas that have faced challenges recruiting doctors and other licensed professionals.”
Telehealth Flexibilities Coupled with Federal Funding Spurred Innovation
The public health emergency also proved to be an opportunity to test new care models using funding and flexibilities the FQHCs would not otherwise have. Many of the pilots enabled health centers to reach patients who have difficulty accessing care. They also positioned health centers to succeed in value-based contracting arrangements that reward providers for lowering health care spending.
CareSouth Carolina used some of the $7 million it received through the American Rescue Plan Act and other grants to purchase five vans, which it staffed with teams of nurse practitioners, licensed practical nurses, and medical assistants. During the pandemic, the teams provided COVID-19 tests and vaccinations to remote areas and in community settings, including churches and worksites. The teams are now dispatched to deliver vaccines to families with multiple children and no reliable transportation or to visit elderly people whose mobility limitations make it difficult to attend annual wellness visits, for example. Because the vans are equipped for telehealth appointments, the FQHC can bill for those visits. “That’s an investment we could never have made on our own. It allows us to double down on value-based care,” CEO Ann Lewis says.
In Indiana, HealthLinc developed a community paramedicine program and a remote monitoring program that allow the FQHC to extend its reach. The community paramedicine program was launched as a pilot in June 2020 with a private emergency medical services (EMS) company that had idle paramedics. During the pandemic, the paramedics were dispatched to the homes of patients who were too frail or immunocompromised to come to the clinic. They performed a wide array of tasks, from delivering medical supplies, meals, and vaccinations to performing blood draws and helping people log on to telemedicine visits. “The paramedics were able to see things we would never know about in a clinic visit: an empty refrigerator or hazards that put a patient at risk,” says Melissa Mitchell, HealthLinc’s chief innovation and strategy officer. “Being able to glean that information was a really powerful thing.”
The initial pilot involved only 16 patients, but HealthLinc has since expanded the program to reach five to 10 patients per week with high-risk conditions who can’t come to the office. The paramedics rotate through five counties, visiting one per day, doing similar work: collecting blood samples, delivering medications, and helping set up telemedicine visits. Their salaries were initially covered by the Paycheck Protection Program; now HealthLinc pays the EMS agency $100 per visit, which enables the health center to break even on the calls that involve telemedicine visits with its providers.
HealthLinc’s remote monitoring program was also an outgrowth of the pandemic: it was initially designed to monitor patients recovering from COVID-19 after being discharged by local hospitals and emergency departments (EDs). With an $898,000 grant the FQHC received from the state’s health department, the program has been expanded to support patients with cancer and multiple chronic conditions. The grant covers the services of dieticians, community health workers, and community paramedics, who help patients identify emergent issues and manage their conditions.
Before the pandemic, Roanoke Chowan had a mobile clinic to serve farm workers and a remote monitoring program that focused on patients with diabetes and cardiovascular disease. Despite the latter producing savings — by preventing unnecessary ED visits and hospitalizations and by allowing for earlier hospital discharges — Schwartz says the FQHC struggled to get payment for those services from Medicare and Medicaid. “It took the pandemic to make that happen,” she says.
Sustaining the Gains
During the pandemic, extra funds and flexibilities enabled the four FQHCs to build programs that had been languishing on their wish lists and to demonstrate their capabilities. “The additional funding, from the rescue plan and other grants, was an unprecedented opportunity to realize dreams we had,” says CareSouth Carolina’s Lewis. Roanoke Chowan and CrescentCare both used extra funding to cover salaries and other operating expenses so they could free up funds to build services that are in high demand: dental care for Roanoke Chowan patients and behavioral health services for CrescentCare’s.
The funds also enabled FQHCs to be responsive to local governments that needed help reaching, vaccinating, and treating populations at risk for poor outcomes from COVID-19. CareSouth provided more than 12,000 monoclonal antibody infusions during the pandemic and HealthLinc dispatched staff to deliver vaccinations and COVID treatments in patients’ homes and community settings. “It proved the value of FQHCs,” says HealthLinc’s Wrobel.
With the end of the public health emergency, FQHC leaders are now concerned about the path ahead. Of the CEOs we spoke with, one said the financial impact of lower Medicaid enrollment would be negligible. But another CEO expected revenues to drop anywhere from 3 percent to 6 percent, and a third predicted a decline of as much as 10 percent, potentially leading to job cuts. There’s also uncertainty surrounding future grant funding for FQHC operations and mobile clinics. And, in some states, the extension of flexibilities around telehealth remains in doubt.
“The big takeaway for me is that you have to invest in public health infrastructure, and that has to be ongoing, sustainable funding that organizations can depend on,” said CrescentCare’s Riener. “It can’t be a grant here or there, but something we can count on to build resilient medical services that are desperately needed by the community.”
Wrobel is particularly worried about HealthLinc patients who refrain from seeking medical care out of cost concerns. Before Indiana expanded Medicaid, she encountered many people who avoided getting care when they were sick, including a woman with cancer who was terrified her family would lose their only asset, their home. By happenstance, the woman learned Indiana offered Medicaid coverage for patients with breast and cervical cancer. Although her cancer had progressed by then, she was able to obtain surgery that saved her life. “I always wondered what would have happened if she came in earlier and didn’t have to have surgery,” Wrobel says. “What are the cost implications of that?”
How to Avoid Care Disruptions for People with Medicaid
Policymakers have advanced several proposals for minimizing the risk that Medicaid beneficiaries will face gaps in coverage. Here are two of them:
Congress could give states the option of allowing adults to maintain Medicaid eligibility for a full year, regardless of changes in their income — something states have long had the ability to provide for children. Three states have already received a waiver from the Centers for Medicare and Medicaid Services to do just this.
States could strengthen “continuity of care” protections to ensure that Medicaid beneficiaries with serious and complex conditions who are undergoing treatment, including people who are terminally ill and those scheduled for nonelective surgery, continue to have access to medical care. Such protections are usually triggered only when a patient’s provider leaves a health plan network.
Publication Details
Date
Citation
Sarah Klein and Martha Hostetter, “Community Health Centers Seek to Prepare Medicaid Beneficiaries, and Themselves, for the Risks Ahead,” feature article, Commonwealth Fund, May 31, 2023. https://doi.org/10.26099/15nm-ff12