

Community health centers (CHCs) serve as a lifeline for millions seeking primary and behavioral health care. In 2023, 32.5 million patients relied on CHCs, many receiving mental health and substance use disorder (SUD) services that improve outcomes and reduce costs. Yet, emerging Medicaid policy proposals, including work requirements and more frequent redeterminations, risk destabilizing this vital infrastructure.
Behavioral health integration is a proven model that embeds mental health and SUD services with primary care. In 2023, CHCs reported more than 43.5 million visits for mental health and substance use disorders, reflecting a 54 percent increase since 2018. Integrated care teams within CHCs coordinate these services, which can reduce emergency visits, help patients manage their chronic conditions, and lower overall Medicaid spending. These benefits depend on uninterrupted Medicaid coverage and predictable funding.
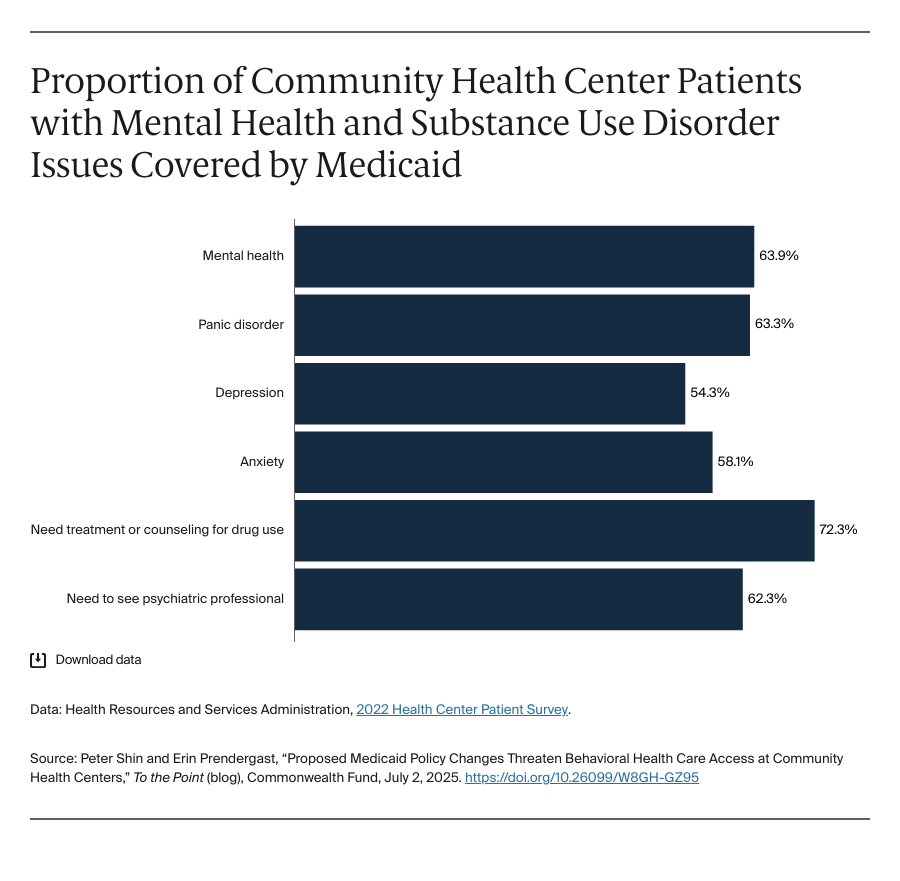
Work requirements pose a direct threat to patients who need care most. Among CHC patients with conditions like depression, anxiety, panic disorder, and bipolar disorder, the majority are covered by Medicaid. Behavioral health conditions can hinder individuals from maintaining a job or they could experience stigma due to a diagnosis or have a criminal record that could jeopardize employment. Tying coverage to work reporting ignores these realities and puts patients at risk of losing access to care when they need it most.
The Congressional Budget Office estimates that under the House bill (H.R. 1), at least 7.8 million Medicaid enrollees nationwide would lose coverage due to federal work requirements and more frequent eligibility verifications. For CHCs specifically, researchers estimate between 2.8 million and 5.6 million people are at risk of losing Medicaid coverage. Most of these losses would not result from ineligibility but from procedural red tape, reporting burdens, or technology failures. When Arkansas and Georgia introduced work requirements, many enrollees lost Medicaid coverage due to paperwork or administrative confusion.
During the Medicaid unwinding (i.e., the process in which states reviewed eligibility for millions of individuals who had remained continuously enrolled in Medicaid under pandemic-era protections), CHCs experienced similar trends. National data show that 69 percent of disenrollments occurred because of procedural reasons, not changes in eligibility. Many of the people affected had mental health and SUD issues. Such disruptions force patients to halt behavioral health treatment abruptly, worsening outcomes and increasing reliance on emergency care. One year after the Medicaid unwinding, community health centers reported significant staff reductions and service cuts.