The U.S. health system trails far behind a number of other high-income countries when it comes to affordability, administrative efficiency, equity, and health care outcomes, according to a new Commonwealth Fund study. Using surveys and other standardized data on quality and health care outcomes to measure and compare patient and physician experiences across a group of 11 high-income nations, the researchers rank the United States last overall in providing equitably accessible, affordable, high-quality health care.
The report, Mirror, Mirror 2021 — Reflecting Poorly: Health Care in the U.S. Compared to Other High-Income Countries, shows that getting good, essential health care in the U.S. depends on income — more so than in any other wealthy country. Since 2004, the U.S. has ranked last in every edition of the report, falling further behind on some indicators, despite spending the most on health care.
Half (50%) of lower-income U.S. adults reported that costs prevented them from getting needed health care, compared to a quarter (27%) of higher- income adults. In the United Kingdom, only 12 percent of people with lower incomes and 7 percent with higher incomes reported financial barriers to care.
Remarkably, a high-income person in the U.S. was more likely to report financial barriers than a low-income person in nearly all the other countries surveyed: Australia, Canada, France, Germany, the Netherlands, New Zealand, Norway, Sweden, Switzerland, and the U.K.
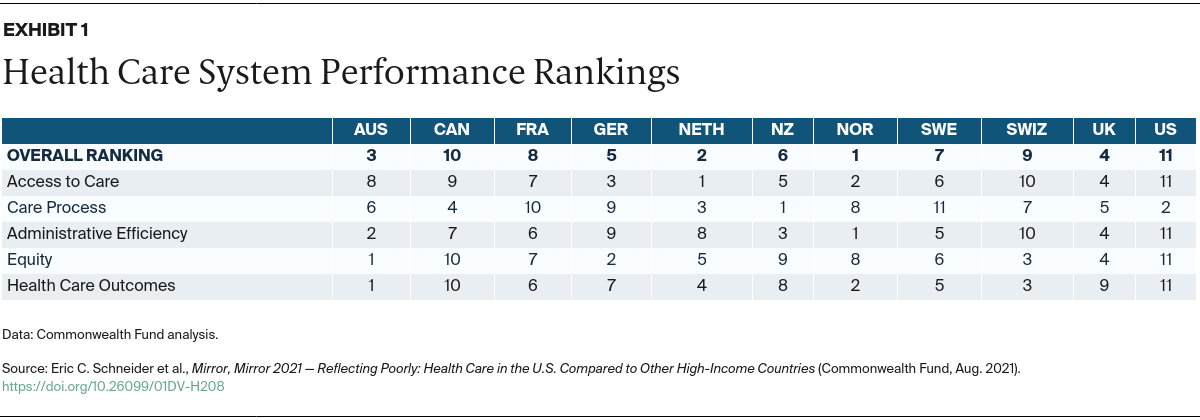
Norway, the Netherlands, and Australia were the top performers overall. In the middle of the pack were the U.K., Germany, New Zealand, Sweden, and France. Switzerland and Canada ranked lower than those countries, although both still performed much better than the U.S.
Among the 11 nations surveyed, the U.S. is the only one without universal health insurance coverage. Other research suggests that the U.S. spends less than other high-income countries on social services, such as child care, education, paid sick leave, and unemployment insurance, which could improve population health.
Additional report findings related to the U.S. include:
- Access to Care: Compared to people in other high-income countries, Americans of all incomes have the hardest time affording the health care they need. The U.S. ranks last on most measures of financial barriers to care, with 38 percent of adults reporting they did not receive recommended medical care in the past year because of cost. This is more than four times the rates for people in Norway (8%) and the Netherlands (9%). U.S. adults were also much more likely to report that their insurance denied payment of a claim or paid less than expected. Thirty-four percent of U.S. adults reported this, compared to 4 percent of adults in Germany and the U.K.
- Care Process: The U.S. ranks near the top, in second place, for care process, which combines four categories of indicators: preventive care, safe care, coordinated care, and patient engagement and preferences. Along with the U.K. and Sweden, on average the U.S. achieves higher performance on preventive care, which includes rates of mammography screening and influenza vaccination for older adults as well as the percentage of adults who talked with a health care provider about nutrition, smoking, and alcohol use. The U.S. also ranks high on safe care and patient engagement. However, not all American adults have equitable access to care and because the U.S. was ranked last in the other domains, including health care outcomes, it still ranks last overall.
- Health Care Outcomes: The U.S. ranks at the bottom on health care outcomes. Compared to other countries, the U.S. performs poorly on maternal mortality, infant mortality, life expectancy at age 60, and deaths that were potentially preventable with timely access to effective health care. The U.S. rate of preventable mortality (177 deaths per 100,000 population) was more than double that of the best-performing country, Switzerland (83 deaths per 100,000).
- Administrative Efficiency: The U.S. ranks last in administrative efficiency because of how much time providers and patients spend dealing with paperwork, duplicative medical testing, and insurance disputes. Nearly two-thirds (63%) of U.S. primary care doctors reported the time spent trying to get their patients needed treatment because of insurance coverage restrictions was a major problem. In Norway, which ranks first on this measure, only 7 percent of doctors reported this problem.

