Beyond the Survey: Engaging Patients and Communities as Partners
Toplines
True patient engagement goes beyond the satisfaction survey to enlist patients as partners in designing health care services.
Engaging patients in meaningful ways can help providers understand what it’s like to live day to day with a chronic conditions and what people need to stay healthy.
Toplines
True patient engagement goes beyond the satisfaction survey to enlist patients as partners in designing health care services.
Engaging patients in meaningful ways can help providers understand what it’s like to live day to day with a chronic conditions and what people need to stay healthy.
When it comes to learning from patients, many health care organizations just scratch the surface; they may field surveys to find ways to enhance satisfaction scores, like how to make hospitals more restful or reduce wait times, or they may solicit feedback on the design of new brochures or websites. It’s still rare for health care organizations to collaborate with patients in the design, development, and implementation of services even though doing so could improve health care and outcomes.
One downside of a more superficial approach to patient engagement is that health systems and plans miss opportunities to elicit information about people’s lives that could help them understand why they don’t come in for vaccines or cancer screenings; what it’s like to live day in, day out with a chronic condition; and what support people may need to stay healthy. Not only could such feedback inform providers’ strategies for reducing health disparities, but it also could help patients recognize the role they play in their own health.
In November 2020, the Commonwealth Fund’s Task Force on Payment and Delivery System Reform released its recommendations for improving quality, advancing equity, and increasing the affordability of health care in the U.S. The report includes more than 20 recommendations for engaging and empowering patients.
As an advocate, I’m often asked ‘How do we get people to engage more in our health care system?’ or ‘How do we get patients to…’ fill in the blank. I think we need to turn that question on its head. We should be asking patients, ‘How can we build a system that better meets your needs — one in which you want to engage?’
Debra Ness
President, National Partnership for Women and Families and Task Force member
This issue of Transforming Care looks at health care organizations and plans that are engaging patients in more meaningful ways: from learning from patients’ perspectives and involving them in efforts to improve quality and safety to partnering with them to identify and meet community needs. Their experiences offer lessons for others, the first of which is that none regretted the additional time spent with patients; to the contrary, they found it reinvigorated staff, led to creative solutions to problems, and elicited not just suggestions for improvement, but a groundswell of appreciation for the work providers were doing.
Viewing Health Care from Patients’ Perspectives
Colorado Medicaid Agency: Member Experience Advisory Council
In 2012, in anticipation of a massive expansion of Colorado’s Medicaid program, the state’s Department of Health Care Policy and Financing began mapping the process new enrollees would follow, looking for ways the system might break down or be confusing. By 2015, staff realized they needed to hear directly from enrollees about how well the program worked and gain feedback on their experiences with managed care plans and providers.
The agency created what is now a 20-member board that draws people from across the state for monthly meetings where they offer input on proposed policy changes, communication strategies, and barriers to accessing care. “We look for people who don’t have a lot of experience in health care but have an interest in improving things,” says Sarah Eaton, the agency’s deputy client officer. Before the pandemic, they met with agency staff in Denver (they now meet online); board members receive gift cards to compensate for their time and reimbursement for travel costs. Another 1,200 Medicaid members regularly respond to surveys about communication and enrollment approaches, among other topics.
One of the board’s first suggestions was to stop describing people as Medicaid beneficiaries or recipients. “They told us the term ‘member’ felt more inclusive, like they had a part in the program instead of feeling like something was being done to them,” Eaton says. Staff were also taken aback by how vulnerable many felt; just receiving correspondence from the agency in its distinctive yellow envelopes provoked fear of losing benefits, with some reporting they wouldn’t open an envelope on a Friday for fear of ruining their weekend. In response, agency staff added headlines to correspondence that is not related to eligibility and made other changes to make requests more straightforward.
As advisory board members began to trust agency staff, they confided other problems, including the fact that some practices were limiting access to Medicaid patients. After getting this kind of input, the state mandated that managed care plans establish their own member advisory committees. The plans also meet quarterly to share the feedback they are receiving.
Participating in the council has been empowering for members, Eaton says; some have joined state boards to provide input on other health care issuesand presented at national conferences alongside Eaton. After their terms end, often at the two-year mark, some have become so passionate about the work they volunteered to work as ambassadors, recruiting others to join.
St. Michael’s Patient Engagement Day
St. Michael’s Hospital Academic Family Health Team also found that viewing health care services from patients’ perspectives led to unexpected discoveries. The primary care team, which operates six clinics in downtown Toronto serving more than 49,000 patients, including young professionals, immigrants, people with HIV, and people experiencing homelessness, held a “Patient Engagement Day” in 2016. St. Michael’s used an approach advocated by the consultant Peter MacLeod, who advises health care and public-sector clients about ways to engage members of the public in policy discussions. Instead of holding events like town halls where people are forced to speak in front of crowds, which intimidates many and tends to invite only the shrillest voices, MacLeod suggests creating events where people, drawn by lottery, can spend time together learning about an issue, discussing shared problems, and brainstorming solutions.
Key to the approach is forming a representative group. St. Michael’s staff asked about 10,000 patients whether they’d be interested in spending a Saturday discussing ways to improve the typical primary care visit. Three hundred and fifty people volunteered, from which 36 were randomly selected to form a group roughly representative of St. Michael’s patient mix in terms of gender identity, housing, age, and self-reported health status; analysis also found they represented the patient mix in terms of ethnicity and immigration status.
To kick off the day, clinicians and other staff offered explanations about the health services the clinic offers and provided a behind-the-scenes look at a typical day. Next, patients identified pain points, from difficulty scheduling appointments to longer-than-expected waits, and then formed small groups to discuss potential solutions.
At the end of the day, patients submitted their recommendations, some of which the clinic has acted upon. For example, clinic staff are now more transparent about wait times (patients are informed at check-in about their place in the queue) and offer education about the role of medical residents. “We were surprised to learn that some patients became worried when residents left the room. They didn’t realize that the residents needed to review with their supervisor and that was pretty routine,” says Tara Kiran, M.D., a family physician and clinician scientist at St. Michael’s and the department of community and family medicine at the University of Toronto.
Kiran says the experience emboldened staff; the Family Health Team set up a Patient and Family Advisory Council and now requires medical residents to elicit patients’ input on quality improvement projects. “When we’re discussing operational changes, it’s likely that someone will now pipe up and say, ‘We need to understand what patients think about this,’” says Kiran.
Strategies to Engage Patients, from More Passive to More Active
The referenced media source is missing and needs to be re-embedded.
Anjana Sharma, M.D.
Anjana Sharma, M.D., assistant professor of family and community medicine at the University of California, San Francisco, School of Medicine, and colleagues have been tracking patient engagement activities in a variety of primary care settings. When they surveyed family medicine physicians across the U.S. in 2016, they found 31 percent worked in clinics that had two-way engagement with patients, such as having a patient advisory council (23.8%) or involving patients in quality improvement activities (20.5%). More consultative activities, such as surveys (76.5%) and suggestion boxes (52.9%), were far more common. The researchers found that larger practices, those certified as patient-centered medical homes, or those serving a higher proportion of vulnerable populations (as defined by the practices themselves) were more likely to report higher-intensity patient engagement activities than others (58.5% vs. 22.1%). Since the survey was conducted, Sharma has received an increasing number of inquiries about how to develop patient or community advisory groups, particularly during the last six months.
The pandemic and the racial reckoning of 2020 have been an inflection point — with more health care clinicians and leaders calling for robust patient and community engagement. Clinicians may think they have the answers, but often they don’t. We won’t be able to improve health care without partnering with patients and community members.
Anjana Sharma, M.D.
Assistant professor of family and community medicine at the University of California, San Francisco, School of Medicine
The PurpLE Clinic
In 2015, family medicine physician Anita Ravi, M.D., M.P.H., M.S.H.P., founded a clinic for people — mostly women — who have been trafficked for sex or labor or have experienced other traumatic events, including domestic abuse and rape. Roughly 90 percent of patients of the PurpLE Clinic (short for Purpose: Listen and Engage), then located within New York City’s Institute for Family Health, a federally qualified health center (FQHC), were referred by social service agencies. Even with a warm handoff, many were reluctant to visit the clinic or trust its providers, and many were still in abusive or trafficking situations and unable to focus on their health.
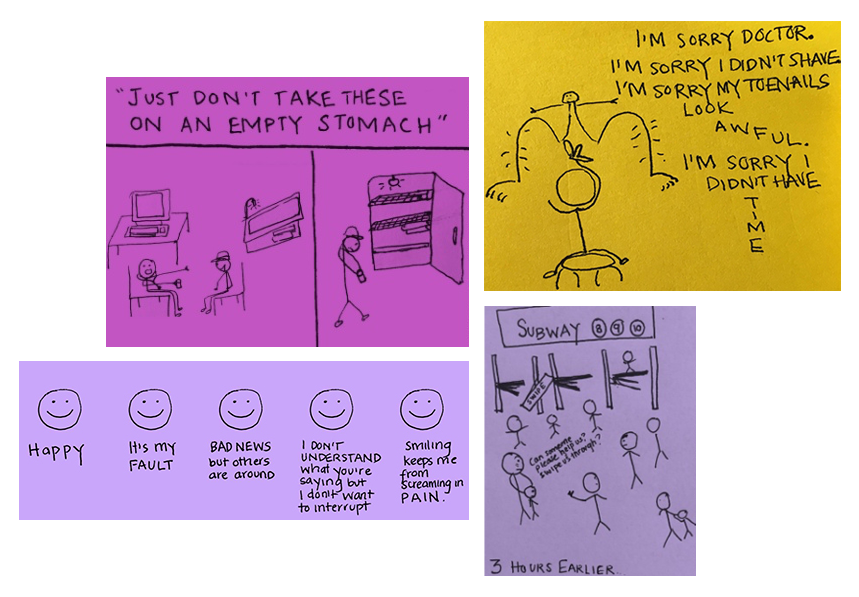
Ravi began making cartoon drawings to help other clinicians understand why patients — some of whom were living in the subway or storage units — were no-shows to appointments (e.g., they lacked subway fare) or couldn’t follow medical advice, like taking medication with food if they couldn’t afford to eat. She also wanted to help them respond appropriately to what seemed like incongruous behaviors, for instance when patients smiled as they described horrifying situations or apologized for their appearance during pelvic exams. “You don’t get taught in medical school how to effectively respond to moments when patients communicate shame,” Ravi says.
A study of PurpLE Clinic patients showed that women who’ve experienced sex trafficking or other forms of gender-based violence have levels of post-traumatic stress disorder at rates similar to those among U.S. combat veterans. Source: Anita Ravi, M.D., M.P.H., M.S.H.P.
Based on feedback from patients gleaned from one-on-one interactions, Ravi began making modifications: offering longer appointments than the typical 20-minute primary care visit to accommodate individual survivors’ needs, emphasizing that all care is confidential, and using pictures rather than words in flyers for patients who couldn’t read. PurpLE Clinic also hired a care navigator, Keisha Walcott, a former patient and trauma survivor herself, who became a key part of the clinic’s care model.
Walcott recognized the fears many patients had about trusting providers and served as a bridge, occasionally making home visits to find out why someone hadn’t returned for a follow-up visit or holding someone’s hand during a medical procedure. She also reinforced the importance of offering subway passes and menstrual products to patients to make it possible for them to come to the clinic — and of eliciting their priorities before proceeding. “In medicine, there’s such an emphasis on medication, but things like trying to find a place to live can be more important,” Walcott says.
After the pilot of the PurpLE Clinic ended in 2019, Ravi launched the PurpLE Health Foundation (PHF), a nonprofit that invests in integrated physical, mental, and financial health for survivors of gender-based violence and their families. It also helps educate providers about best practices for serving this population. In May, Ravi and her colleagues, including Walcott, plan to open PurpLE Family Health, a PHF-supported medical practice in New York City that will provide survivors with integrated physical and mental health care, as well as services to help them regain their financial footing. “We will be piloting emergency employment programs and working with survivors to develop financial health initiatives that prevent the cycle of exploitation,” Ravi says. PHF was awarded $1 million in funding support from the NoVO Foundation to launch this model of integrated care.
“I Suspect Sepsis” Campaign
MedStar Health’s public education campaign encourages patients who suspect they have sepsis to speak up. To spread the message, the health system has played the What You Need to Know About Sepsis video in waiting rooms of ambulatory care practices and has advertised it on MedStar Health’s buses.
In some cases, health care providers are forced to engage with patients when something goes wrong. Armando Nahum, an entrepreneur from Atlanta, began asking questions after three members of his family were diagnosed with life-threatening, health care–acquired infections in the space of 10 months. His father recovered, his wife is still living with complications, and his adult son died after developing sepsis from an infection, just as it seemed he would recover from a skydiving accident.
For Nahum, these incidents brought the deficits of the health system into sharp relief, including lack of transparency (the hospital where his son was treated did not disclose he’d twice contracted MRSA and listed the cause of death as complications of a skydiving accident rather than complications of a drug-resistant infection) and the burden placed on families to act as intermediaries and coordinate care, often without sufficient information. Wanting to do something in his son’s honor, Nahum and his wife, Victoria, founded the Safe Care Campaign to educate other families about the risks of infections and empower them to ask their providers about their infection-control practices.
In 2011, Nahum was invited to take part in Partnership for Patients, an initiative led by the Center for Medicare and Medicaid Innovation that since 2010 has involved nearly all U.S. hospitals in efforts to reduce adverse drug events, infections, and other health care–acquired conditions. In 2014, Nahum and his wife together with two patient safety advocates, Marty Hatlie, J.D., and Tim McDonald, M.D., J.D., launched the Healthcare and Patient Partnership Institute to offer hospitals technical assistance and advice on how to effectively partner with patients, starting with the creation of robust patient and family advisory councils focused on quality and safety.
In one such partnership in 2014, Nahum worked with clinicians at MedStar Health, which runs 10 hospitals in Washington, D.C., and Maryland, to promote early identification and treatment of sepsis. Every year, some 1.7 million Americans develop sepsis, an overactive and toxic response to an infection, and 270,000 die; timely treatment is key to recovery.
Nahum attended monthly meetings with clinical leaders, reviewing data on health care processes and outcomes. In one, Nahum questioned why ED patients sometimes wait hours to be screened for sepsis. He recommended changing the triage process to include an initial sepsis screening question, which generated concern from some clinicians that it would make the triage process too long. “I looked at them and said, ‘Really? Then tell me how much my son is worth,’” Nahum says. Today, every MedStar ED screens for sepsis during the triage process.
Nahum also helped break a logjam among MedStar clinicians who were debating how to use lab values and vital signs to make a sepsis diagnosis. “There’s no gold standard for doing so,” says Meena Seshamani, M.D., Ph.D., vice president for clinical care transformation at MedStar. “Armando’s voice created a sense of urgency and encouraged the group to try making a change and evaluating its impact to make headway toward saving lives.”
Today, MedStar has patient and family advisory councils focused on quality and safety at all 10 of its hospitals, modeled on the approach that Nahum recommends: including patients who represent the community the hospital serves in terms of race, ethnicity, gender identity, and socioeconomic status; including equal numbers of patients and staff, so patients won’t be intimidated; and creating a mechanism for reporting patients’ recommendations to hospital boards, for example by having a board member sit in on council meetings. To recruit patients, Nahum advises hospitals to go through their grievance databases. “I guarantee you that they will come and serve in your council,” he says. “Families want to help if you give them a chance.”
Nahum’s organization encourages hospitals to partner with patients on two types of projects: their own quality improvement activities and ones suggested by community council members. Across the country, the more than 300 quality and safety–focused patient and family councils have been involved in a wide range of activities, including: holding simulation exercises to help clinicians understand patients’ perspectives, participating in root cause analyses of adverse safety events, offering clinicians advice for broaching difficult conversations with patients, and designing programs to engage patients when there are clinical huddles or bedside shift changes.
An analysis of programs at 266 hospitals published by Vizient, a network that includes nonprofit hospitals and academic medical centers, found that those that had deeper levels of engagement with patients and families on issues related to quality and safety — assessed through qualitative interviews with patients and staff as well as quantitative measures of safety practices and ways in which patients were involved — had lower rates of unplanned hospital readmissions and fewer patient falls leading to injuries.
Engaging Patients in Their Health and Communities
Asian Health Services
As a condition of their funding, FQHCs must have patients comprise the majority (51%) of their governing boards; qualitative research has found most FQHC boards focus on finances and staffing and that patients tend to be recruited for their professional skills. Some FQHCs have also established patient advisory councils, which tend to get more involved in shaping services and may be more representative of their communities than governing boards.
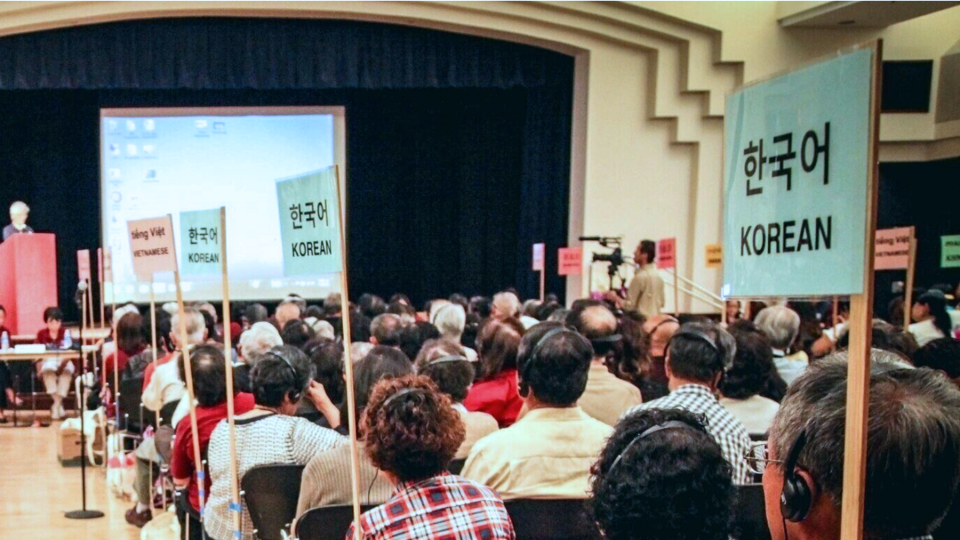
Asian Health Services, an FQHC in the San Francisco Bay Area, serves 50,000 patients, many of whom immigrated from other countries. To understand their distinct needs and encourage engagement, leaders established seven Patient Leadership Councils, representing patients whose first language is Cantonese, Khmer, Korean, Mandarin, Tagalog, or Vietnamese. Council members receive training in health topics such as diabetes, mental health, and the importance of having health insurance, and are then encouraged to educate their broader communities as community ambassadors.
Every one to two years, Asian Health Services holds general patient assemblies to elicit ideas and hear feedback. They offer simultaneous translation in 12 Asian languages. The events have drawn as many as 500 patients as well as local, state, and federal government leaders.
Asian Health Services staff have also partnered with patients to create healthier neighborhoods and workplaces. “Part of our work has been teaching our patients to assert their voices in their own languages. In this way, they can feel empowered to shape policies that affect them,” says Julia Liou, M.P.H., chief deputy of administration and development.
In 2004, one of the health center’s community health workers reported that nearly 100 Vietnamese nail salon workers were reporting health issues like dermatitis and respiratory problems. At the same time, many Vietnamese patients who were part of the salon workforce were asking their clinicians whether it was safe to work in nail salons. Asian Health Services staff found independent federal oversight over nail salon products lacking. After reaching out to other community-based groups in the region and bringing patients and other nail salon workers in other cities together, they realized the scope of the problem was far wider. “Everyone was experiencing the same health issues. We realized that this was an overlooked epidemic,” Liou says.
In 2005, Asian Health Services helped cofound the California Healthy Nail Salon Collaborative. The group, which now includes 20 statewide organizations and professional staff, offers training to patients and other salon workers about workplace health and safety, and builds their capacity to advocate for policy changes, in part by testifying about the effects of toxic chemicals on their health. Initially, it was difficult to convince women to come forward because they worried about jeopardizing their livelihoods. “They said, ‘If we tell our story, who will want to come to our salon to get their nails done?’” says Liou. “‘This is my livelihood.’” Eventually, some patients and workforce members agreed to testify before the federal and state lawmakers, helping gain support for the 2016 passage of the state’s Healthy Nail Salon Recognition Program Act, which incentivizes salons to reduce the use of toxic ingredients, install ventilation systems, and take other health and safety measures.
More recently, Asian Health Services staff have responded to increasing racist attacks on Asians throughout the nation and in the Bay Area amid political and public rhetoric blaming Asians for the pandemic. “Our patients and staff have experienced attacks and assaults, often within close vicinity of our clinic,” Liou says. The health center established a victim’s support fund and has been providing escorts for staff coming and going from clinic sites. Asian Health Services is also developing culturally tailored therapy and support for victims. “As a trusted community health provider, it has been in our DNA to respond to the needs of not only our patients, but our community as a whole,” Liou says.
Stephen and Sandra Sheller 11th Street Family Health Services
Many FQHCs are rooted in communities that lacked primary care services. Asian Health Services grew out of a one-room clinic that opened in San Francisco’s Chinatown in 1974; Stephen and Sandra Sheller 11th Street Family Health Service (11th Street) opened in 1998 in response to public housing residents’ demands for more accessible care in their North Philadelphia neighborhood.
For this reason, and because the payment model for FHQCs supports larger staffs and more comprehensive services than most primary care practices, the health centers are often able to mount vigorous responses to community-identified needs. Before opening a clinic, 11thStreet’s founders partnered with food banks to create an emergency food pantry. It and other health centers can then build on community members’ trust to engage them in their health and care.
The health center, which operates in partnership with Family Practice and Counseling Network and now serves 6,000 patients, has had a Community Advisory Committee since its inception. Its members (there are now 15) have shaped services and built relationships with local churches, public housing councils, schools, and nonprofits.
After a 2009–10 survey revealed high rates of trauma among patients linked to exposure to gun violence, discrimination, and adverse childhood experiences including having been placed in foster care, Community Advisory Committee members helped launch a campaign to let people know healing from trauma is possible and encourage them to seek help. 11th Street had already added a wide array of services — from mindfulness classes to yoga and creative arts therapies — in response to feedback from the community that they wanted the health center to focus on wellness, not just treat sickness. Leaders say these classes have helped patients cope with mental health problems and build resiliency; many are more willing to try them than traditional therapy.
Jacqui Williams and Diane Monroe sit on 11th Street Family Health Services’ Community Advisory Committee; members helped develop a campaign to encourage people affected by trauma to seek help. During the pandemic, the health center has been distributing bags with cleaning supplies, hand sanitizer, masks, and information about how to stay safe. Source: Stephen and Sandra Sheller 11th Street Family Health Services
During the pandemic, 11th Street has been responding to patients’ health and social needs while trying to keep them safe from COVID-19. Since April 2020, they’ve run a walk-up and drive-up coronavirus testing clinic for anyone, whether or not they have COVID symptoms or a prescription from a physician. Many testing sites only offer curbside testing, which leaves out people who don’t own cars, and during the early months of the pandemic most were only testing those with COVID-19 symptoms. But the health center’s leaders realized that many members of their community were at particular risk of contracting the coronavirus because they live in crowded homes and work where social distancing is not possible, and they wanted to make testing as easy as possible.
Starting this March, 11th Street began offering walk-up vaccination clinics to any Philadelphia resident who meets the city’s eligibility criteria, in addition to proactively reaching out to schedule appointments for older patients and others at high risk. Beforehand, leaders held a Zoom meeting to offer information about the vaccines and answer staff and community members’ questions. One staff member asked about the best way to convince patients who may be hesitant to get vaccinated. “I tell them that’s not the focus,” says Diana Hartley-Kim, M.S.W.,11th Street’s operations director. “As one of our panelists noted, you need to let go of the desire to get somebody get vaccinated and instead hear their concerns and just share some education. We need to recognize it’s their choice.”
LESSONS
As these examples illustrate, involving patients in efforts to increase the safety, effectiveness, and experience of health care draws attention to problems that can deter people from seeking help and points the way toward potential solutions. Successful efforts have emphasized building trust by forging long-term relationships and educating patients on policies that affect them. Many also stressed the importance of two-way communication (e.g., responding to patients’ feedback, not just asking for it) and attending to problems that patients themselves prioritize, even if the issues lie outside the four walls of their organization. One systematic review found that the benefits of patient engagement accrue not just to patients but to institutions in the form of greater staff satisfaction and improvements in safety.
It’s not incidental that many of the clinics we feature serve marginalized patients, including those with low incomes, immigrants, and survivors of trauma. To engage patients, their leaders have had to create deliberate processes to make care as accessible as possible and acknowledge the root causes of fear and mistrust, including past instances of discrimination. While these clinics aren’t typical, their experiences offer lessons for other providers who hope to build more effective partnerships with patients.
Spreading these practices to other institutions may require training for both patients and providers, as well as evidence of the types of leadership and culture that best support collaboration. Having frank conversations about what’s not working isn’t always comfortable. “Providers must make themselves vulnerable and transparent to patient and family representatives to truly engage them in improvement efforts,” says Seshamani of MedStar. Patients may also need encouragement to challenge prevailing practices. “Having community representatives outflanked by staff doesn’t work and can lead to them being marginalized,” says Debra Ness, president of National Partnership for Women and Families, an advocacy group.
Providers may also need financial or other incentives to partner with patients. Some value-based payment models, including some Medicare and Medicaid accountable care organization contracts, require providers to demonstrate they have consulted with patients and are meeting their expectations. Although there isn’t a one-size-fits-all model of patient engagement, best-practice standards could provide guidance about ensuring equitable recruitment, setting clear expectations, and providing accountability. “It matters who is at the table, how the conversations occur, and what expectations are set,” says Anjana Sharma, M.D., assistant professor of family and community medicine at the University of California, San Francisco, School of Medicine.
Patients, too, may need to be compensated for their time. In 2020, PHF created the Lived Experience Advisory and Research Network, or LEARN, to pay survivors of gender-based violence for their expertise and time helping design health care services and engagement strategies for people who face a variety of financial, cultural, and logistical barriers in accessing care.
Ultimately, tracking engagement — from which patients are filling prescriptions and getting screenings to more complex patient-reported outcomes measures — will be essential for building the evidence base of what works. Technologies that enable patients to monitor their conditions day to day and easily share that information with providers also may help. “The very fact that there is no standard set of patient engagement measures is, I think, very revealing,” says Vivian Lee, M.D., president of health platforms at Verily Life Sciences, a digital health company owned by Alphabet. “Oftentimes, we think about health as something that we as providers manufacture or produce. And that’s sometimes true in a hospital operating room or in an emergency room or in an ICU,” says Lee. “But we know that the vast majority of health is really determined by the behaviors of individuals and the degree to which health systems can support those individuals in enabling and producing their own health. And so engagement is absolutely essential to that.”
Q&A: Lessons from YouTube’s Leading Doctor About Engaging People in Their Health
The referenced media source is missing and needs to be re-embedded.
Garth Graham, M.D., M.P.H
In January, YouTube announced it would be collaborating with physicians and several health care organizations including the American Public Health Association, the Cleveland Clinic, and Mayo Clinic to create high-quality health content for the platform, which reaches 2 billion people monthly. Transforming Care spoke to Garth Graham, M.D., M.P.H., a cardiologist who previously served as U.S. Deputy Assistant Secretary of Health in the Bush and Obama administrations, about the effort. Graham now serves as director and global head of health care and public health partnerships at YouTube.
Transforming Care: When it comes to making medical information accessible, there seems to be a large divide between material that is either really simplified or very arcane and accessible only to experts. What’s your vision for how health information should be communicated?
Graham: The way we communicate information to patients, to communities, and even among ourselves as clinicians has lagged behind technology. Long gone are the days of posters and fliers. People get things on their phone and have come to expect information that’s relevant to be delivered instantaneously. COVID-19 has shown us we need to be transparent and communicate to the public in ways that people are going to understand and in the places they already are. YouTube is a platform that’s very present in people’s lives. People turn to it for information on all kinds of things, from yoga, meditation, and health to how to do things around the house.
Transforming Care: Is there something particular about video that makes it an advantageous way to communicate information?
Graham: Video allows you to take complicated information and make it digestible. For instance, it's very hard to explain messenger RNA in just a short brief. And again, a year ago, who would have thought people wanted to know what messenger RNA was? Video helps us break down complex information with visualization and makes it more engaging, digestible, and understandable. We can help people understand when it comes to social distancing, why six feet and not two feet? People want to know the evidence.
Transforming Care: YouTube has partnered with popular YouTube contributors to create health content. How do you go about picking which creators you partner with?
Graham:What we try to do is look for ways to make relevant, scientific information engaging with the help of creators who can engage people and encourage them to care about facts — for instance by bringing the rapper Fat Joe and Dr. Fauci together. Fat Joe has a large audience, with 1.37 million subscribers, and he was able to ask Dr. Fauci questions other people have not: When can I go back to my life and the kinds of activities I find important? He was able to articulate that.
Transforming Care: How much vetting do you do of people who are providing medical advice on YouTube?
Graham: We don’t pre-vet any content that is posted to YouTube, but of course we look toward authoritative organizations when it comes to choosing partners to collaborate with. The core of this is science, so what we try to do is use credible scientific partners, whether it be the U.S. Centers for Disease Control and Prevention, the World Health Organization, or the National Institute of Allergy and Infectious Diseases. There are also a lot of clinicians like Kimberly Manning, M.D., a general internist in Atlanta, who are able to break down the science in real terms. So for us, when we select partners we want to make sure that the source is authoritative, scientific, and is able to articulate the evidence. Then, we work with the creators to help them make their content engaging.
Transforming Care: One of the challenges of the pandemic has been that information is evolving. How do you put out good information when it changes so quickly? How do you keep people’s trust?
Graham: In medicine, we’ve never been good at explaining trials and studies, so people don’t understand that as science evolves, a study may come out one day and a bigger study may come out another day, and they can be conflicting. One of the things I’ve learned about people is once they understand a process, they can understand the outcome. They don’t just want to know whether the medicine is good: they want to know how many people you tested it on. They want to know what the side effect profiles are — all these things we are now making more transparent with the vaccine process. Early on in the pandemic, as we were getting information from smaller studies, we were passing it on without helping people understand these were initial pieces of information. Now that we want the public to participate in vaccination, their understanding the scientific process that is bringing this to their homes and into their bodies is important. It’s a very valid process and one that the public should feel reassured and safe in.
Transforming Care: What might that look like in terms of explaining the process? Is it being more transparent about the limits?
Graham: We need to be transparent, engaging, and informative. We also need to put ourselves in the shoes of the person receiving the information. As a clinician, I’m explaining diagnoses, and I get caught up in the studies that gave me the information. But the person looking at it, listening to me, doesn’t care about acronyms that only have meaning to clinicians and researchers or the impact factor of the journal. They want to know what does this mean for me? Put this in the context of my life. By getting this vaccination, it will allow you to visit your grandchildren more if you’re a grandparent or it’ll allow your community to become more economically vibrant. Fat Joe allows you to contextualize the science in that person’s life without saying that’s what he doing.
Transforming Care: Do you see a scenario where doctors would be prescribing videos or helping people navigate through and find information?
Graham: I think so. On average, patients may spend two hours or three hours a year with their doctor if they have a chronic condition. There are all those thousands of other hours. I can foresee a day where doctors figure out how to extend their impact. Video may help reinforce what they learned during visits and help them carry on with their lives and make the right decisions. I think we are in a phase where people expect more from our communication.
Publications of Note
Recommendations for Strengthening Medicaid Programs
In a commentary in the Journal of the American Medical Association, Rebekah E. Gee, M.D., M.P.H., former secretary of the Louisiana Department of Health; David Shulkin, M.D., former secretary of Veterans Affairs; and Iyah Romm, CEO of Cityblock Health, outline five principles for strengthening state Medicaid programs, which now cover more than 75 million Americans. Their recommendations take aim at high churn rates that create disruptions in care for patients and discourage providers from entering value-based payment contracts. They also call for new infrastructure to help states manage operations, compare performance, and engage in innovation, including putting greater emphasis on the nonmedical determinants of health. Rebekah E. Gee, David Shulkin, and Iyah Romm, “A Blueprint for Comprehensive Medicaid Reform,” Journal of the American Medical Association 325, no. 7 (Feb. 2021):619–20.
Adults with Functional Limitations and American Indian/Alaska Natives Among Groups at Highest Risk for Deaths of Despair
Researchers who followed respondents to the 2008 American Community Survey through 2015 found the overall mortality rate for suicides, poisonings, and chronic liver disease was 41.3 deaths per 100,000 person-years. Groups at highest risk for such deaths included adults with functional disabilities (102.8 deaths per 100,000 person-years), American Indian/Alaska Native people (102.6), working-age adults who are not employed (77.3), separated or divorced people (76.5), people with net income losses (70.6), and people with military service (67.0). Mark Olfson et al., “Deaths of Despair: Adults at High Risk for Death by Suicide, Poisoning, or Chronic Liver Disease in the U.S.,” Health Affairs 40, no. 3 (March 2021):505–12.
Racial Disparities in Excess Deaths Varied Substantially Among States
Researchers found racial and ethnic disparities in excess all-cause mortality rates varied substantially among states in the early part of the pandemic. Analyzing data from April 2020, they found nationwide adjusted excess all-cause mortality was 6.8 per 100,000 for Blacks, 4.3 for Hispanics, 2.7 for Asians, and 1.5 for whites. Michigan and Louisiana had markedly different rates of Black mortality as did Pennsylvania compared with Rhode Island. They found Wisconsin experienced no significant excess mortality among whites but had significant Black excess mortality. More research is needed to understand the drivers of geographic variation to develop policy responses, the authors say. Maria Polyakova et al., “Racial Disparities in Excess All-Cause Mortality During the Early COVID-19 Pandemic Varied Substantially Across States,” Health Affairs 40, no. 2 (February 2021):307–16.
Racial Disparities in Heart Attack Outcomes Linked to Nurse Staffing Levels
Researchers studying disparities among patients who had a heart attack while hospitalized found the odds of survival were lower for Black patients than white patients (odds ratio of 0.70). They also found that each additional patient per nurse lowered the odds of survival for Black patients (odds ratio of 0.92) more than for white patients (odds ratio of 0.97). The authors say the benefits of being admitted to hospitals with better staffing may be more pronounced for Black patients. The study relied on data for 14,132 patients from 75 hospitals in four states. Carthon Brooks et al., “Better Nurse Staffing Is Associated with Survival for Black Patients and Diminishes Racial Disparities in Survival After In-Hospital Cardiac Arrests,” Medical Care 59, no. 2 (February 2021):169–76.
An Alternate Approach to Defining Safety-Net Status
In a commentary in the New England Journal of Medicine, the authors suggest a new method of defining safety-net institutions. Rather than using a binary approach that depends heavily on metrics such as uncompensated care, they recommend creating a composite, sliding-scale measure. The scale could include the percentage of the patient population covered by Medicaid, a geographic measure of socioeconomic disadvantage, a measure of the proportion of services provided to racial and ethnic minorities, and a measure of the institution’s community benefit spending and provision of essential but unprofitable services, among other variables. Creating such a scale would also allow for a more equitable distribution of funding and enable more accurate peer comparisons in pay-for-performance and alternative payments models, the authors say. Paul Chatterjee, Benjamin D. Sommers, and Karen E. Joynt Maddox, “Essential but Undefined — Reimagining How Policymakers Identify Safety-Net Hospitals,” New England Journal of Medicine 383, no. 27 (Dec. 2020):2593–95.
Adjusting Lab Values for Kidney Disease Function May Reduce Outcomes Disparities for Black Patients
Researchers simulated the effect of eliminating a race-multiplier used to assess kidney function in patients with chronic kidney disease (CKD). They found eliminating the adjustment of estimated glomerular filtration rate equations, which assign higher values to Black patients, would reclassify a third of Black patients as having a later and more severe stage of CKD. With this change, roughly 3 percent of patients would newly qualify for kidney transplant prioritization. The study was based on an analysis of medical records at Partners HealthCare System. Salman Ahmed et al., “Examining the Potential Impact of Race Multiplier Utilization in Estimated Glomerular Filtration Rate Calculation on African-American Care Outcomes,” Journal of General Internal Medicine 36, no. 2 (February 2021):464–71.
Capacity for Electronic Communications Plays a Key Role in PCMH Savings
Researchers assessing the relative contributions of different features of the patient-centered medical home (PCMH) model to savings found that, overall, the model was associated with a greater than 8 percent reduction in total health care expenditures. The savings came from significant reductions in emergency department (ED) use and outpatient care, as well as lab and imaging studies. The authors segmented practices into three groups: those with a relatively low level of PCMH implementation and two clusters with more extensive adoption of PCMH capabilities. They found that while all three groups achieved reductions in outpatient care, the reduction in ED utilization was driven by practices that had enhanced their electronic communications, potentially increasing access for patients. The authors say more research is needed to assess the impact of variation in PCMH capabilities on health outcomes. Philip Saynisch et al., “Evaluating Approaches to Patient-centered Medical Home Implementation,” Medical Care 59, no. 3 (March 2021):195–201.
Analysis of Health System–Sponsored Housing Program Quantifies Societal Benefit
Researchers evaluating the benefits of Bon Secours Hospital’s Housing for Health program, an affordable housing program in Baltimore, Md., found the program generated between $1.30 and $1.92 of social return in the community for every dollar in yearly operating costs. The analysis took a more expansive view of benefit, going beyond traditional return-on-investment or cost-effectiveness analyses by quantifying returns to residents and the city, as well as the health system. Bon Secours currently has 801 units of affordable housing across 12 properties in West Baltimore. Emmanuel Fulgence Drabo et al., “A Social-Return-on-Investment Analysis of Bon Secours Hospital’s ‘Housing for Health’ Affordable Housing Program,” Health Affairs 40, no. 3 (March 2021):513–20.
Recommendations for Improving Medicare’s Value-Based Payment Programs
In a commentary in the Journal of the American Medical Association, the authors review the problems and successes of Medicare’s value-based payment programs and offer suggestions for improving them to ensure they benefit patients and achieve savings while reducing administrative complexity for practices. They note successful programs use population-based models that assign beneficiaries, often prospectively, to clinician groups, using global spending targets and sharing the risk of savings and losses. Kenton J. Johnston, Jason M. Hockenberry, and Karen E. Joynt Maddox, “Building a Better Clinician Value-Based Payment Program in Medicare,” Journal of the American Medical Association 325, no. 2 (Jan. 2021):129–30.
Geographic Disparities in Mortality Rates for Dual Eligibles
A study contrasting mortality rates among people who were dually eligible for Medicare and Medicaid, known as dual eligibles, in rural and urban communities found all-cause mortality rates for both groups declined between 2004 and 2017, but the declines were more pronounced among urban beneficiaries. In rural communities, the mortality rate among dual eligibles declined from 96.6 to 92.7 per 1,000, a 4 percent decline. Among urban beneficiaries the mortality rate dropped from 86.9 to 72.8 per 1,000, a decline of 16.2 percent. The researchers found rural mortality rates were highest in East North Central states and increased modestly in West North Central states during the study period. Emefah Loccoh et al., “Rural-Urban Disparities in All-Cause Mortality Among Low-Income Medicare Beneficiaries, 2004–17,” Health Affairs 40, no. 2 (February 2021):289–96.
Joint Replacement Program Reduces Postacute Care Use, Readmissions But Not Disparities Between Medicare Beneficiaries and Dual Eligibles
Medicare’s Comprehensive Care for Joint Replacement model is a mandatory bundled payment program for hospitals in randomly selected metropolitan statistical areas. Researchers studied its effects on three groups of patients who underwent hip or knee surgery — Medicare beneficiaries, those who were dually eligible for Medicare and Medicaid, and Medicare beneficiaries who had partial Medicaid benefits — to assess whether the program reduced persistent disparities between dual eligible and Medicare-only patients. They found that the program was associated with reduced stays at skilled nursing facilities and fewer unplanned hospital readmissions among all three groups, but it did not reduce disparities between them. Yue Li, Meiling Ying, Xueya Cai, and Caroline P. Thirukumaran, “Association of Mandatory Bundled Payments for Joint Replacement with Postacute Care Outcomes Among Medicare and Medicaid Dual Eligible Patients,” Medical Care 59, no. 2 (February 2021): 101–10.
Telehealth Visits with CHWs Lead to Improved Diabetes Outcomes for Latinx Patients
A study of TIME, an intervention that relies on community health workers (CHWs) to improve glycemic control among Latinx patients with type 2 diabetes, found that compared with a control group, participants experienced significant decreases of hemoglobin A1c, saw improvements in blood pressure levels and had greater adherence to nutrition guidelines within six months. Weight changes were not significant between groups. As part of TIME, which stands for Telehealth-supported, Integrated care with CHWs, and MEdication-access program, CHWs communicated with patients via videoconferencing and helped them navigate the health care system. They also identified barriers to care, including accessing medication, that may have gone unrecognized otherwise. The authors recommend larger trials to determine the scalability and sustainability of the intervention. Elizabeth M. Vaughan et al., “A Telehealth supported, Integrated care with CHWs, and MEdication-access (TIME) Program for Diabetes Improves HbA1c: a Randomized Clinical Trial,”Journal of General Internal Medicine 36, no. 2 (February 2021):455–63.
Editorial Advisory Board
Special thanks to Editorial Advisory Board member Clemens Hong for his help with this issue.
Jean Accius, Ph.D., senior vice president, AARP
Anne-Marie J. Audet, M.D., M.Sc., senior medical officer, The Quality Institute, United Hospital Fund
Eric Coleman, M.D., M.P.H., director, Care Transitions Program
Marshall Chin, M.D., M.P.H., professor of healthcare ethics, University of Chicago
Timothy Ferris, M.D., M.P.H., CEO of Massachusetts General Physician Organization and professor of medicine at Harvard Medical School
Don Goldmann, M.D., chief medical and scientific officer, Institute for Healthcare Improvement
Laura Gottlieb, M.D., M.P.H., assistant professor of family and community medicine, University of California, San Francisco, School of Medicine
Martha Hostetter and Sarah Klein, “Beyond the Survey: Engaging Patients and Communities as Partners,” Transforming Care (newsletter), Commonwealth Fund, Apr. 8, 2021. https://doi.org/10.26099/cav5-ww97