
Abstract
- Issue: The United States spends twice as much per person on health as peer nations. Current research points to higher prices as a driving factor, but less is known about how the dollars associated with higher U.S. prices and spending are distributed.
- Goals: To identify and estimate components of excess U.S. health spending relative to peer nations.
- Methods: Review of published and grey literature comparing international health systems and analysis of Organisation for Economic Co-operation and Development (OECD) Health Statistics data with other public data.
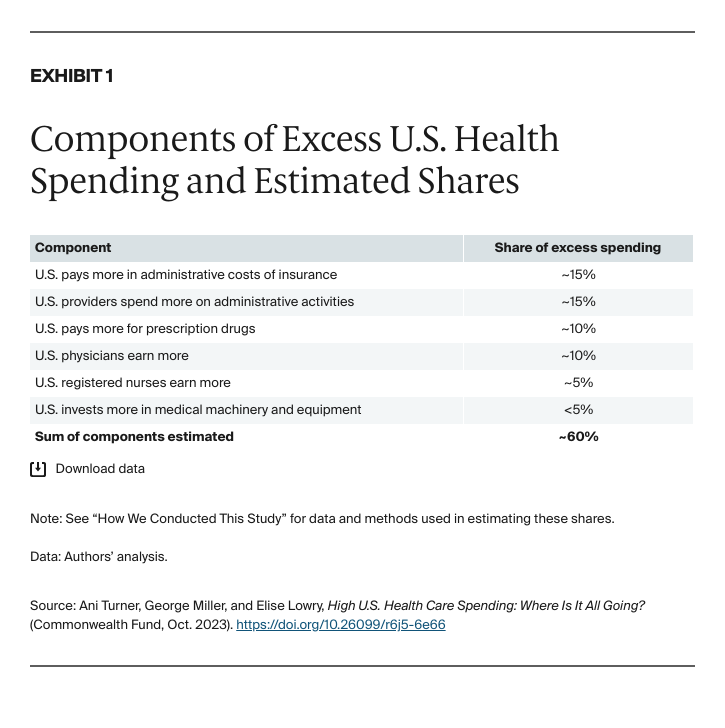
- Key Findings and Conclusion: More than half of excess U.S. health spending was associated with factors likely reflected in higher prices, including more spending on: administrative costs of insurance (~15% of the excess), administrative costs borne by providers (~15%), prescription drugs (~10%), wages for physicians (~10%) and registered nurses (~5%), and medical machinery and equipment (less than 5%). Reductions in administrative burdens and drug costs could substantially reduce the difference between U.S. and peer nation health spending.
Introduction
The United States spends twice as much per person on health as the average of peer nations.1 A number of studies have concluded that high prices are a major driver of this “excess” spending.2 A better understanding of where the excess health spending is going can guide strategies to address high spending and shed light on the populations most likely to be affected.
We examined published research, grey literature, and Organisation for Economic Co-operation and Development (OECD) data for the U.S. and comparator countries to identify potential components of higher U.S. health spending and, where possible, to estimate the order of magnitude of each component. It’s important to note that while our research was aimed at estimating “excess” spending, we were not able to definitively identify or quantify all components.
Components of Excess U.S. Health Care Spending
We were able to find evidence to support more than half of the difference in per capita health spending between the United States and the average of 12 comparator OECD countries (Exhibit 1). The components we estimated are all associated with higher prices, rather than being utilization effects.
Administrative Costs: About 30 Percent
We estimate that higher administrative costs associated with health insurance — for example, those related to eligibility, coding, submission, and rework — represent approximately 15 percent of excess U.S. health spending. Higher administrative burden on providers — for example, general administration, human resources, and quality reporting and accreditation — represents an additional 15 percent of the excess. This makes administrative complexity the single biggest component of excess U.S. spending estimated in this study. The large impact of administrative costs is consistent with previous research that found 39 percent of the difference between U.S. and Canadian spending on hospital and physician care was administration.3
Salary and Wages for Physicians and Nurses: About 15 Percent
OECD and international survey data show that physicians and registered nurses (RNs) in the U.S. are paid more than the average of comparator countries, with physicians earning about twice as much and RNs 1.5 times as much. These wages are determined in the context of U.S. labor markets and also may be influenced by higher levels of educational debt. Nevertheless, we estimate that higher wages for these two key health care occupations may explain a combined 15 percent of excess U.S. health spending relative to other countries.
Prescription Drugs: About 10 Percent
This estimate is based on data showing that the U.S. spends twice as much per person on retail prescription drugs, which may include differences in both utilization and price. U.S. prescription drug prices are two to three times those in other OECD countries.4 While the U.S. compares favorably on prices for unbranded generic drugs, U.S. prices are much higher for branded drugs, which account for approximately 80 percent of prescription drug expenditures in the U.S.5 Therefore, we consider this component to primarily represent a price effect.
Medical Machinery and Equipment: Less Than 5 Percent
We hypothesized that a potential driver of higher U.S. spending was higher capital costs associated with more frequent construction and modernization of facilities. However, OECD data comparing capital expenditures on health did not show the U.S. spending more for construction costs. Only in the capital investment subcategory of “medical machinery and equipment” did the data show U.S. expenditures were higher than comparator countries, corresponding to a modest impact of less than 5 percent of excess U.S. spending, approximately.
Possible Additional Excess Spending Reflected in Higher Prices
In this study, we examined several drivers of excess U.S. spending that would likely be reflected in higher prices, including: labor costs for physicians and RNs; capital costs; administrative costs; and profits.
There are other possible components of excess spending that could be reflected in higher prices that we were not able to estimate and that may be worth further exploration. These include labor costs for other workers in health care, as well as low-value care and fraud.
Labor Costs Other Than Those for Nurses and Physicians
Labor cost differences in our estimates include the impact of differences in wages for physicians and registered nurses and the impact of greater numbers of administrative staff reflected in higher provider administrative costs. We were not able to estimate differences in wages or numbers of workers for other types of health care providers, or for any of the health care support occupations and nonhealth occupations working in health care.
OECD data on total health employment indicate that the overall size of the health workforce in the U.S. is at or slightly below that of comparator countries, with the U.S. employing 64 people per 1,000 population in health, while comparator countries averaged 70 employees per 1,000 people.6 However, wages and the mix of occupations employed in health across countries may differ in ways that affect labor costs beyond what this study has captured.
Low-Value Care and Fraud
We did not estimate spending associated with two areas commonly identified as “waste” in health care — low-value clinical care and fraud. These areas are appropriate targets for health care cost reduction, but we did not find comparative data or strong evidence that low-value care and fraud are experienced more in the U.S. compared with other countries.7
Role of Health Service Use and Intensity in Higher U.S. Spending
We hypothesize that a sizable share of U.S. health spending not explained by our estimates may be because of differences in health care utilization when the definition of utilization is broadened to include the “intensity” of care (the range of services provided per visit or hospital stay), and the use of services outside hospitals and office settings. We found some evidence supporting this hypothesis, summarized below, but more robust research and analysis is required.
U.S. Patients May Receive a Greater Range of Health Services
There are several reasons why differences in service intensity may be a major factor in higher U.S. spending. First, we find evidence that patients in the U.S. receive a greater intensity of treatment per visit or hospital day, including greater access to and use of advanced diagnostic and treatment technologies, one area in which the U.S. ranks highly on supply. For example, a published analysis of OECD data shows a 44 percent higher rate of magnetic resonance imaging (MRI) exams and 62 percent higher rate of computed tomography (CT) scans in the U.S. compared with an OECD average.8 In another study, rates of coronary artery bypass graft surgery were 50 percent to 100 percent higher in the U.S. for patients with acute myocardial infarction.9
Second, we find evidence from comparative studies of well-defined procedures and patient populations that the U.S. provides more services in settings that are not as consistently tracked in the OECD data across countries, such as postacute care or specialty outpatient care, especially for high-need patients.10 In fact, the relatively low U.S. lengths of stay are consistent with a greater push to postacute and more intensive ambulatory settings.
U.S. Patients May Be Sicker Than Peers in Other Countries
In assessing potential utilization differences, it also may be useful to consider whether there is a greater underlying need for services in the U.S. We do not see evidence that the U.S. population is older on average than most peer nations. However, the U.S. population is sicker in ways that may increase the intensity of care required. OECD data indicate higher U.S. rates of obesity, diabetes, and heart disease, and a larger share of the population with multiple chronic conditions. Recent research has explored the extent to which the U.S. spends relatively less on prevention and public health and more on medical care, and the extent to which this leads to poorer population health.11
We also examined the potential impact of higher rates of assault and violence, as the U.S. is an extreme outlier in this regard. Notwithstanding the human toll, our initial estimate is that increased health care utilization resulting from higher rates of assault and violence accounts for a relatively modest 1 percent of excess U.S. spending.
Adjusting for Cost-of-Living Doesn’t Explain Spending Differences
Another piece of evidence pointing to a utilization impact on higher U.S. spending comes from analyses of international purchasing power parity (PPP) adjustments. In comparing spending by country, data are first converted to a common currency, such as U.S. dollars. The OECD health spending data used in our study were also subject to PPP adjustments that essentially adjust for differences in costs of living between countries.
In addition to the economywide PPP adjustments typically applied, the OECD has developed health care–specific PPP adjustments that reflect price comparisons of a market basket of readily comparable health care goods and services (160 drugs, 24 products, 37 hospital services, and 49 other services). Adjusting for these select health care unit price differences brings U.S. spending closer to other countries but still leaves some difference unexplained, suggesting a remaining utilization effect.12
Discussion
Some of the factors that receive a lot of attention in comparing the U.S. with other countries did turn out to be impactful, according to our estimates, with administrative costs, drug spending, and wages for physicians and nurses topping the list. Others such as higher capital costs and higher rates of violence were not associated with excess spending.
The factors we were able to estimate tended to relate to input costs and were therefore likely to be reflected in higher prices, consistent with the large body of research pointing to price differences as a major factor in high U.S. spending. Still, our estimates leave approximately half of excess U.S. spending unexplained.
Conclusion
This study is a first attempt at quantifying drivers of the difference in per capita health spending between the United States and peer nations. Most of the estimates were based on computing potential savings if the U.S. spent at the comparator country average using OECD data for the most recent year or years available. OECD data vary by year and by country in completeness and comparability, so these figures should be viewed as initial estimates. We had more success estimating components likely reflected in higher U.S. prices, which were associated with approximately half of “excess” U.S. spending.
The findings suggest that reductions in administrative burdens, drug costs, and wages for physicians and nurses have the potential to substantially reduce the difference between U.S. and peer nation health spending. A more detailed understanding of international differences in health care utilization, including intensity and modalities of care, is an important aim for future research.