
Abstract
- Issue: Efforts to improve the integration of care delivery and financing systems for dual-eligible individuals enrolled in both Medicare and Medicaid typically do not address the unique health and social circumstances of those under age 65.
- Goal: To collect information directly from dual-eligible individuals under age 65 and their caregivers describing their particular needs and challenges to inform enrollment, access, and care management approaches.
- Methods: We held four focus groups of dual-eligible adults under age 65 and/or their caregivers in July 2024 via Zoom. Participants included individuals with physical and behavioral health conditions as well as those with intellectual and developmental disabilities.
- Key Findings: Focus group participants raised specific challenges, including: 1) fragile support networks and fear of losing parents’ assistance as they age; 2) poor coordination of medical, behavioral health, and social care; 3) scarcity of providers equipped to address their health and social needs; 4) limited access to services, equipment, and personal care support needed for employment and community integration; and 5) absence of trusted, knowledgeable, and reliable sources for navigating health plan enrollment choices, authorization rules, and provider networks.
- Conclusion: Policymakers need to recognize and address the specific needs of dually eligible individuals under age 65 as integration efforts proceed.
Introduction
Federal and state legislative and regulatory policymakers are pursuing a number of approaches for better integrating Medicare and Medicaid for Americans enrolled in both programs.1 These initiatives include monthly opportunities for dual-eligible beneficiaries to enroll in integrated managed care plans to receive better-coordinated, less-fragmented care.2 But such efforts typically do not acknowledge the heterogeneity and varied needs of dual-eligible beneficiaries, who can have an array of physical and behavioral health conditions, intellectual and developmental disabilities (IDD), and/or complex health and social needs.
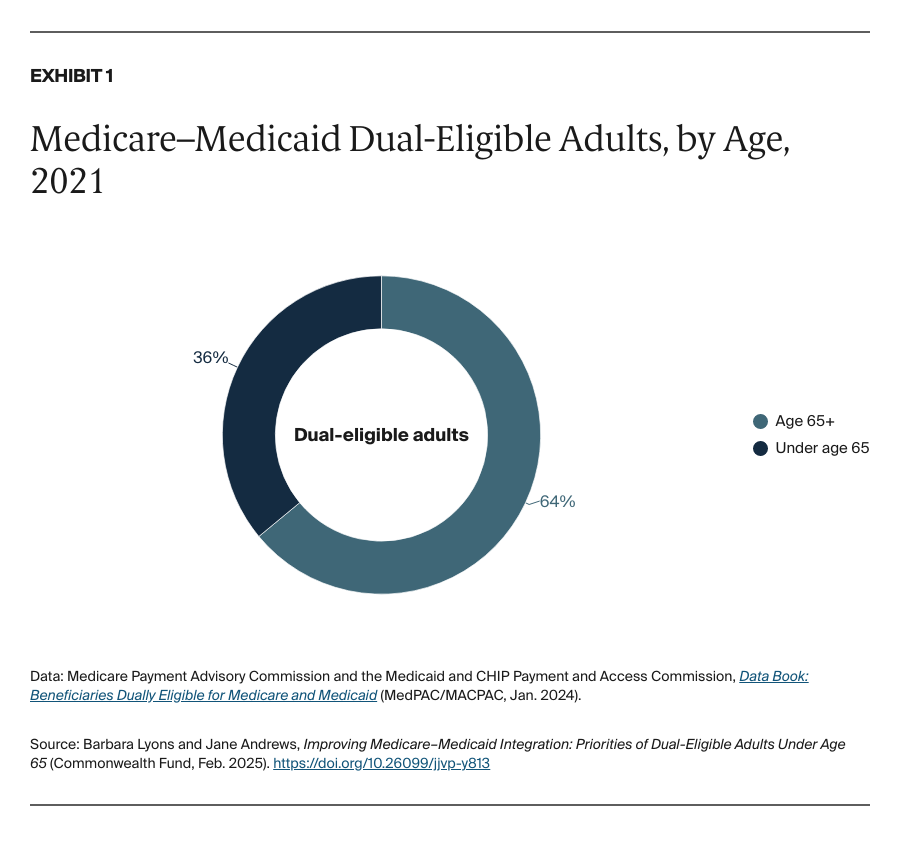
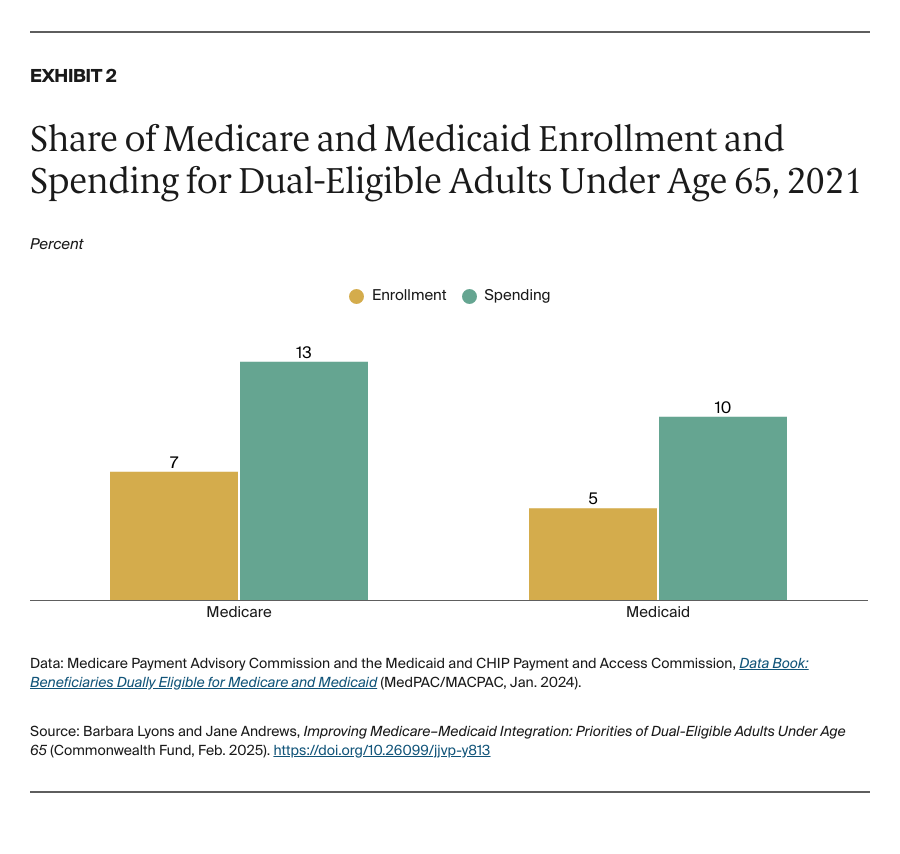
More than a third (36%) of the 12.8 million individuals dually eligible for Medicare and Medicaid are under age 65 (Exhibit 1). Behavioral health conditions such as anxiety and bipolar disorders, depression, and schizophrenia and other psychotic disorders are more common in the under-65 population, and they require intensive medical and nonmedical assistance to maintain independent living and avoid institutionalization.3 Unsurprisingly, this group accounts for a disproportionate share of health care spending (Exhibit 2).
Nonelderly dual-eligible individuals who have chronic disabilities and low incomes are eligible for benefits under both programs (see box below). These individuals often experience fragmented and uncoordinated care because financing and care delivery may come from different programs, leading to confusion about coverage, long wait times for services, and lack of access to providers who understand their special health and social needs. This disjointed system puts them at risk for poor health outcomes and can jeopardize their ability to remain in the community.
Integrated care aims to coordinate and combine Medicare and Medicaid services and payments; align administrative procedures such as beneficiary materials, appeals, and grievances; jointly oversee the programs; and improve access for dual-eligible individuals. While federal and state policymakers strive to bring down costs, reduce fragmented care delivery, and increase enrollment in Medicare managed care plans through Medicare and Medicaid integration testing,4 legislation,5 and regulation,6 they also should be seeking to address the unique health and social challenges facing dual-eligible beneficiaries under age 65.7 These individuals often struggle with access to specialists like behavioral health providers, worry about aging parent caregivers, and meeting social needs like utility and rent payments — all essential for employment and community living.
To explore people’s needs and experiences in navigating care, we conducted four focus groups via Zoom in July 2024. Participants included dual-eligible individuals under age 65 who have physical, behavioral health, and IDD, as well as their caregivers. (See “How We Conducted This Study” for additional details.)


