Abstract
- Issue: When COVID-19 began to spread, countries scrambled to implement sweeping responses across their public health and health care delivery systems. Lack of preparation often meant international leaders were slow to identify and respond to the crisis, and many health care delivery systems were overwhelmed — short on critical infrastructure, supplies, and staff. Beyond the initial challenges posed by the pandemic, its prolonged duration has strained health care facilities and providers.
- Goals: Provide specific examples of how international delivery systems adapted to respond to the pandemic and identify lessons learned that can be applied to U.S. health care delivery and public policy.
- Methods: NORC conducted a literature review and in-depth interviews of health system and government leaders in five countries: Australia, Finland, Germany, Singapore, and South Korea. An advisory board of U.S. experts informed research areas and identified opportunities for the United States.
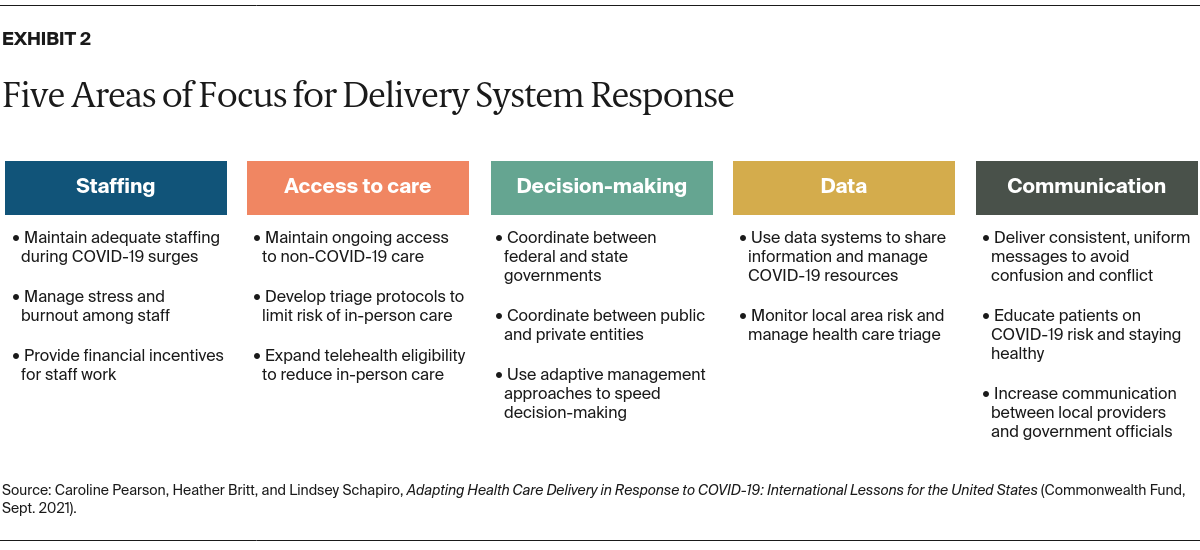
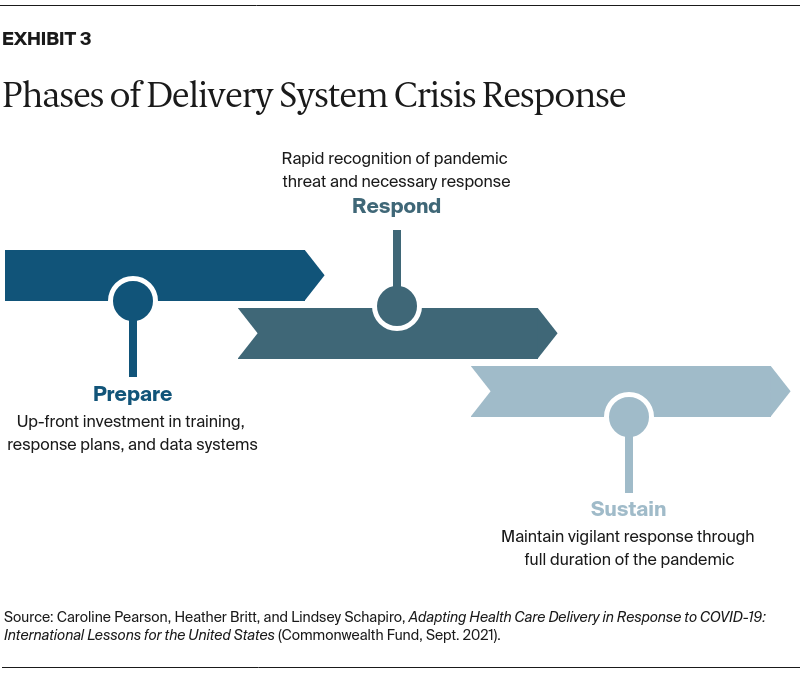
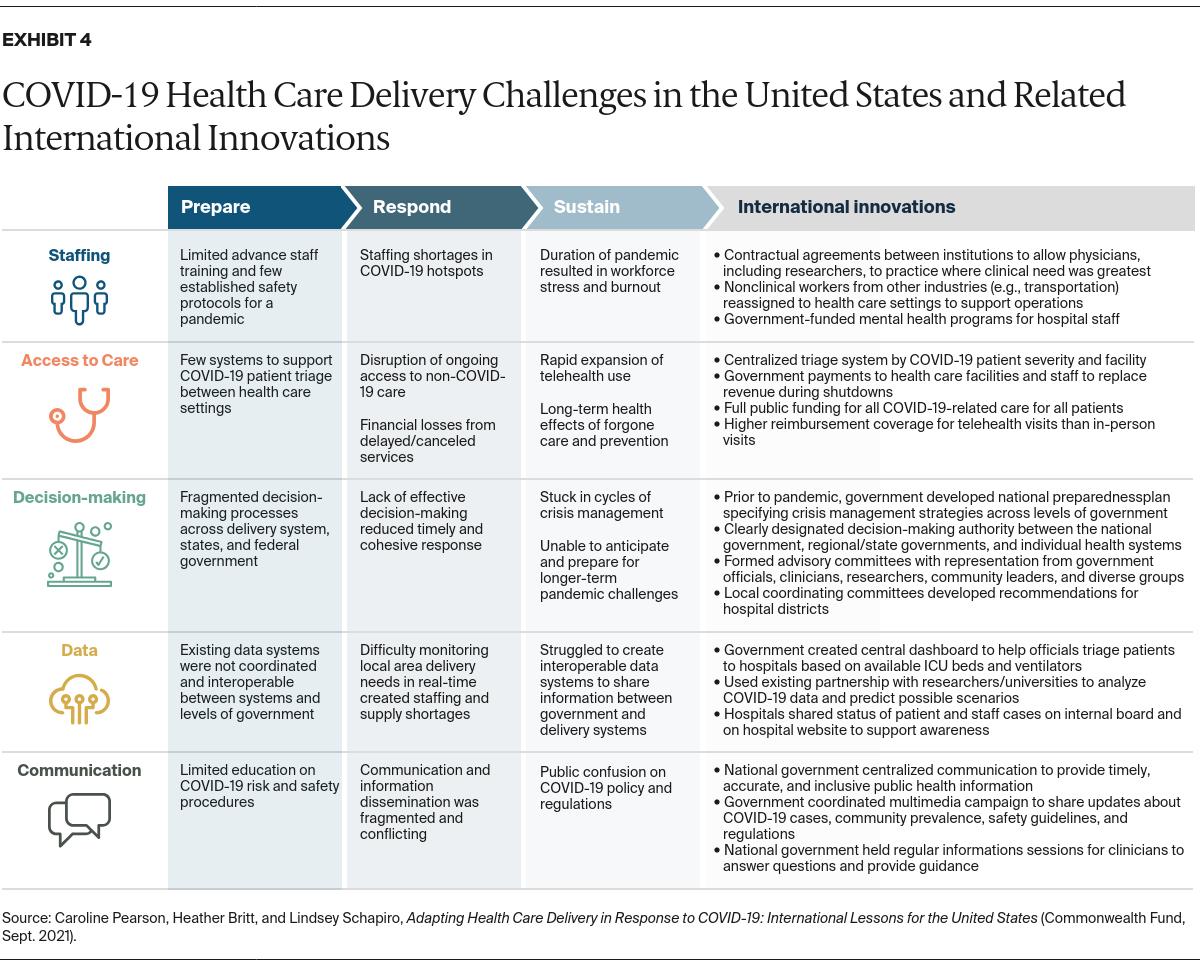
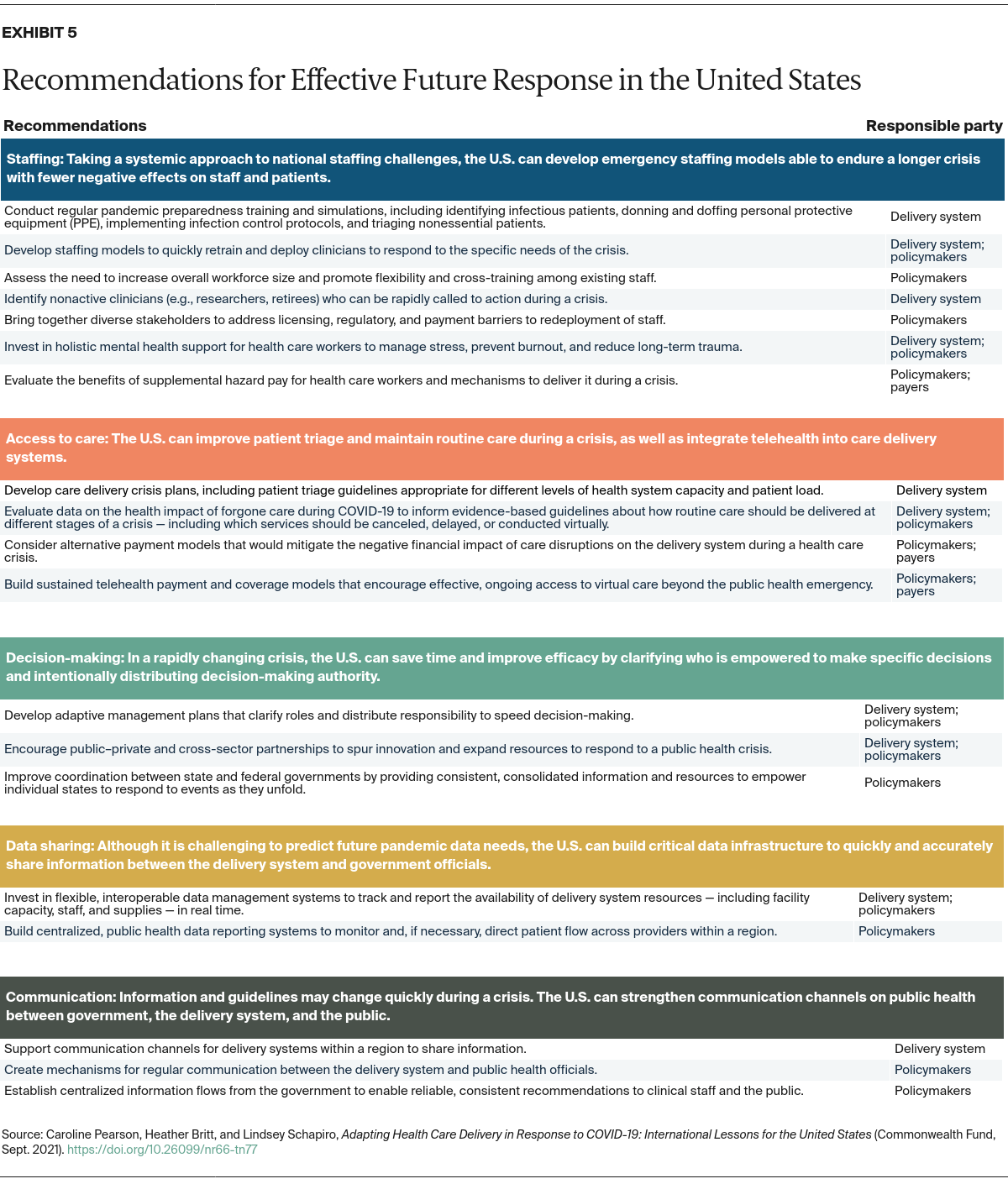
- Key Findings: Policies and actions that address staffing, access to care, decision-making, data infrastructure, and communication can help countries prepare for a pandemic, respond quickly, and sustain the response for the duration of the public health threat.
- Conclusion: As COVID-19 cases rise once again, planning and investment can help the United States confront future health crises.
Introduction
Since the outbreak of COVID-19, the U.S. health care delivery system — including hospitals and other facilities, health care workers, payers, and policymakers — has been facing unprecedented challenges. At different points during the pandemic, the virus has strained hospital capacity, disrupted supply chains, and delayed regular ongoing care and elective services, deeply affecting health systems’ finances. COVID-19 also has exacted a heavy toll — mental, emotional, physical, and financial — on the health care workforce.
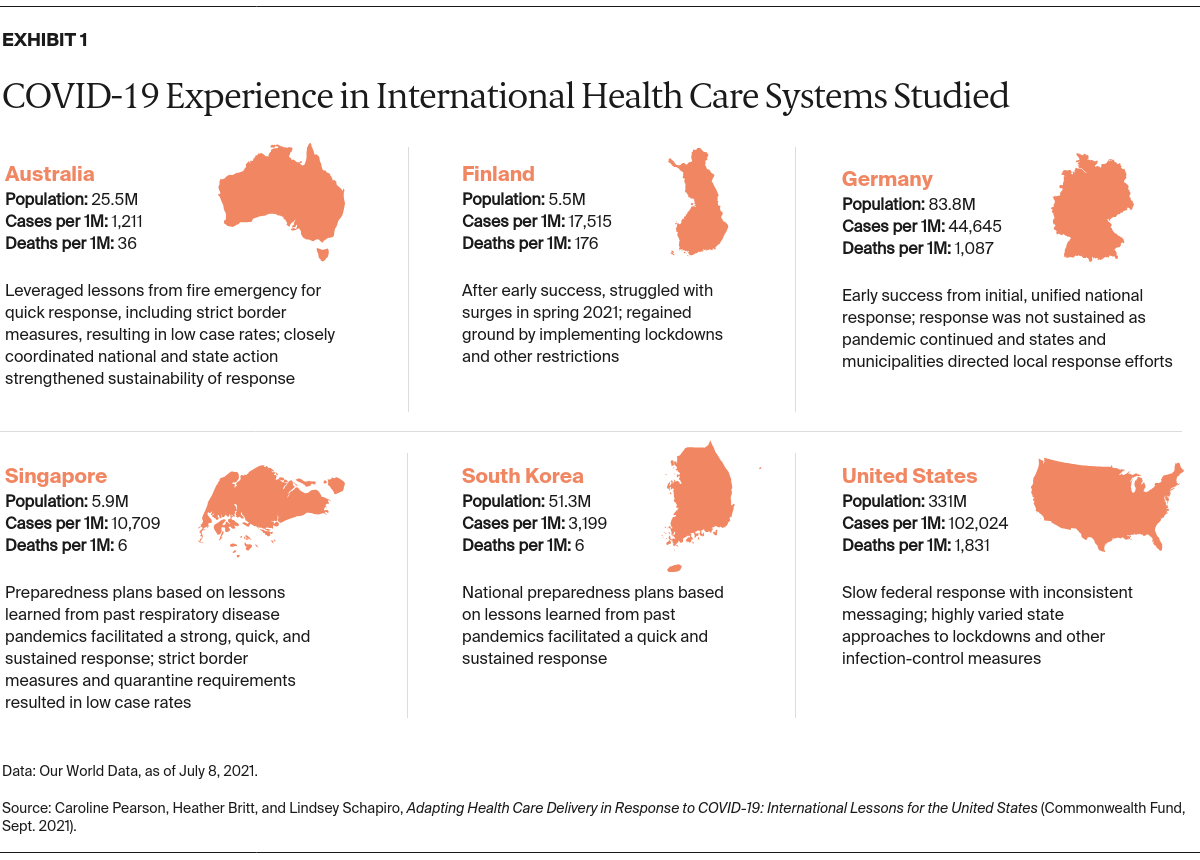
This issue brief explores how five diverse countries — Australia, Finland, Germany, Singapore, and South Korea — with advanced health care delivery systems have adapted and innovated to meet the challenges of operating during the COVID-19 pandemic, with the goal of identifying lessons for care delivery in the United States. The political structures of these countries vary, but like the U.S., Australia and Germany both have large federated systems in which national and regional or state governments share responsibility.
An advisory board of nine U.S. health care experts representing hospital administrators, physicians, and nurses from various health systems convened first to prioritize research topics and then again to assess which of the international approaches would be the most feasible and have the greatest impact in the U.S. (See “How We Conducted This Study” for further detail.) Exhibit 1 provides an overview of the countries studied.