Driving Changes in Commuting Practices
The environmental stewardship team’s visits to hospitals are an opportunity to observe successful practices and promote new ones. “They quickly gain credibility because they have so much data and expertise,” says Jared Amerson, chief administrative officer of Providence Saint John’s Health Center, a 266-bed hospital in Santa Monica, Calif. His hospital, with 1,500 employees and 1,000 physicians, is a high performer in the commuting category even though some staff drive up to 1.5 hours each way to work. “We’re in a community where very few people can afford to live,” Amerson says.
The health center spends roughly $200,000 each year incentivizing staff to avoid single occupancy travel and assigns a staff person to help identify other options. The hospital pays for public transportation; it also pays employees $5 for each day they don’t park on site. For those willing to carpool in groups of three or more, the hospital leases vans and provides free gas and parking.
Amerson has been toying with creating charter bus routes to ferry people from downtown Los Angeles and the San Fernando Valley but hasn’t pulled the trigger because of the challenges of scheduling. Unlike most businesses where employees are arriving and leaving at roughly the same time, hospital schedules vary based on an employee’s role, making it difficult to get the timing right.
Reporting Progress Toward Carbon Negative Emissions
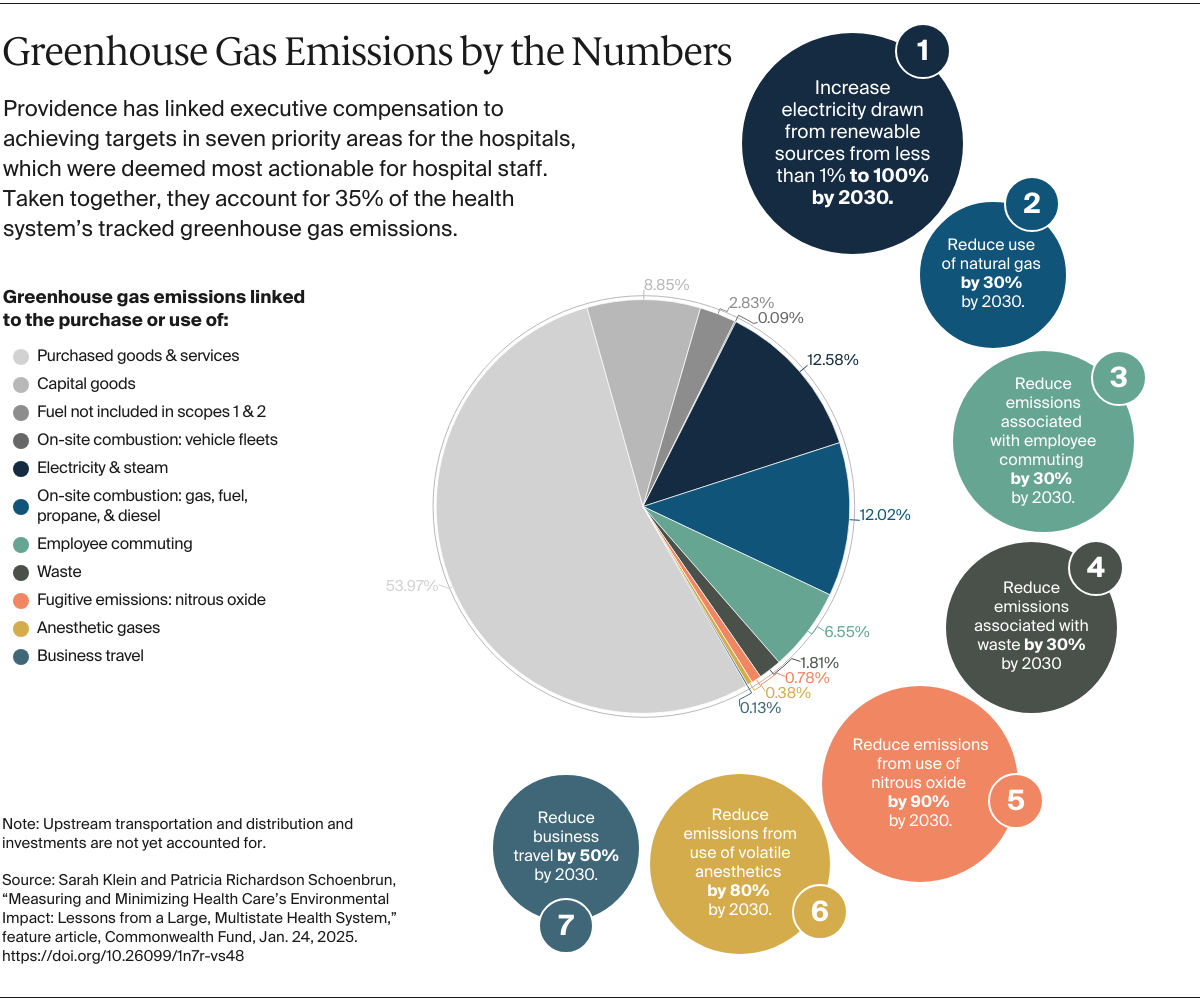
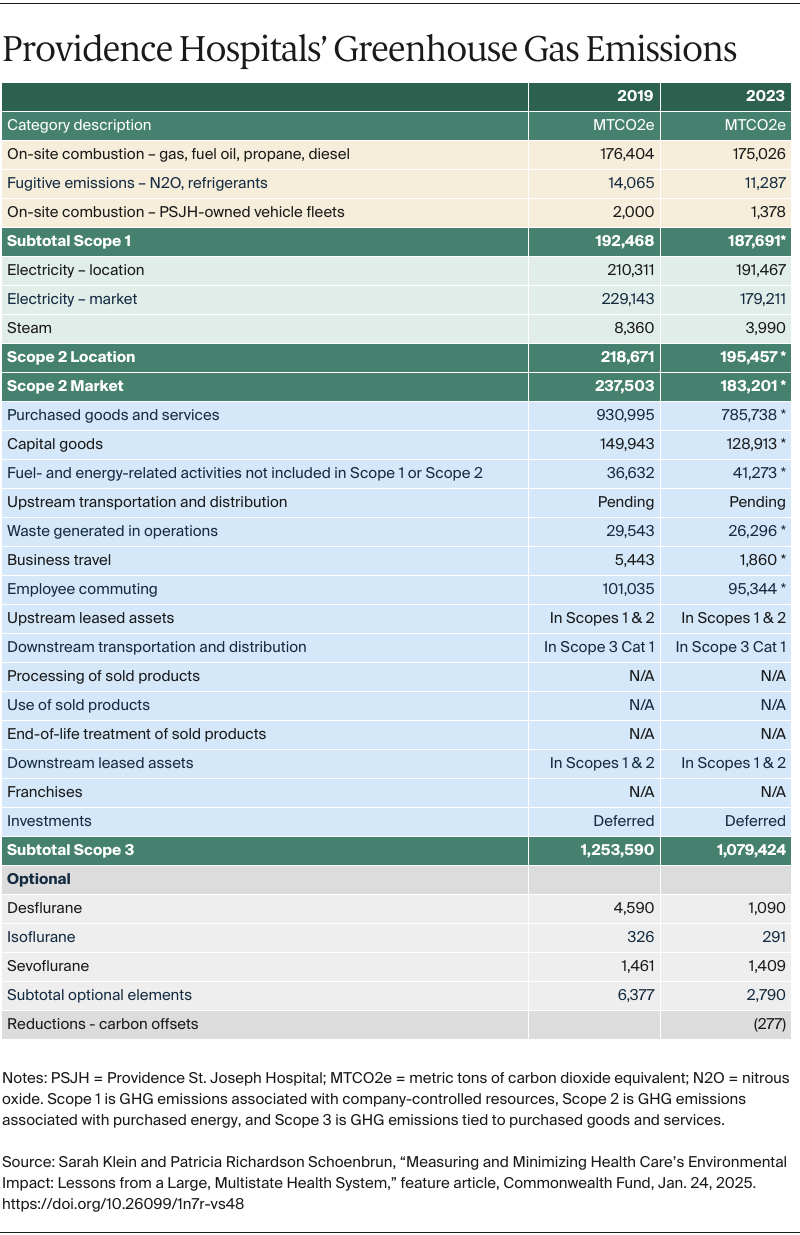
Since setting its carbon negative goal in 2020, Providence has reduced greenhouse gas emissions in the categories it prioritized by 13 percent, from 570,369 metric tons of CO2e in 2019 to 495,526 metric tons of CO2e in 2023. Schenk expects sharper declines over the next year as a $50 million investment in LED lighting across the system bears fruit and the practices of leading hospitals are spread. For instance, decommissioning nitrous oxide supply lines in 17 California hospitals, completed in the first half of 2024, is expected to reduce greenhouse gas emissions by 4,000 metric tons. As hospitals in Alaska, New Mexico, Texas, and Washington follow suit, the system may see an additional reduction of 8,000 metric tons of CO2e.
In relative terms, the health system saw the steepest declines in emissions related to business travel (–66%), anesthetic gases (–56%), and the use of steam (–52%) and electricity (–22%, half of which came from purchasing renewable energy credits). Reductions in business travel and the use of the anesthetic gas desflurane produced immediate cost savings ($5 million and $2 million per year, respectively), while investments in lighting and water conservation are expected to pay off within three to seven years.
If Providence continues at roughly the same pace — achieving 5 percent reductions year over year — it will reduce its greenhouse gas emissions in the areas prioritized by nearly 60 percent by 2040. To become carbon neutral or negative for the broader set of greenhouse gas emissions, Providence faces two significant challenges: reducing emissions associated with purchased goods and services and retrofitting older buildings to improve energy efficiency. The former requires sweeping changes in how manufacturers worldwide produce and transport goods, while the latter requires money. In 2023, Providence partnered with the American Hospital Association and the American Society for Health Care Engineering to estimate the cost of replacing natural gas with electricity in a single hospital, Providence St. Peter Hospital in Olympia, Wash. The price tag — $80 million — was daunting, but Schenk and Glass want to demonstrate that with smart capital planning and emerging technologies, it’s feasible — and cheaper — to decarbonize existing building stock than build new structures.
Lessons for Other Health Systems and State and Federal Policymakers
As these examples from Providence illustrate, hospitals and health systems can engage their staff in meaningful efforts to mitigate their environmental impact. Others could use these lessons to inform their own efforts to reduce greenhouse gas emissions that contribute to climate change.
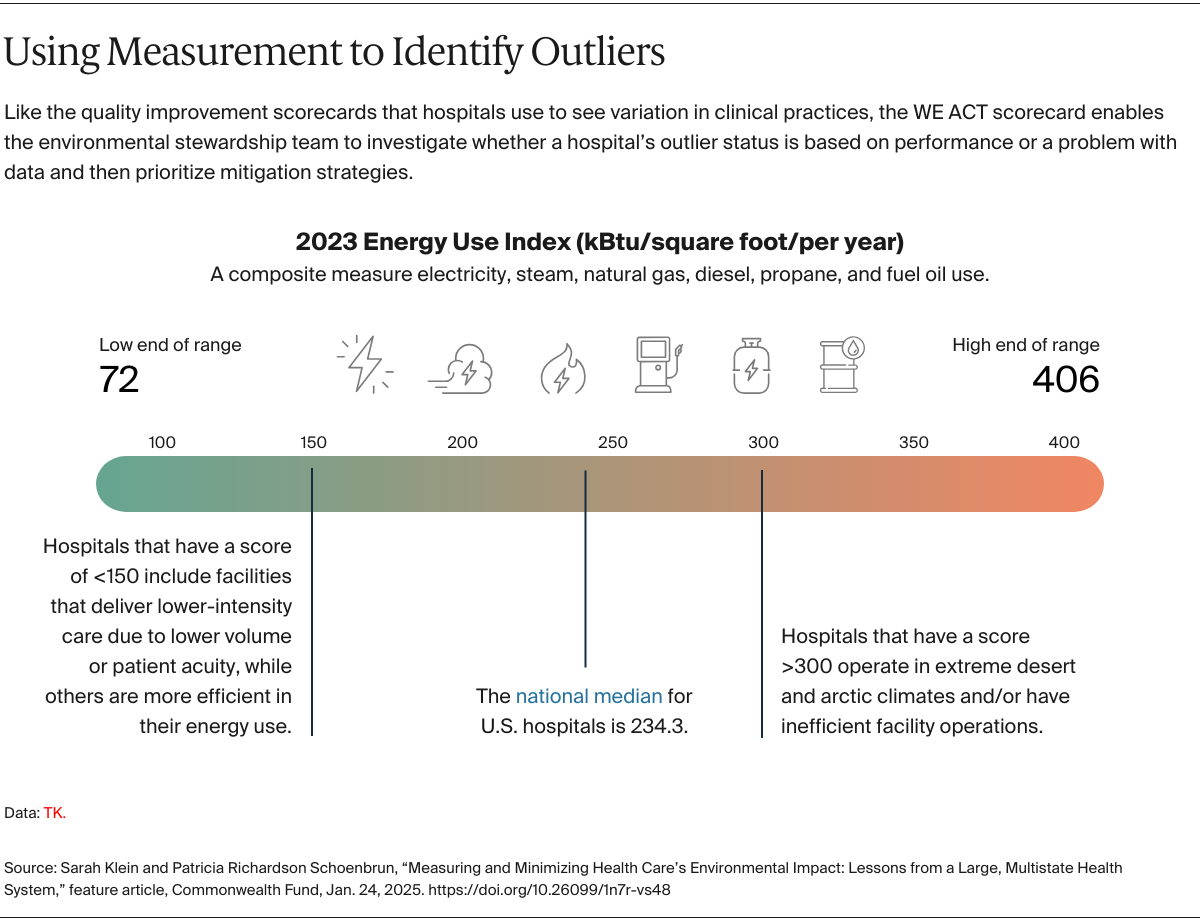
When it comes to engaging staff in carbon-reduction efforts, transparency can be a force multiplier. The Providence WE ACT scorecard is not the first or only effort to quantify hospitals’ greenhouse gas emissions in granular fashion. Aga Khan University in Pakistan and Practice Greenhealth, an organization that supports health systems in implementing environmental stewardship programs, have created Excel-based tools that health care organizations can adopt. Health systems like Penn Medicine, Cleveland Clinic, and Massachusetts General Hospital have also publicly reported their progress toward carbon-reduction goals using similar categorization. What makes Providence’s scorecard distinct is its benchmarking functionality and how that is being used to make the environmental costs of health care salient and actionable to staff at all levels. Transparency undercuts concerns about greenwashing and helps build trust among staff. Montoya says, “There are no secrets about how or why a particular project has been prioritized.” Making the data visible also promotes friendly competition. “The first thing I look at is the outliers and ask, ‘Where do we need to go to get to the top of this list?’” Mason says.
Good measurement is a balancing act. Constructing a scorecard that captures the complexities of hospital operations without overwhelming users or sacrificing accuracy is an ongoing challenge. In selecting measures, Schenk and Glass must balance their desire for precision with the limitations of existing data sets that weren’t designed with carbon accounting in mind. Take business travel as an example. Corporate accounting systems may be able to report days or dollars spent on car rentals but not miles driven, a far more accurate measure of greenhouse gas emissions. They push vendors to send electronic files with new levels of detail where it makes a material difference. In instances where the cost of capturing such data exceeds the benefit (for example with refrigerants or diesel for generators), they accept estimates. They are also limited to using data from vendors and health system departments that can send automatic feeds that can be updated monthly and audited. At times, it takes a lot of detective work to figure out where the data they want are hidden. Normalizing what they collect to create an apples-to-apples comparison of hospitals also requires careful thought. All energy data are adjusted to account for seasonal weather variation, and all costs are adjusted for inflation, but other measure adjustment is done on a case-by-case basis to ensure comparisons are not misleading. If this sounds challenging, neither Schenk nor Glass see it that way. “It’s a labor of love,” Schenk says.
Technical assistance is as important as data. The Commonwealth Fund’s 2023 Climate and Health Care Workforce Survey found 80 percent of clinicians surveyed wanted their employers to act on climate change, but few were offered training to identify or implement decarbonization steps in their jobs. Providence’s environmental stewardship team acts much like an in-house consulting firm, dispensing advice on how to improve. To assemble such teams, other health systems may want to recruit employees who combine expertise in engineering, nursing, or medicine with a passion for sustainability. Finding the budget for these positions may be a persistent challenge when hospital margins are thin. Providence’s five Alaska hospitals split the cost of hiring Darcy Moxon, sustainability program manager. Moxon, who has Six Sigma expertise, helps hospital leaders and staff find opportunities for carbon savings in a state where municipal recycling is severely limited. Schenk is exploring other ways to fund these positions, including using savings from conservation efforts. The scorecard itself has helped to identify errors in utility bills and reduced the time facilities’ staff spend reviewing them. “I used to have a calendar block to just go in and monitor our utility usage. Now I just open the scorecard to see it,” Mason says.
Prioritize projects that achieve financial and carbon goals simultaneously. As Chesebro’s discovery of nitrous oxide loss and the groundskeeping team’s work at Providence St. Vincent demonstrate, employees play a critical role in identifying potential carbon savings, as well as blind spots in the health care industry’s current accounting for carbon use. Studies of the health sector’s carbon footprint point to a slew of opportunities under employees’ direct control, including reducing avoidable imaging from computed tomography (CT) and magnetic resonance imaging (MRI) scans and preventing medical errors that result in the duplication of services. Health systems can partner with staff to identify and implement projects that advance financial and environmental goals at the same time, says Vivian Lee, MD, PhD, MBA, author of The Long Fix: Solving America’s Health Care Crisis with Strategies That Work for Everyone and a Commonwealth Fund board member. To do so, health system leaders need better tools to quickly and easily assess the return on investments. “Sustainability has to become sustainable, which it’s not right now,” Lee says.
Providence’s WE ACT scorecard is a crucial step in that direction because it enables health system staff to forecast savings based on local commodity costs, state and federal incentive programs, and resource use. Requiring greenhouse gas emissions reporting from other health systems would facilitate comparisons across states, but previous efforts to compel reporting (such as by the Joint Commission) have met with pushback from the industry. If the Centers for Medicare and Medicaid Services made emissions reporting a condition of participation in the Medicare program, the field would see more progress, says Antonia Herzog, PhD, director of climate policy and advocacy at Practice Greenhealth. “That’s the holy grail.”