St. Louis Mayor Tishaura Jones holds 7-month-old Jaylen Taylor in the Walnut Park East neighborhood of St. Louis on July 21, 2021. The local health coalition FLOURISH St. Louis brings together representatives of the city and county health departments, local health systems and health plans, and community-based organizations to reduce Black infant mortality rates through better support for families. Photo: Nick Schnelle for Washington Post via Getty Images
St. Louis Mayor Tishaura Jones holds 7-month-old Jaylen Taylor in the Walnut Park East neighborhood of St. Louis on July 21, 2021. The local health coalition FLOURISH St. Louis brings together representatives of the city and county health departments, local health systems and health plans, and community-based organizations to reduce Black infant mortality rates through better support for families. Photo: Nick Schnelle for Washington Post via Getty Images
Toplines
By listening and responding to what residents say they need to be healthy — like better transportation and safe housing — local health coalitions in California, Missouri, and New Jersey are helping to restore trust in public health
Community residents may view the root causes of health disparities differently from health departments and care providers
Toplines
By listening and responding to what residents say they need to be healthy — like better transportation and safe housing — local health coalitions in California, Missouri, and New Jersey are helping to restore trust in public health
Community residents may view the root causes of health disparities differently from health departments and care providers
In June 2022, the Commonwealth Fund convened the Commission on a National Public Health System to think through the hard lessons of the coronavirus pandemic, which has taken more American lives than all wars since the nation’s founding. In its report, Meeting America’s Public Health Challenge, the commission pointed to a key issue: just as our country lacks a system to ensure all people can access health care, we lack a national system for fighting disease and promoting health. While there are nearly 3,000 state, local, tribal, and territorial public health departments, there’s no central body to direct efforts.
Commission members offer recommendations on how to build a national public health system that start with nominating a federal leader and appropriately funding the work; the U.S. spends just one to two cents on public health for every dollar invested in health care. But they acknowledge that taking these steps will not solve a deeper problem: “the public health enterprise is facing a crisis in trust.” Too many Americans have lost faith in the health care system overall, and in their government’s ability to keep them healthy in particular.
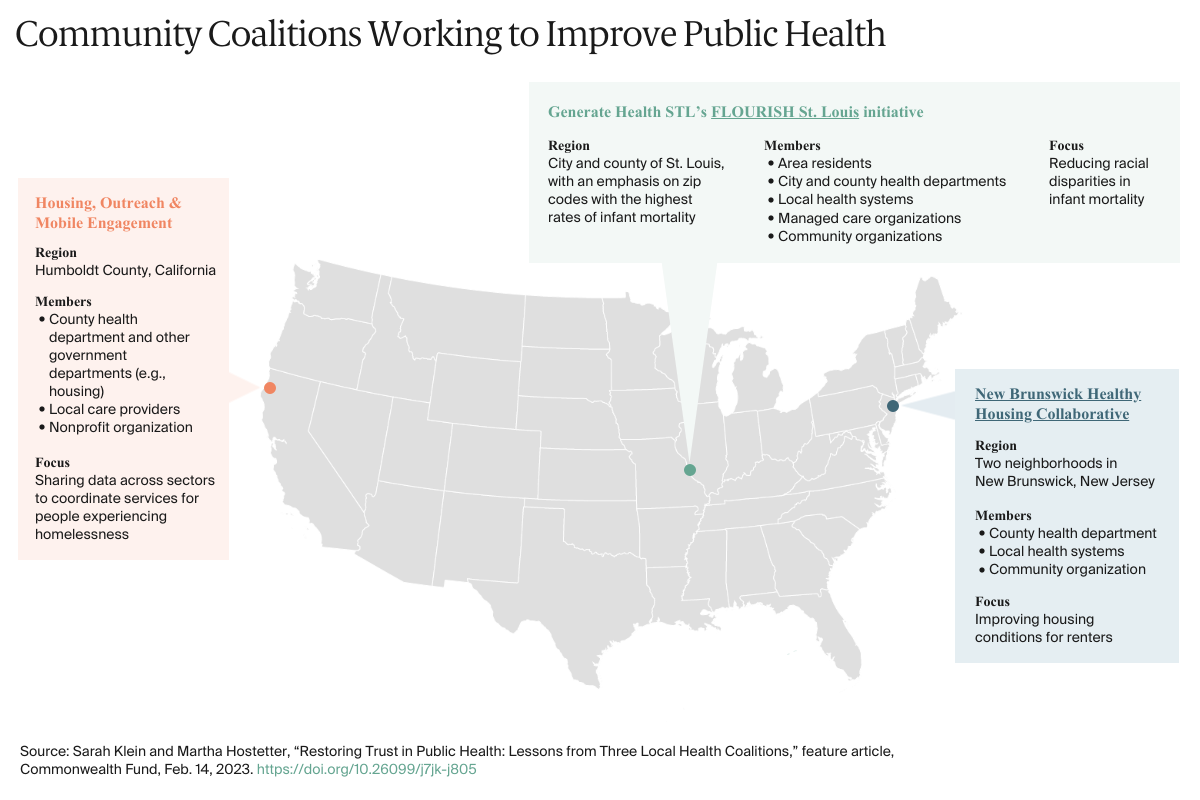
In this feature, we consider what it might take to restore trust in public health. Instead of taking a national view, we profile local initiatives that work to rebuild trust by listening to and acting on what residents of different communities say they need to be healthy. While all involve city or county health departments, the efforts also engage medical providers, health plans, and community organizations. And rather than focusing on traditional public health issues like preventing the spread of infectious diseases or curbing chronic conditions, they target upstream factors such as lack of transportation or unsafe housing that have an outsized impact on health.
None of the coalitions directly address the distrust of public authorities on display when people protested against COVID-19 vaccination and masking requirements during the pandemic. But by strengthening social ties among public health agencies, health care providers, and community residents, they may lay the groundwork for more trusting relationships in the future.
Helping Black Families Thrive by Engaging People with Lived Experience
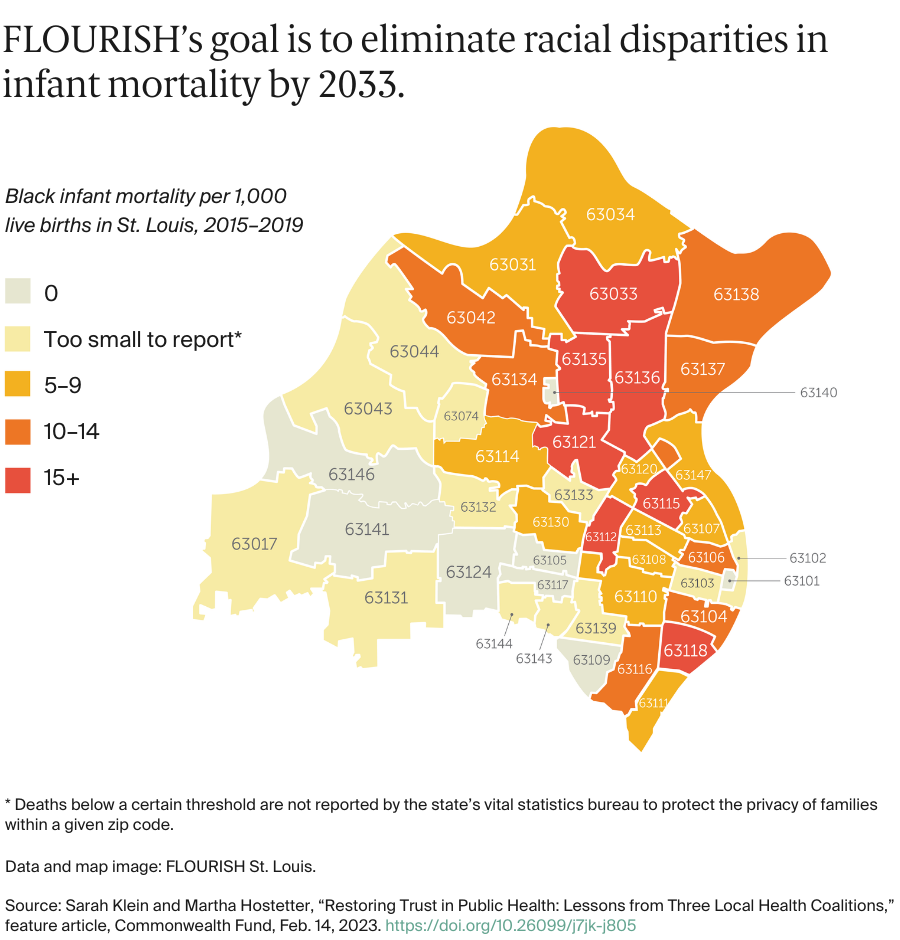
FLOURISH St. Louis is an initiative led by residents of St. Louis, Missouri, neighborhoods with the highest rates of infant deaths. Formed in 2015 by the nonprofit coalition Generate Health STL, it brings together representatives of the city and county health departments, local health systems and health plans, and community-based organizations in an effort to reduce Black infant mortality rates through better support for families.
Infant mortality is most often linked to preterm births and low birth weight, both of which may be preventable with timely and effective prenatal care. Yet in St. Louis and the surrounding county, Black pregnant people, even those with insurance coverage, are much less likely than other pregnant people to receive adequate prenatal care: more than one-third of Black women had fewer than five prenatal visits over the course of their pregnancy. In contrast, fewer than 10 percent of white women had five or fewer prenatal visits.
In 2017, FLOURISH launched “listening sessions” in neighborhoods with high infant mortality rates to learn from Black families what would help them access prenatal care. The group concentrated on two zip codes where nearly 90 percent of pregnant people are covered by Medicaid but fewer than 40 percent receive adequate prenatal care. At the 17 sessions, held over two years in churches, health centers, and community organizations, transportation emerged as a consistent problem. Many of the 350 participants said getting to medical appointments, pharmacies, and grocery stores required navigating long distances, often through dangerous neighborhoods and, in some cases, streets without sidewalks. “People were walking on major roads or trying to push strollers through grass,” says Kendra Copanas, executive director of Generate Health STL, the nonprofit that oversees the work.
The sessions also revealed that Medicaid managed care plans were using the city’s bus system as the default option for members’ transportation benefit. The erratic nature of bus schedules and lack of seating and safety at bus stops discouraged people from relying on the system. “The degree to which it wasn’t working for families was startling to health systems, which had heard about transportation barriers before but felt it was someone else’s problem to solve,” Copanas says.
To engage residents in brainstorming solutions, FLOURISH partnered with Vision for Children at Risk, a family advocacy organization with strong ties to St. Louis’s Black community that ran a Transportation Community Café. Over eight months, people who had struggled to find reliable transportation joined with leaders from Medicaid managed care plans and the transit authority to identify better alternatives for travel to and from prenatal visits. “We wanted families who were most affected to be heard in a way they generally haven’t been,” Copanas says.
Video courtesy of FLOURISH St. Louis.
This exercise, along with feedback from other community residents, led to a long list of suggestions. One was to streamline and standardize protocols for requesting nonemergency medical transportation from Medicaid plans and change plan policies to allow people to travel with their small children to medical appointments. One of the plans began offering car service, instead of bus vouchers, and added Lyft and Uber to its network so that members had another option if the car service wouldn’t arrive in time to make an appointment, a not-infrequent occurrence.
The group also developed a Medicaid Riders’ Bill of Rights, although Copanas says it has been difficult to monitor the extent to which plans are adhering to it. In part, this is because health plans have not supplied requested data on use of medical transportation for nonemergencies, making it difficult to assess the impact of policy changes on health outcomes.
Recognizing that strengthening maternal and infant health requires a layered approach, the coalition’s members have focused on issues other than transportation. For example, they’ve trained care providers on ways to recognize and reduce their own biases, as many pregnant people said they had been treated poorly by their providers because of their race or ability to pay. And they’ve improved conditions at a public housing complex by getting the city to address a mice infestation, among other efforts.
Training Residents to Serve as Health Ambassadors
In the Esperanza and Unity Square neighborhoods of New Brunswick, New Jersey, more than 80 percent of residents are Latino, close to 40 percent are immigrants, and many speak Spanish only. New Brunswick Tomorrow, a community-based organization launched over 40 years ago to improve the quality of life for city residents, has long been concerned about living conditions in these neighborhoods, where lack of investment by some landlords has led to dilapidated housing conditions.
The organization’s staff had heard stories of people with health problems from moldy basements where water had pooled; windows that didn’t open or didn’t lock; and pest infestations. Between language barriers and fears of eviction or immigration enforcement, many were unwilling to assert their rights as tenants, if they were aware of those rights at all, says Manuel J. Castañeda, New Brunswick Tomorrow’s director of community health.
In 2017, the organization joined forces with the area’s two hospitals (Robert Wood Johnson University Hospital and Saint Peter’s University Hospital) and the county health department to form the New Brunswick Healthy Housing Collaborative, an effort to engage and empower residents to improve housing conditions. With an award from the BUILD Health Challenge, the collaborative hired and trained 12 Spanish-speaking residents to serve as community health ambassadors who would attend community events in churches, day care centers, and other facilities to share information about health hazards in the home, from lead paint and carbon monoxide to pests and mold. When the COVID-19 pandemic began, they leveraged meetings about eviction moratoriums to drive home these points.
“Home Is Where the Heart Is,” a 2021 painting from New Jersey artist Krishna Schroth, pays tribute to the community health workers who work with the New Brunswick Healthy Housing Collaborative. Reprinted with the permission of the artist.
Over time, the community health ambassadors overcame residents’ fears, persuading more than 200 to allow them in their homes to conduct inspections. “We had cases where people didn’t have heat for a year because the landlord said, ‘I fixed it once and I’m not going to fix it again,’” Castañeda says. The inspections also revealed lead in soil that some families were using to grow food.
The ambassadors helped residents understand their options, including advocating for themselves, filing a complaint with the city, or seeking legal assistance. To help families who faced health risks but didn’t qualify for legal aid because of their immigration status, the Robert Wood Johnson University Hospital created a medical–legal partnership staffed by a nonprofit. Often the appearance of an attorney was enough to resolve a tenant’s problem, Castañeda says. The ambassadors have also made referrals to free clinics and other sources of primary and specialty care for families without insurance.
The New Brunswick collaborative has also sought to change the city’s housing policies by funding two reports: an overview of best practices in health-related housing policy and an examination of how local housing ordinances stacked up against these best practices. Both were a launching point for dialogue with members of the City Council, who in 2022 made several changes in response to the group’s advocacy. These included passing an ordinance that prevents landlords from holding tenants responsible for past tenants’ unpaid water bills and requires written agreements about how water bills are to be divided in multifamily houses. The city rent control office also improved its website to make it easier for prospective tenants to see previous rents and the record of tenant complaints. “The success is through that community integration piece. It was these community leaders who have stuck with us,” says Castañeda, who joined New Brunswick’s city council in 2023.
Building Bridges Across Sectors
Another major problem in public health relates to the ability of government agencies to access and share data. During COVID, timely data were often unavailable, leading to gaps in tracking disease spread and delays in getting tests and equipment to where they were needed. Sharing data across organizations requires trust, not just technical know-how.
In 2016, California’s Humboldt County partnered with the local health information exchange to create a cloud-based platform that enables care providers and local government agencies to share information about people experiencing homelessness. The size of Rhode Island, the county is home to some of the oldest redwood trees in the U.S. as well as a diverse population of back-to-the-land enthusiasts, ranchers, and cannabis farmers. Its location along California’s northern coast and tendency to become cut off from the rest of the state during mudslides have fostered a culture of self-reliance and a spirit of collaboration among medical and social service providers.
Humboldt County also has one of California’s highest per capita rates of homelessness, on par with Los Angeles. High rates of poverty, substance use, and childhood trauma, as well as a mild climate that makes outdoor living feasible, all contribute the problem. In response, the county’s Housing, Outreach & Mobile Engagement (HOME) program offers rental assistance and supportive services — including counseling, case management, and peer support — to individuals who are chronically homeless and have one or more serious disabling conditions. Many are frequent users of emergency departments (EDs) and the county’s behavioral health services and known to police and fire department personnel.
Securing permanent housing can be a multiyear process involving staff from different agencies and multiple rounds of documentation. It’s not unusual for a person who is homeless to have difficulty keeping up with the paperwork or lose a birth certificate or other ID needed to get housing. The divide between medical and social service sectors also makes it difficult to identify the supports someone is already receiving and the gaps that remain.
In partnership with the North Coast Health Improvement and Information Network (NCHIIN), Humboldt County has implemented a care coordination platform that creates a single record for each individual seeking housing. Described as “Facebook for clients,” it contains demographic information, contacts for case managers and social workers, and a secure document vault for housing applications, lease agreements, and other key documents. Tasks like preparing a newly housed person for a home inspection can be assigned to a team member, and deadlines are flagged.
The platform has enabled case managers and social workers in the health and housing departments to share information on roughly 1,000 clients since 2016 and, with their permission, obtain real-time alerts when clients are in the ED or have been hospitalized. The system also enables users to find care managers to contact for help. “We had an early win with a local woman who showed up in the ED with all her earthly possessions. She was terrified,” says Jessica Osborne-Stafsnes, NCHIIN’s chief operating officer. Hospital staff reached out to the county’s case manager, who had been worried about this client. “The case manager said, ‘Keep her there. She’s been lost to care for several weeks. We need to connect.’”
The episode built trust as well as a willingness to share more information through the platform. The county’s behavioral health agency began to feed information about upcoming appointments and admissions to a crisis stabilization unit to users who have the authority to view it; the probation department sent a list of clients enrolled in probation; and information on upcoming primary care appointments was transferred electronically from the local federally qualified health center. Jail records, which are publicly available, were also added.
The system enables medical providers and county staff to act as one another’s eyes and ears, catching people who might otherwise fall through the cracks. “If someone goes to jail, we know and we’re able to ensure the clinician there knows the person is a HOME client and that they can access his or her medical record, including their current medications,” says Jaclyn Culleton, program manager for Humboldt County’s Department of Health and Human Services.
If someone goes to jail, we know and we’re able to ensure the clinician there knows the person is a HOME client and that they can access his or her medical record, including their current medications.
Jaclyn Culleton
Program manager, Humboldt County Department of Health and Human Services
Culleton says the platform has made the process of getting people housed far more efficient. That, in turn, has contributed to sharp declines in hospitalizations and ED visits, a phenomenon the program documented through its partnership with NCHIIN. Among clients who were housed for two years, hospitalizations and ED visits fell by 63 percent and 35 percent, respectively.
NCHIIN is now partnering with the county and community organizations (through Humboldt Community Health Trust) to develop a cloud-based system that will allow social service agencies and community-based organizations to coordinate their efforts to serve clients by developing shared care plans. Through the consent-based system, clients decide whether individual service providers can access their care plan. Like the care coordination platform for people experiencing homelessness, the system will provide secure and ready access to documents needed to apply for social services. People who use these services sit on a steering committee and have been offering suggestions for how to talk to other clients about informed consent, among other issues.
Lessons for Building Sustainable Public Health Partnerships
Community leaders, policymakers, and funders across the U.S. can learn from the experiences of these three coalitions.
Trust is foundational for change.
As the Commonwealth Fund Commission on a National Public Health System notes, trust is a prerequisite for collective action. But for many marginalized communities, trust is in short supply.
One way to build trust is to learn from and empower the people you are trying to help. In St. Louis, the health impacts of poor public transportation had been well documented by local researchers, and residents had grown frustrated with sharing their opinions only to be forgotten about later on. “What the community wanted was greater access to decisionmakers and to see meaningful collaboration among agencies, systems, and individuals,” says Copanas, director of the nonprofit leading the work. To move forward, the coalition brought health plans and the transit agency to learn from residents how the services were falling short. They then formed a “community leaders cabinet” made up of 33 people who’ve lived in neighborhoods most affected by health disparities to help develop and implement new approaches. One of the initiative’s funders, the Missouri Foundation for Health, delegated authority to community members to distribute a significant share of its $3 million investment. Roughly $1 million has been given to small, mostly Black-led nonprofits, including A Red Circle, an organization that provides nutrition education and organizes group meals for pregnant and postpartum people. “Engaging with organizations that are less visible but really trusted in their community has been really important,” Copanas says.
Lloyd Michener, M.D., a professor at the Duke School of Medicine’s Department of Family Medicine and Community Health and an editor of The Practical Playbook II: Building Multisector Partnerships That Work, says his institution began to forge effective community partnerships only when leaders acted on what the community said it wanted: dental care for children covered by Medicaid. “Duke didn’t have dentists or a dental school, but we took a deep breath and said, ‘We’re going to deal with dental pain,’” Michener recounted. Creating a mobile clinic staffed by the health department and volunteer dentists from the community “was the beginning of trust in a partnership that goes to this day.”
To foster such responsiveness, the BUILD Health Challenge requires that community organizations lead the initiatives it funds and that a local hospital match its award. This structure ensures each partner’s work is aligned with the priorities of communities, which may see the root causes of health disparities differently from health departments and care providers.
Community coalitions can be hard to sustain.
It takes time to gather input from residents and build consensus on priorities. That process becomes more challenging as leaders and grants come and go. In Humboldt County, collaboration has been ongoing for years through programs such as Aligning Forces for Quality and the Accountable Communities for Health. While the initial efforts didn’t always achieve their intended aims, they helped build trusting relationships among participants. “Everyone wants to get to that pinnacle solution right now, but we’ve had some success in building that brick by brick. Along with that comes the trust and partnership you need to make those efforts sustainable in the long run,” Osborne-Stafsnes, chief operating officer of the health information exchange, says.
Copanas says the FLOURISH St. Louis initiative has engendered collaboration among county health departments and hospitals and increased hospitals’ interest in anchor mission work, which enables hospitals to leverage their hiring and purchasing power to effect social change. The initiative also led to an academy to train and foster community leaders. The graduates serve as champions, mobilizing their networks and helping with data collection.
Community health workers like the ambassadors deployed in New Brunswick can also serve as a bridge between residents and leaders of health and other organizations, helping to keep partnerships together.
Successful partnerships depend on transparency.
Assessing the effectiveness of community health initiatives requires medical providers and health plans to share data. The St. Louis and New Brunswick projects have been constrained by the unwillingness of plans or providers to share information needed to assess, for example, whether use of nonemergency medical transportation in some neighborhoods increased or whether ED visits for asthma decreased when housing conditions improved.
Ensuring access to such data may require clearer mandates from states and funders. Public data repositories such as Healthy Places Index 3.0, which enables comparisons of community conditions across regions and time, can be a place to start. “I’m a firm believer that you use existing public data to go and have conversations with communities. What you find is that there’s sometimes a different interpretation at a community level of what the data mean,” says Mary Pittman, Dr.P.H., president and CEO of the Public Health Institute, a nonprofit focused on strengthening the nation’s public health care system. These conversations can also identify where gaps in data exist, she says.
Moving Forward
As the work of these local health coalitions demonstrate, building health is not so much an endpoint as an ongoing process, one requiring trusting partnerships that go well beyond public health departments. “There were bright spots across the country during COVID, where community organizations, health care, and public health were coming together to identify problems on the ground and quickly deploy solutions,” says Duke’s Michener. “The need for those kinds of local partnerships is a lesson that comes up in every pandemic, going back as far as you could trace. And yet we seem to keep losing the thread.”
Sarah Klein and Martha Hostetter, “Restoring Trust in Public Health: Lessons from Three Local Health Coalitions,” feature article, Commonwealth Fund, Feb. 14, 2023. https://doi.org/10.26099/j7jk-j805