Abstract
- Issue: Recent debates about reducing federal support for the Affordable Care Act’s Medicaid eligibility expansion have focused on federal spending cuts, how states might respond, and potential loss of coverage. However, the potential impact on health care providers that serve Medicaid patients has largely been overlooked.
- Goal: To assess the potential financial impact on hospitals in states that would be affected by reduced federal support for the Medicaid expansion.
- Methods: We used Urban Institute estimates of coverage losses to project the financial impact on acute-care hospitals if reduced federal spending causes states to stop covering Medicaid expansion enrollees.
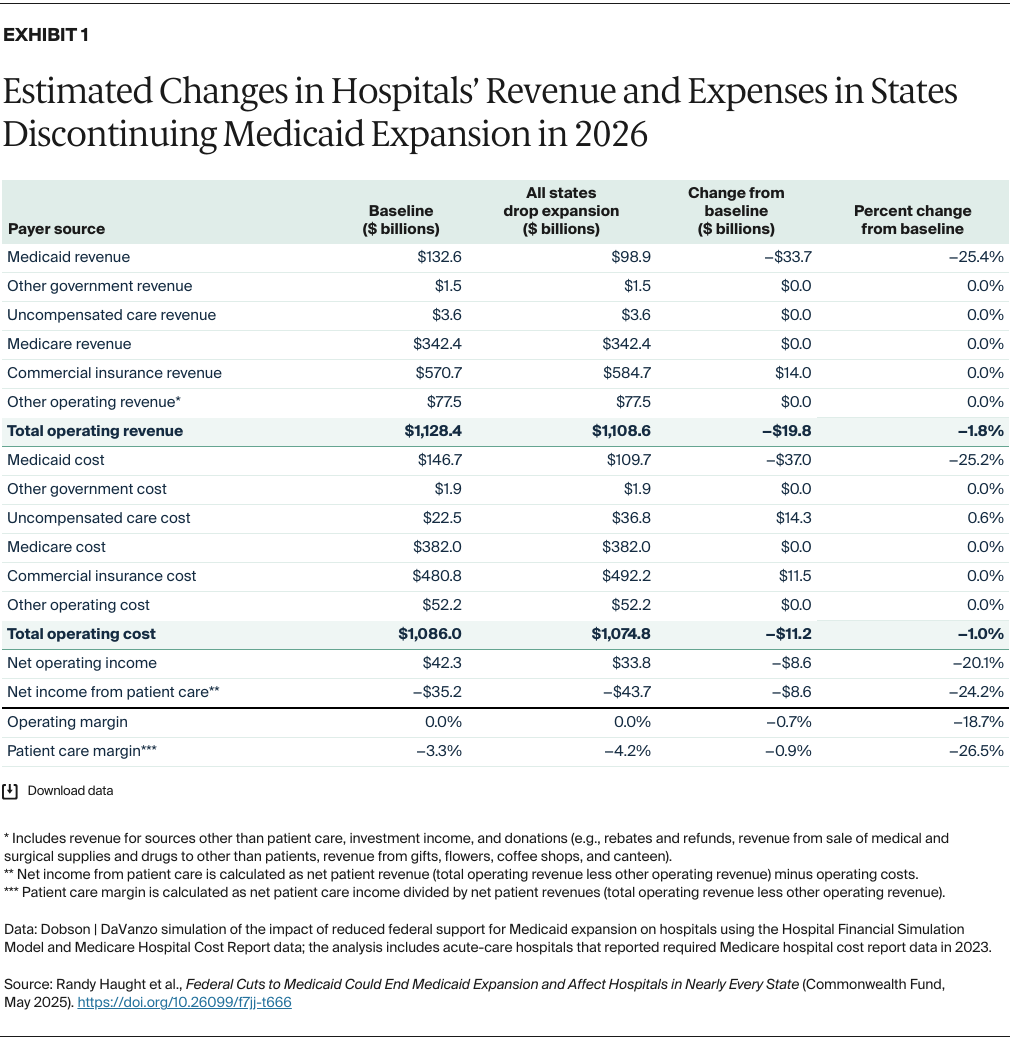
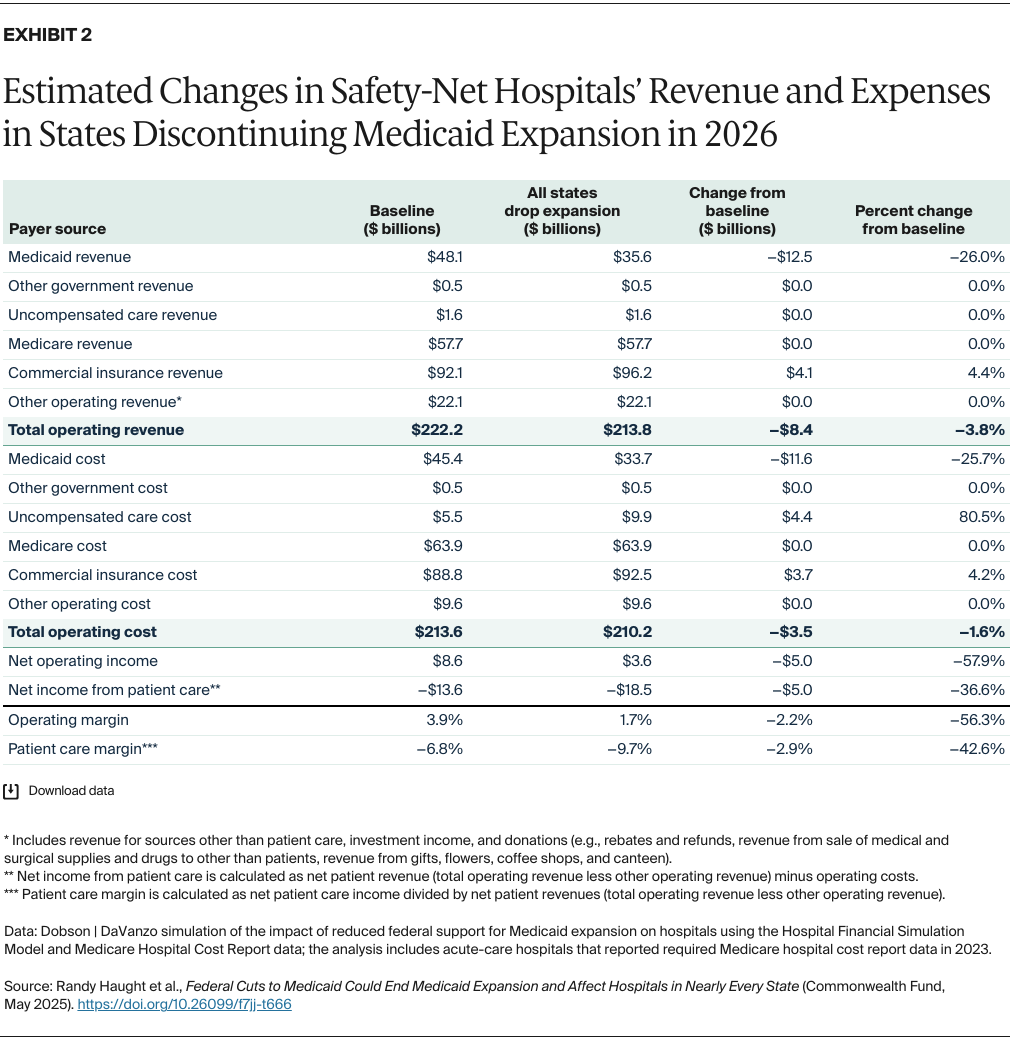
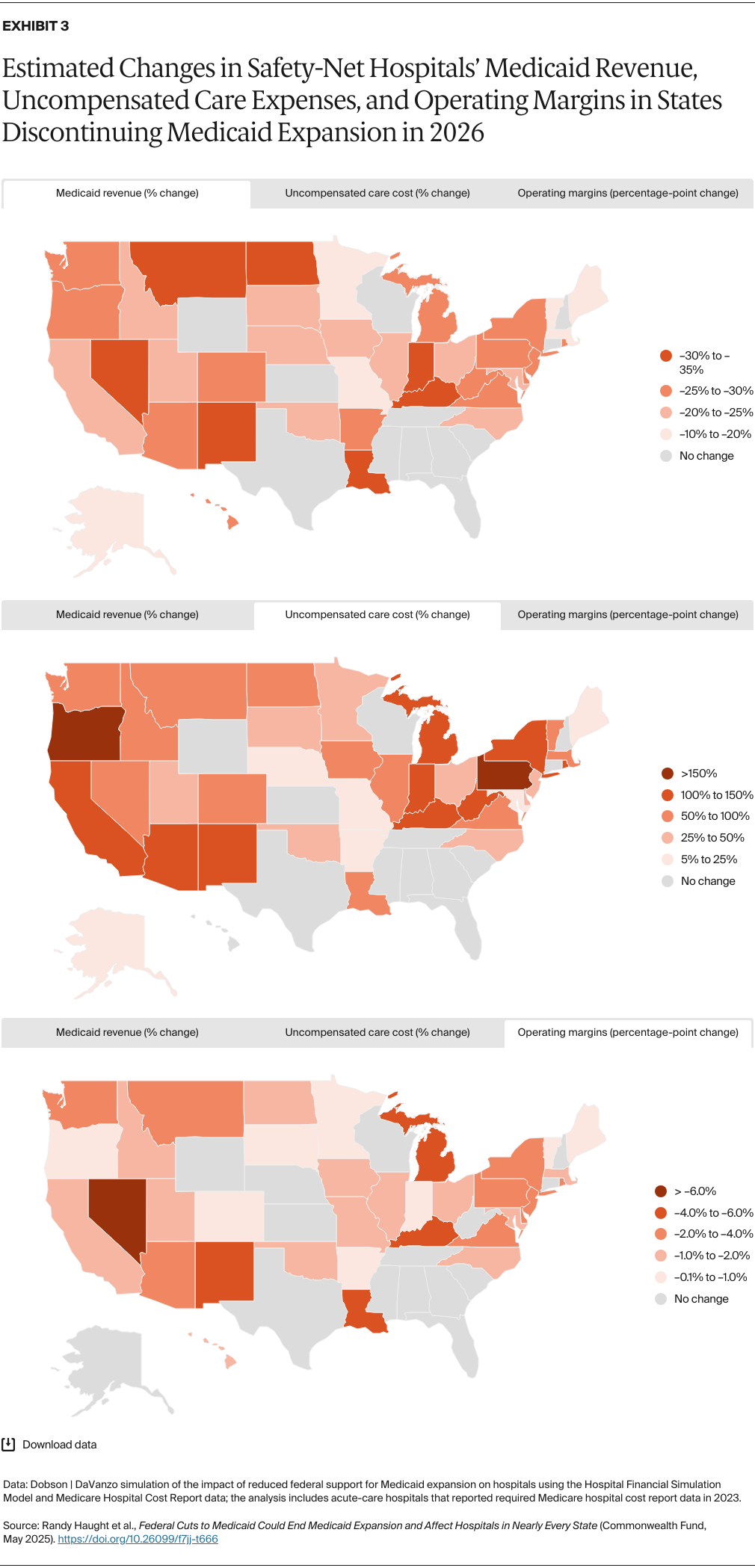
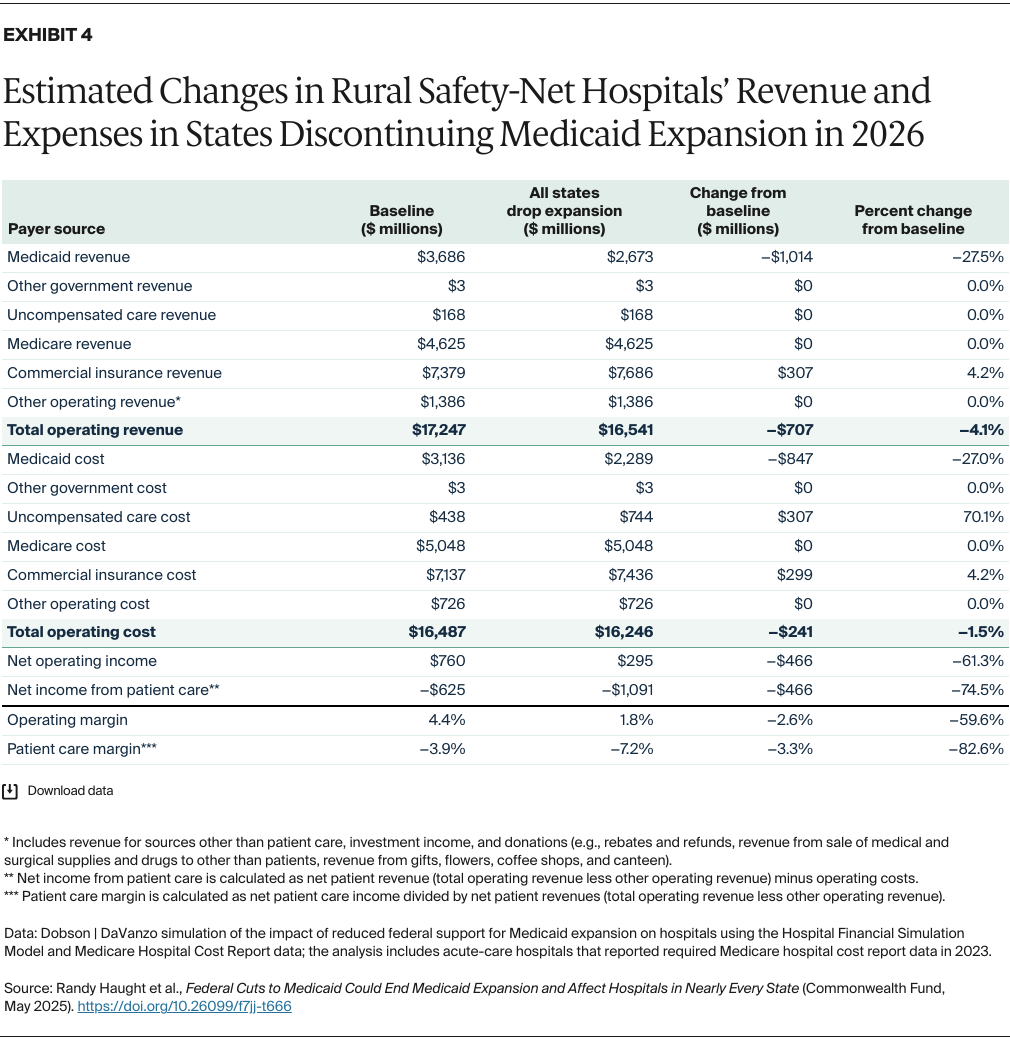
- Key Findings and Conclusion: A reduction in federal funding for Medicaid expansion — one of a number of policy changes that Congress is considering — could cause significant coverage losses. For hospitals in Medicaid expansion states, these cuts could lead to a 19 percent decline in operating margins, on average. Safety-net hospitals could be disproportionately impacted, as they treat a higher share of Medicaid and low-income patients. These facilities could see operating margins reduced by an average of 56 percent — and even more in certain states and rural areas. These adverse outcomes will affect not only Medicaid patients but also the entire community served by these hospitals, as lower revenues and increased uncompensated care could force hospitals to reduce staff or eliminate services.
Background
The U.S. Congress is considering deep cuts to federal Medicaid spending, as much as $880 billion over 10 years. According to the Congressional Budget Office, such cuts would represent a 12 percent reduction in federal Medicaid spending, totaling $7.5 trillion over that 10-year period.1
Congress is considering a number of potential policy changes to achieve these cuts. Regardless of the chosen policy, federal spending reductions of this magnitude will greatly affect state Medicaid expenditures. These in turn will impact not only Medicaid beneficiaries but entire safety-net health care systems, which serve a wide array of patients and families. One of the methods that Congress is considering is to reduce the federal Medicaid matching rate for the Affordable Care Act (ACA) expansion population to each state’s general matching rate. The share of costs paid by the federal government (the Federal Medicaid Assistance Percentage, or FMAP) for the traditional Medicaid program varies by state from 50 percent to about 77 percent in the current federal fiscal year. However, the federal government currently pays an enhanced FMAP of 90 percent for enrollees who qualify as newly eligible under the ACA’s Medicaid expansion. This enhanced FMAP has helped to incentivize 40 states and the District of Columbia to expand Medicaid eligibility to nonelderly adults with incomes up to 138 percent of the federal poverty level — totaling more than 16 million people in 2024.2