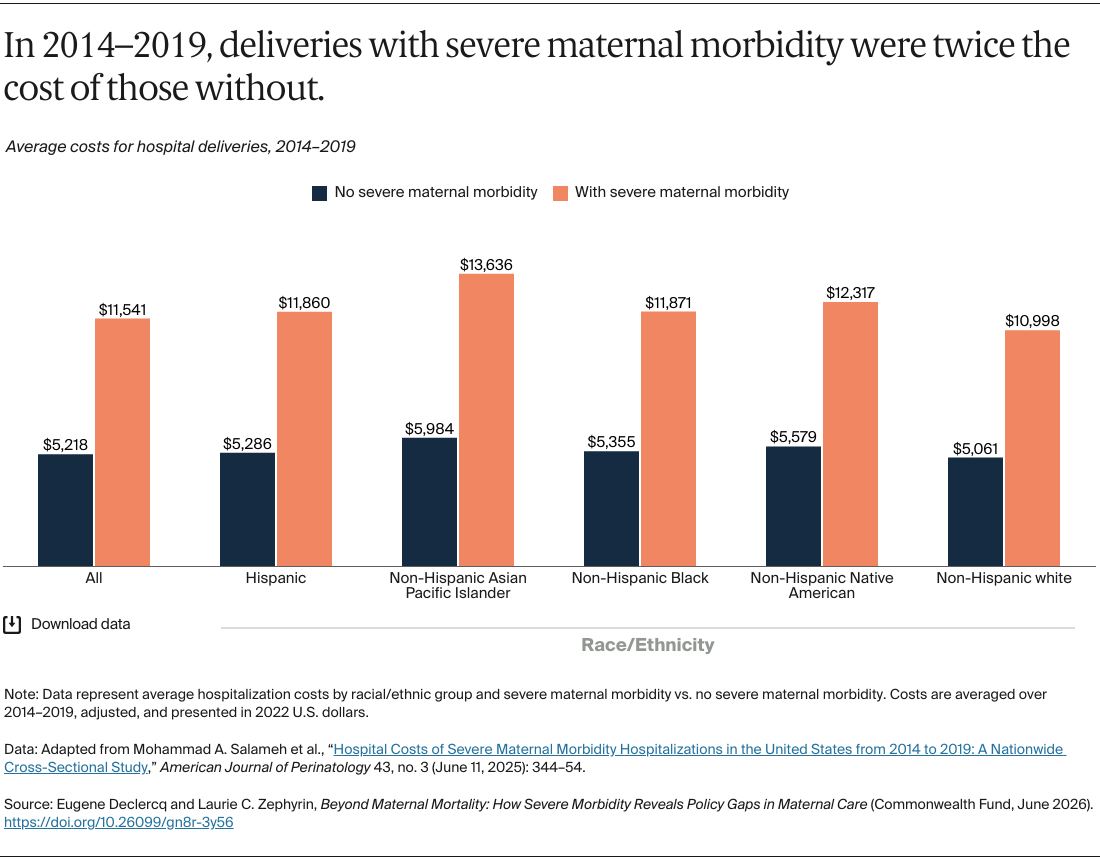
Between 2014 and 2019, births involving SMM were more than twice the cost of those births without SMM. The difference is consistent across racial and ethnic groups, but for all births to non-Hispanic Asian Pacific Islander mothers, the cost of births involving SMM rose to more than $13,600.
Discussion
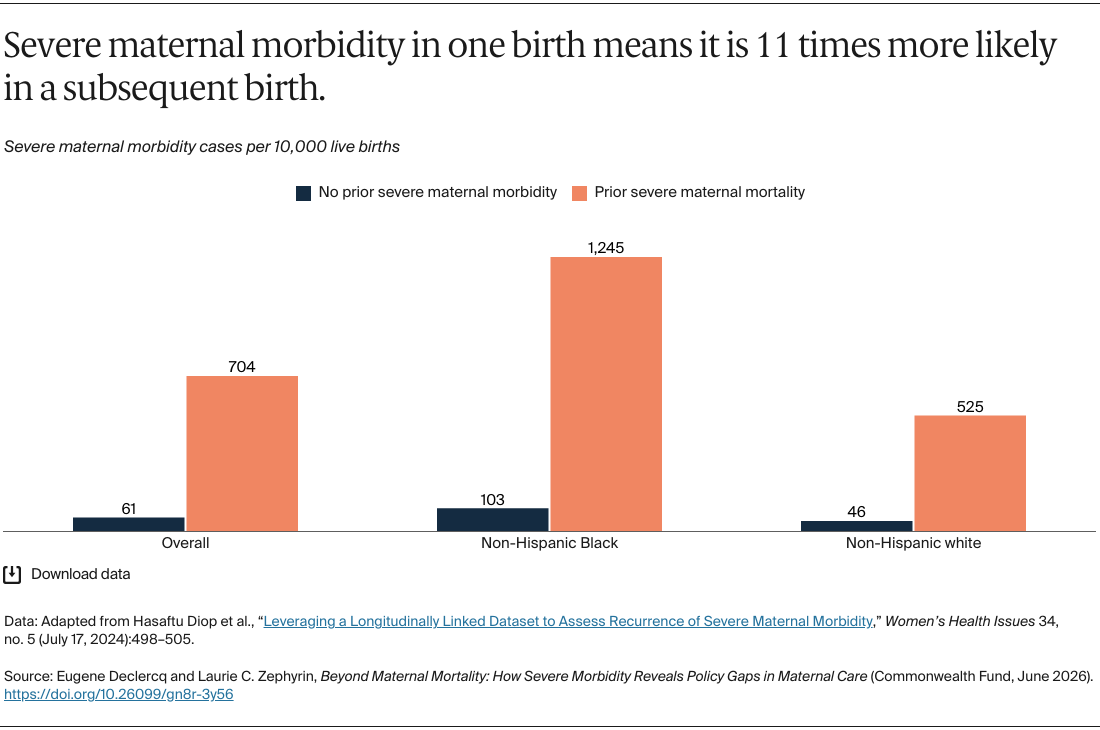
Severe maternal morbidity undermines maternal health and well-being in the United States. In addition to the up to 40,000 people a year who are impacted, SMM increases the odds of maternal death by 31 times and infant death by almost four times. These are not isolated clinical events but rather clear signals of people not getting the care that they need due to breakdowns in transitions of care, prevention, timely referral, chronic disease management, and postpartum continuity of care.
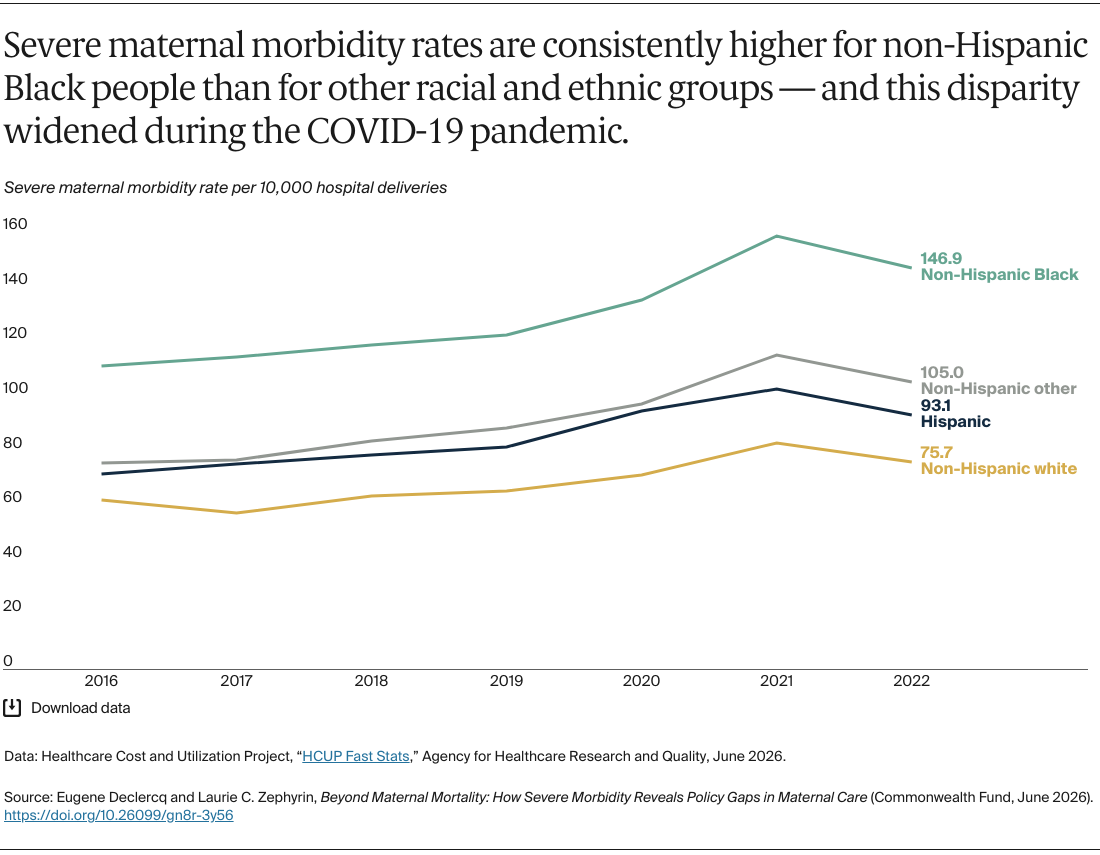
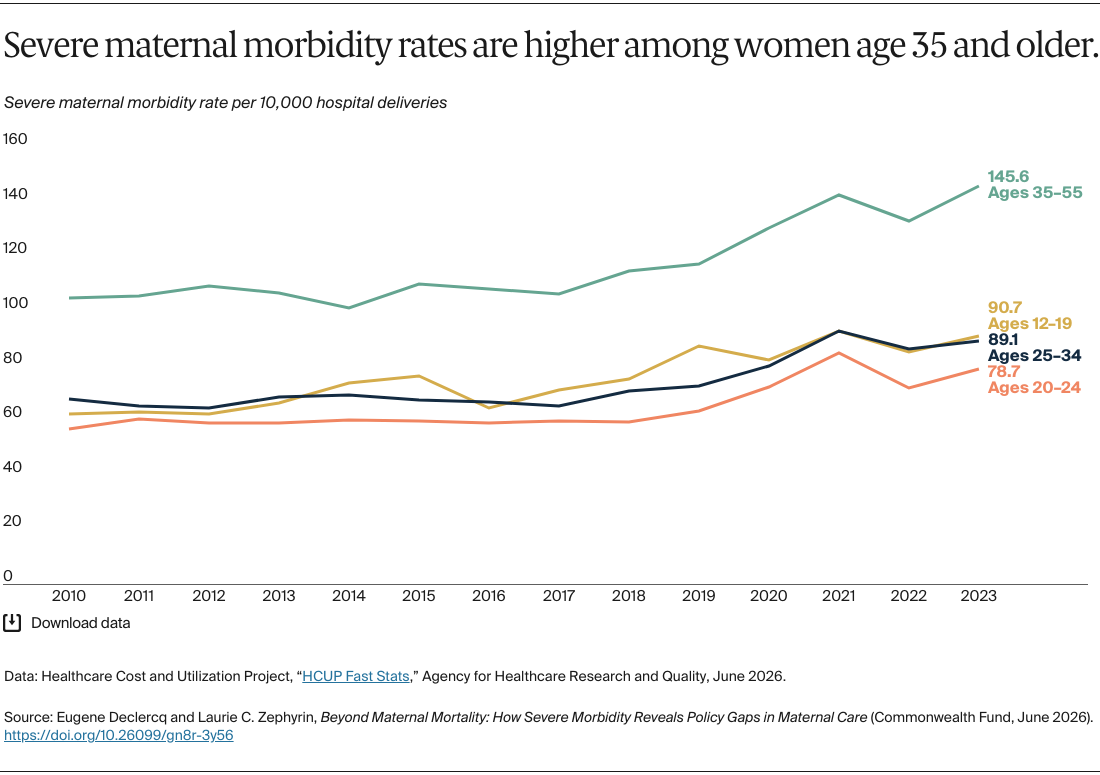
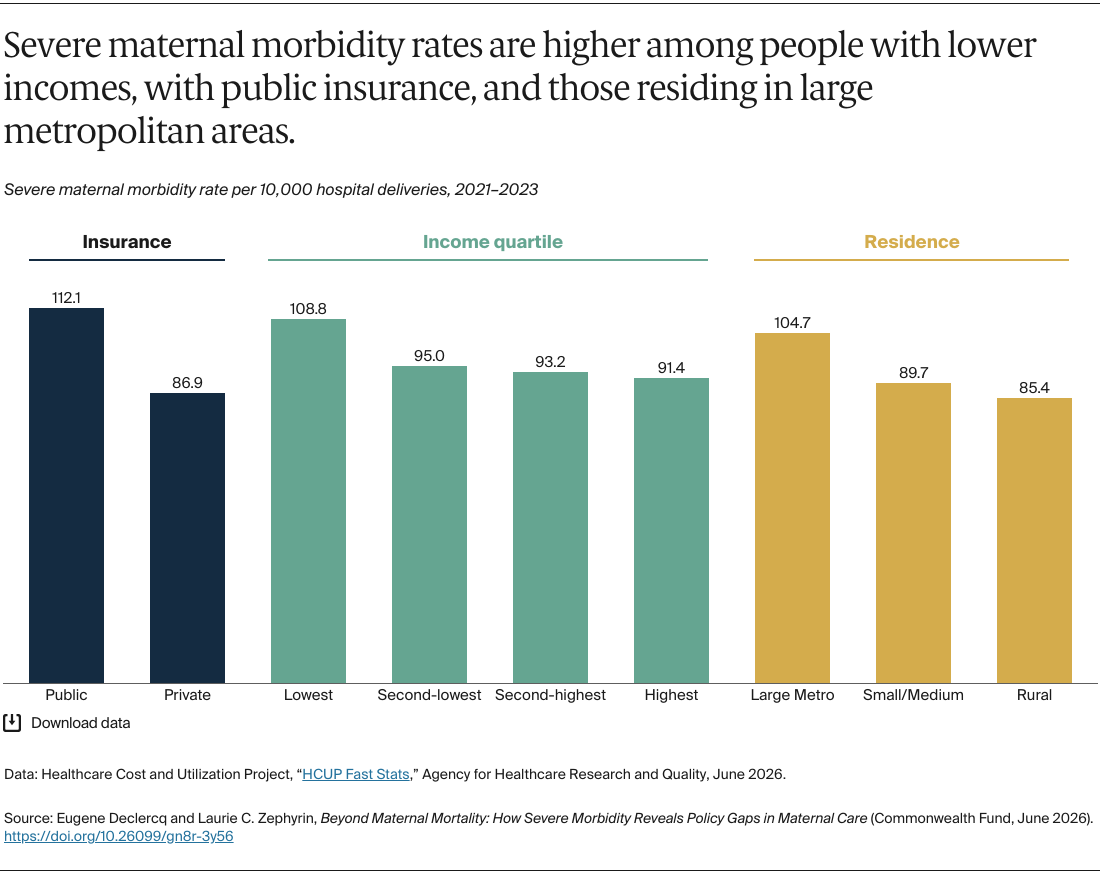
Cases of SMM are unevenly distributed, with women over age 35, non-Hispanic Black mothers, those relying on public insurance, and those in the lowest income quartile at greatest risk. Effectively tackling the problem of SMM necessitates addressing these disparities. Key steps toward lowering SMM rates in the U.S. include the following:
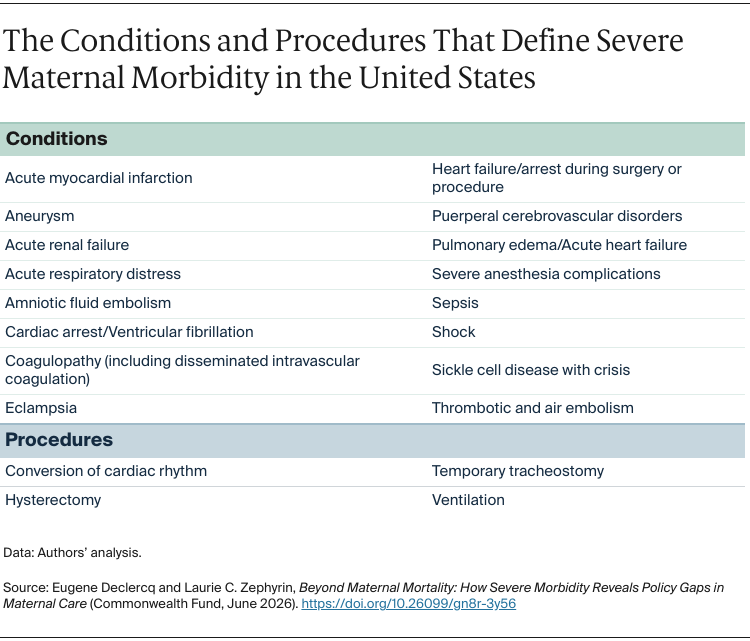
Modernizing and safeguarding maternal health data systems. Accurate measurement of severe maternal morbidity is foundational to prevention, but there are considerable challenges in doing so. The SMM algorithm applied to hospital discharge data excludes many prenatal and postpartum health and mental health conditions. While the measure has great value since it includes data on all birth hospitalizations, it misses serious morbidity that occurs outside of childbirth, undercounting conditions such as postpartum depression and anxiety, despite their well-documented impacts on maternal well-being and mortality risk.
Alongside a standard definition of SMM to improve comparability, a more comprehensive measure of SMM that includes pregnancy, one year postpartum, and mental and behavioral health indicators would improve our understanding of SMM.
Maternal Mortality Review Committees and the Pregnancy Risk Assessment Monitoring System (PRAMS) are also critical resources for understanding and tracking maternal health, but the latter is under threat due to federal funding cuts. Sustaining and improving data collection through appropriate resource allocation, including funding and expertise, is critically important.
Ensuring insurance coverage throughout pregnancy and one year postpartum. Although severe maternal morbidity is relatively rare — impacting approximately 32,505 women out of 3.6 million pregnancies each year — its consequences are profound, and many cases are preventable. Prevention is possible through robust health coverage that guarantees timely access to affordable, high-quality care. Coverage disruptions during pregnancy and postpartum impact early identification and management of serious complications. While coverage is a key part of the solution, it is the “floor” that supports additional, critical health system solutions.
Over 40 percent of births are paid for by Medicaid. Since SMM is more common among people with public insurance and low income, substantial Medicaid cuts in the July 2025 budget reconciliation bill, H.R. 1, will likely undermine health coverage and may increase SMM rates. Implementing 12-month postpartum coverage, which most states have now adopted, is key to preventing health access gaps after birth. Additionally, Medicaid managed care has an opportunity to ensure contracts provide standard postpartum care coverage.
These steps should also include improving patient transitions from obstetrics to primary care and supporting community birthing models of care. This can be done by aligning payment models to support postpartum standards, team-based perinatal care, midwifery care, doulas, and behavioral health providers. While comprehensive community-based care exists, its survival is under threat, with nearly two dozen birthing centers closing since 2023 due in part to financial pressures, including payments from insurers not covering the full cost of services.
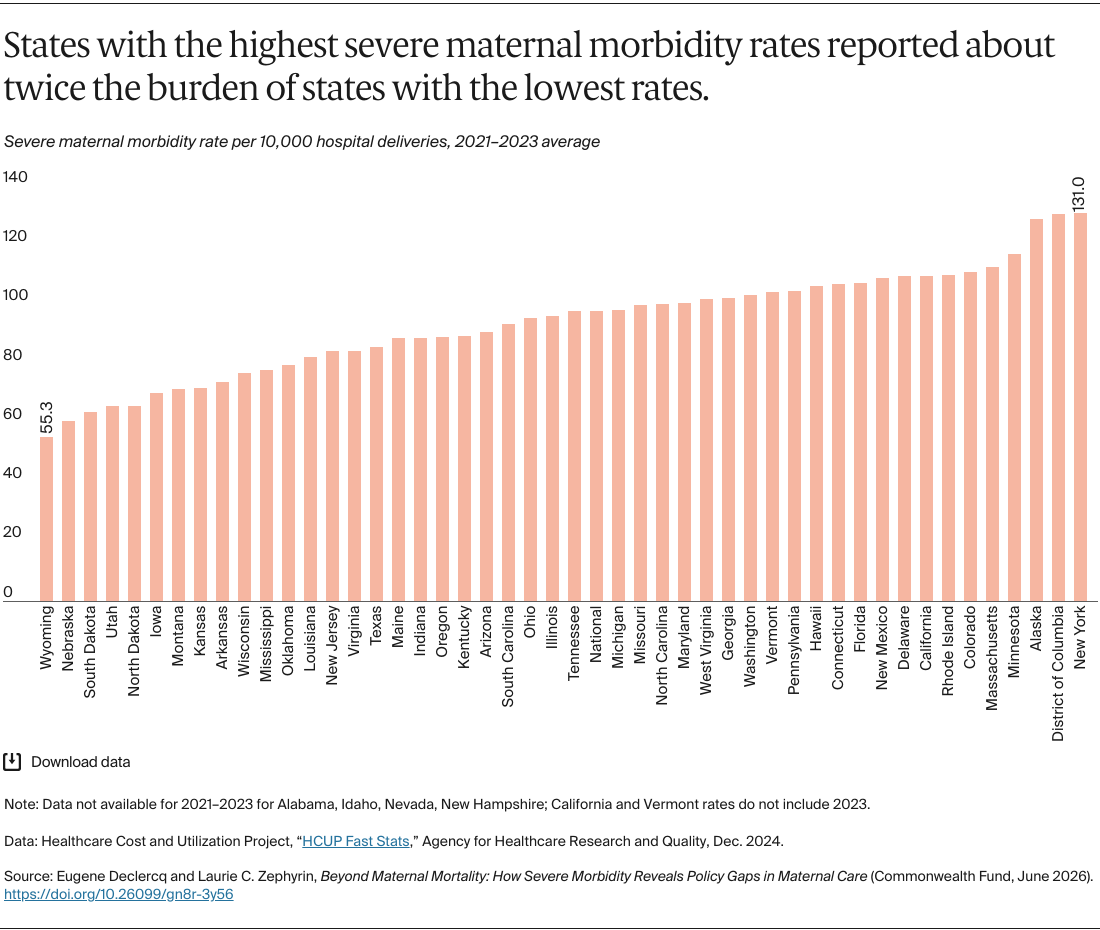
Strengthening regional care systems and referral networks. The surprising finding that states with lower maternal mortality rates tend to have higher incidence of SMM, and vice versa, merits further investigation. Whether this reflects flaws and inconsistencies in the way SMM is measured across states, or states successfully preventing maternal deaths in high-risk cases, impacts our strategies for addressing SMM.
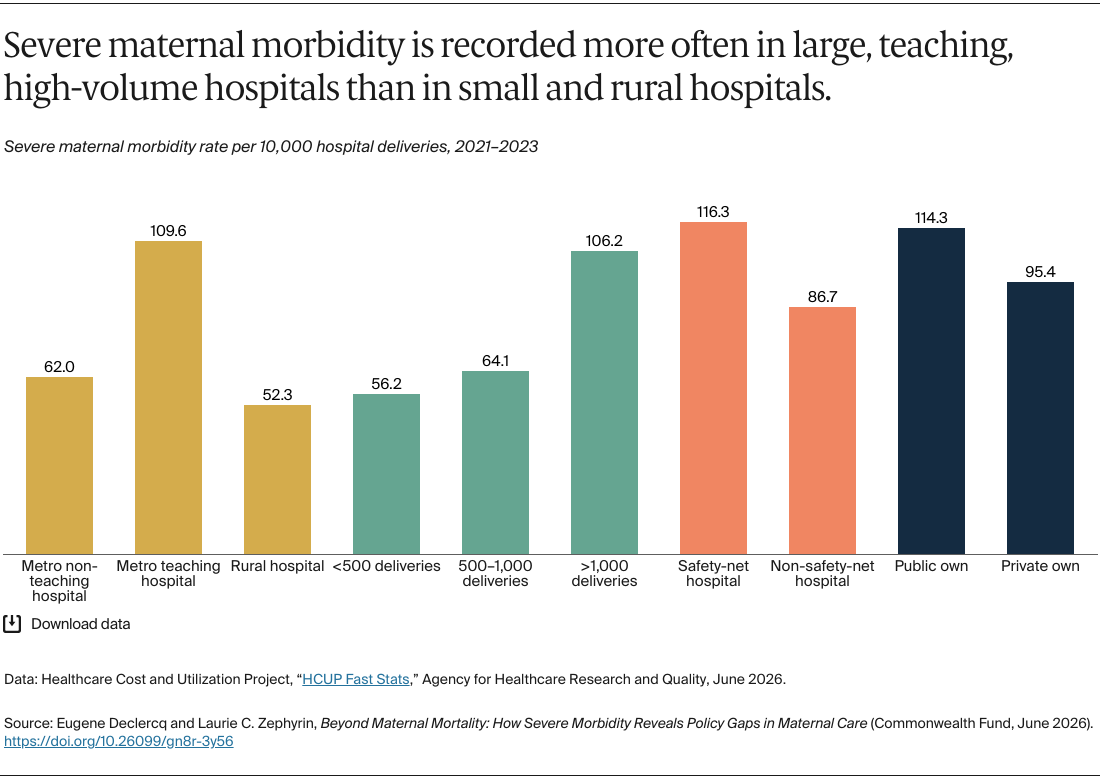
SMM is more frequently recorded in metropolitan teaching hospitals and safety-net facilities. This could be because rural and non-teaching facilities are effectively identifying high-risk patients and referring them to higher-capacity facilities, which are a critical element of SMM prevention. Prevention depends on ensuring that high-risk pregnancies are identified early and managed in facilities equipped to respond.
Efforts are underway to improve maternal health care, particularly in high-risk cases, through the continued growth of Perinatal Quality Collaboratives, which are state or multistate networks of teams focusing on improving care quality for mothers and infants. These collaboratives have prioritized reducing severe maternal morbidity, especially pregnancy complications associated with high blood pressure and hemorrhage. Additionally, there are campaigns to better identify higher-risk patients earlier in pregnancy and develop communication systems and transfer protocols to ensure they receive care at an appropriate facility.
In the future, there may be opportunities to leverage rural health funding, such as the Rural Health Transformation Program, to bolster access to maternal health services in underserved communities. Investing in telehealth and collaborative e-learning models can also create opportunities to further strengthen rural capacity and regionalization of care.
Conclusion
Addressing today’s severe maternal morbidity is essential to preventing tomorrow’s maternal and infant mortality. Doing so also improves people’s quality of life, lowers risks for future pregnancies, and reduces health care costs overall. SMM is both a critical warning sign and an opportunity — by signaling preventable harm within the health system, it offers a measurable target for quality and safety improvements.
To improve SMM rates, the health system must be designed to support people before, during, and after pregnancy with well-resourced and coordinated care facilities that are accountable for providing safe, equitable, high-quality care.