


Congress is currently proposing nationwide Medicaid work requirements. Previous studies of Medicaid work requirements have focused on coverage losses among working-age adults. In this blog post, we look at enrollees who are patients of community health centers (CHCs), the largest source of comprehensive primary health care for people with low incomes. CHCs serve their patients regardless of insurance status and thus are available for care even when coverage lapses or is unavailable. In 2023, CHCs served more than 31 million people; sometimes they are the only source of health care in a community. Since the first CHCs began operating 60 years ago, they have operated alongside Medicaid; together the two programs are fundamental to health care access for medically underserved communities. It is essential to consider how Medicaid policies generally — and in particular, work requirements — will affect CHCs’ ability to carry out their health care mission.
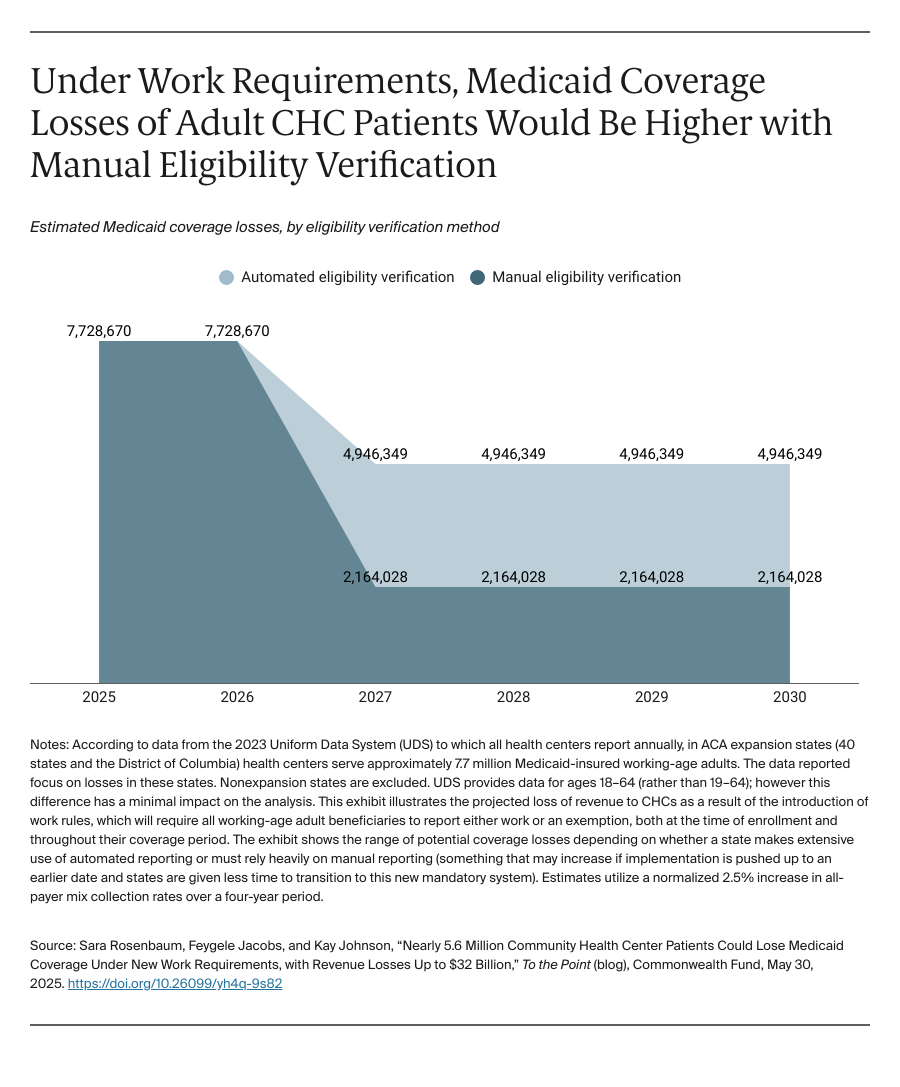
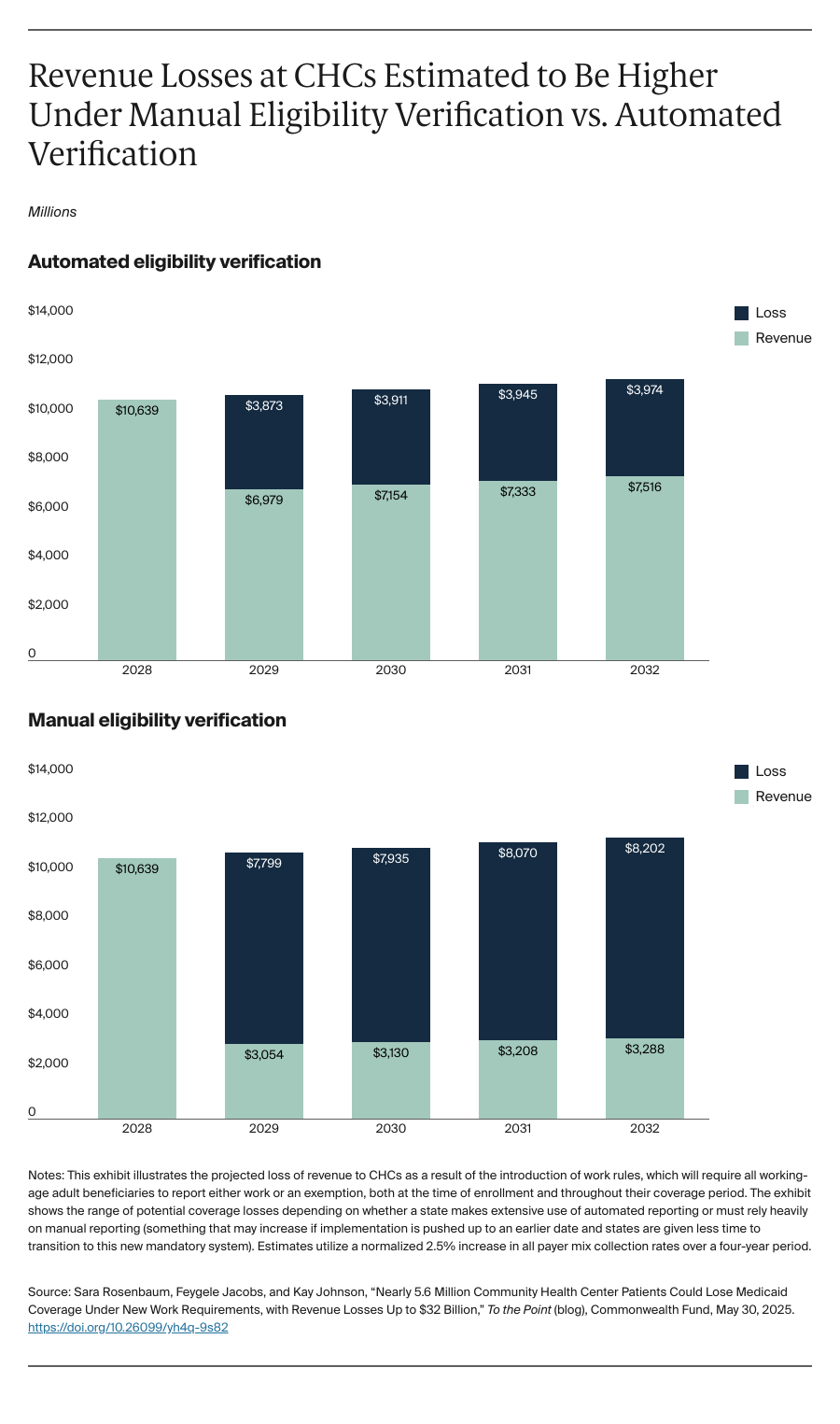
Over the five years following implementation of the Congressional reconciliation bill’s work requirements, we estimate that nearly 5.6 million CHC Medicaid patients who live in states that have expanded Medicaid to low-income working-age adults (i.e., 40 states and the District of Columbia, as of May 2025), could lose coverage; CHC revenue losses would be nearly $32 billion. Funding losses this steep would severely affect CHCs’ operational capacity and could lead to the outright closure of many, since, on average, Medicaid accounts for 43 percent of CHCs’ operating revenue.
CHCs are often the primary health care homes for Medicaid patients with the most complex medical and social needs. Adults who receive care at CHCs tend to be older, in poor health, and have considerable health and social burdens. More than 1.4 million are homeless. One-third are residents of rural communities, and nearly 1 million are seasonal agricultural workers, who face added health and social risks. More than 6 million are served in sites located in or near public housing. Overall, adult CHC patients are twice as likely to report being in fair-to-poor health, with elevated rates of chronic health conditions. Patients may struggle to work more than a few hours a week, and their wages, from jobs such as day labor, babysitting, or housekeeping, are less likely to be captured in automated wage information. These patients will be far less likely to benefit from automated systems for providing documentation of their work status or exemption. Instead, they will have to rely on frequent manual reporting.
The budget reconciliation bill, as passed in the U.S. House of Representatives on May 22, conditions Medicaid eligibility on work for adults whose coverage is based on the Affordable Care Act Medicaid expansion (i.e., for low-income adults 19 to 64). To enroll or maintain continuous enrollment in Medicaid, these adults must demonstrate either that they fulfill the work requirements or qualify for an exemption, such as caring for children or disabled family members or having a serious health condition. States must implement and enforce the requirement as a condition of federal funding and risk major federal funding losses if they erroneously cover nonqualified people. The bill encourages (but does not require) states to have automated reporting systems. This may be virtually impossible, at least in the near term, because the bill mandates nationwide implementation by December 31, 2026. For enrollees, the added burden of having to continuously report their status manually may result in high rates of coverage interruption, particularly for people with a heavy medical burden or social hardships, like a lack of transportation or stable housing. Yet states, fearing that erroneous coverage will expose them to substantial federal funding clawbacks, may choose to require reporting more frequently than the bill’s minimum six-month intervals (e.g., monthly).
The Urban Institute has estimated that although more than 90 percent of Medicaid-enrolled working-age adults currently either work or would be exempt, between 36 percent and 42 percent of people could lose coverage, largely because of reporting complexities. For populations dependent on manual reporting, the evidence shows that the risk of coverage loss grows to 72 percent. Although CHCs provide patients with Medicaid enrollment assistance, the sheer size of the patient population, along with significant funding declines, rising health care costs, and heavy patient care demands would likely hamper their ability to provide their patients with the extensive reporting assistance they need.
Using the Urban Institute estimates, we look at the potential coverage losses among CHC patients and the related financial consequences. CHCs would experience steep revenue declines and continue to treat patients without the attendant insurance revenue. Based on previous work, we estimate that 65 percent of CHC patients losing Medicaid will become uninsured, while the remainder may qualify for another form of insurance, whether job-based coverage or a subsidized marketplace plan. Some patients ultimately may return to Medicaid, but as Georgia’s experience shows, navigating the enrollment process is so challenging that enrollment among eligible people remains extremely low.