Phreesia is a health care technology company that helps ambulatory practices with the patient intake process, including registration, insurance verification, patient questionnaires, patient-reported outcomes, and payments. Data reported here come from Phreesia’s clients, which include more than 1,600 provider organizations representing more than 50,000 providers across all 50 states. In a typical year, these provider organizations have more than 50 million outpatient visits, or more than 1 million visits a week.
The provider organizations include independent single-provider practices, multispecialty groups, federally qualified health centers, and large health systems. Of all visits in a typical week before the pandemic, 47 percent are with primary care physicians (adult and pediatric) and the other 54 percent of visits are spread across more than 25 specialties. Visits with nurse practitioners and physician assistants are included under these 25 other specialties.
Data come from several sources at the organizations: 1) practice management/scheduling software; 2) check-in information submitted via patients on the Phreesia platform (e.g., reported age); and 3) selected data from the electronic health record, such as problem lists.
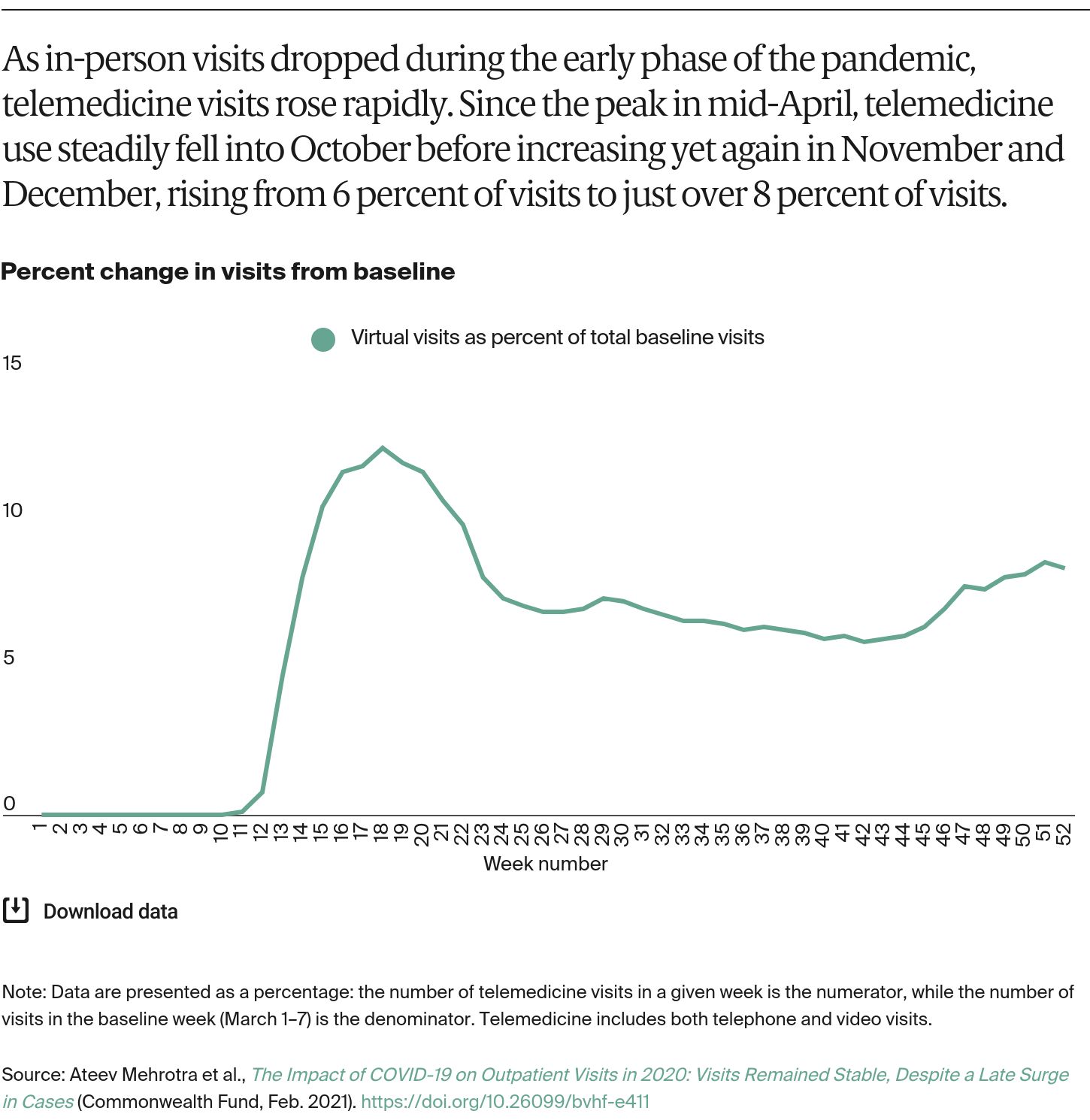
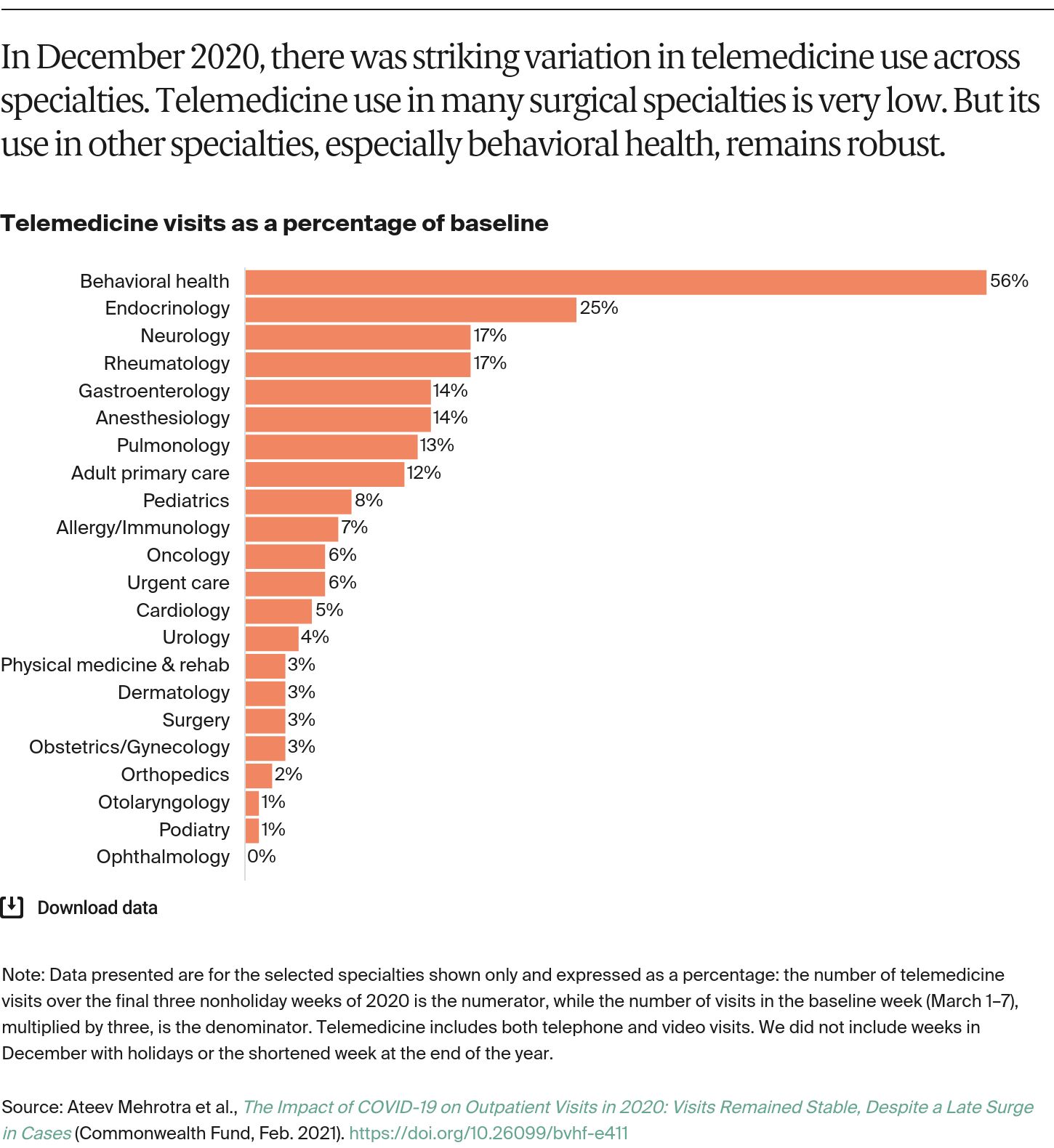
Visits were captured from January 1, 2016, to December 31, 2020. A visit was counted if it was in the practice’s scheduling software and the patient was checked in. A visit is considered checked in when either the patient or someone at the practice (such as a nursing assistant) filled in the necessary information using the Phreesia platform and the patient was ready to see the provider. Telemedicine visits were identified in the scheduling software based on the appointment type or location. Telemedicine includes both telephone and video visits.
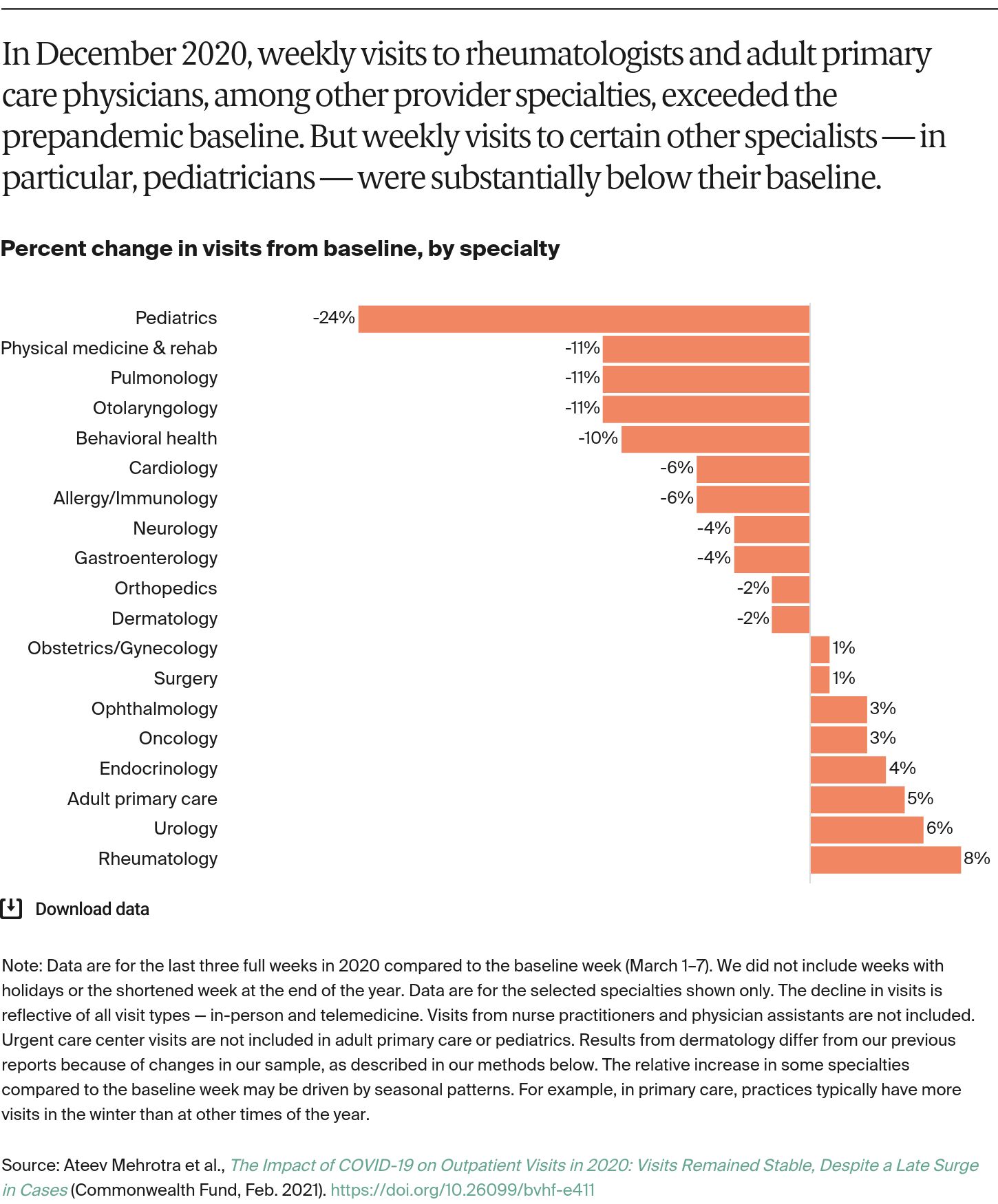
We made several modest changes in this most recent report. We included all Phreesia clients that were part of the data as of January 1 of a given year. New Phreesia clients that joined after January 1 were not included in the data for that year. During the year, existing clients may introduce Phreesia to new clinical sites. For example, an organization might buy a new practice site or begin to use Phreesia services at existing clinical sites that had not been previously counted in our data. To avoid bias in our estimates of changes of visit patterns, we excluded organizations that displayed very high levels of such expansion. This change had a very small impact on our overall visit counts, but readers will note that this change did have a substantive change in dermatology results from our October 2020 report.
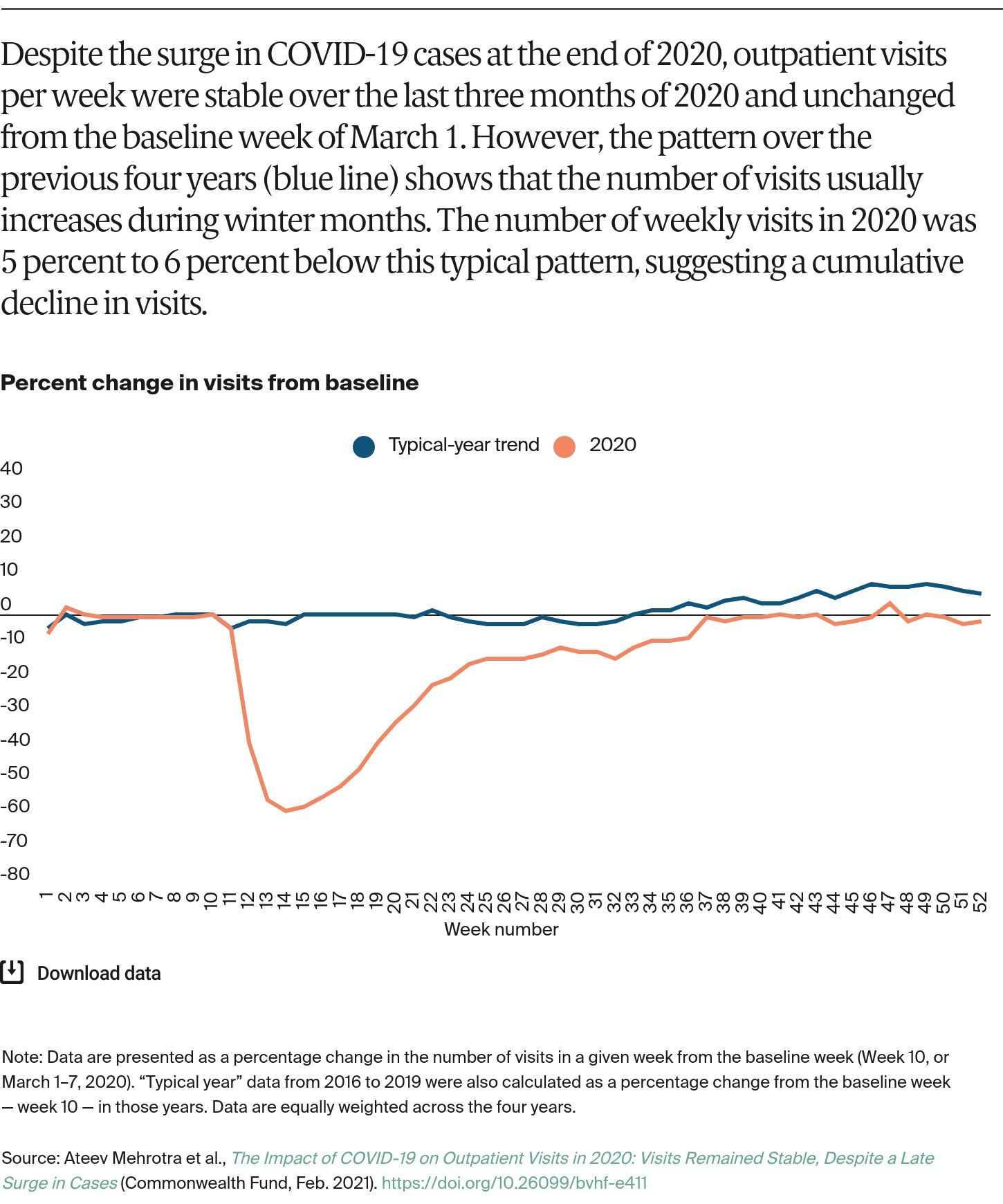
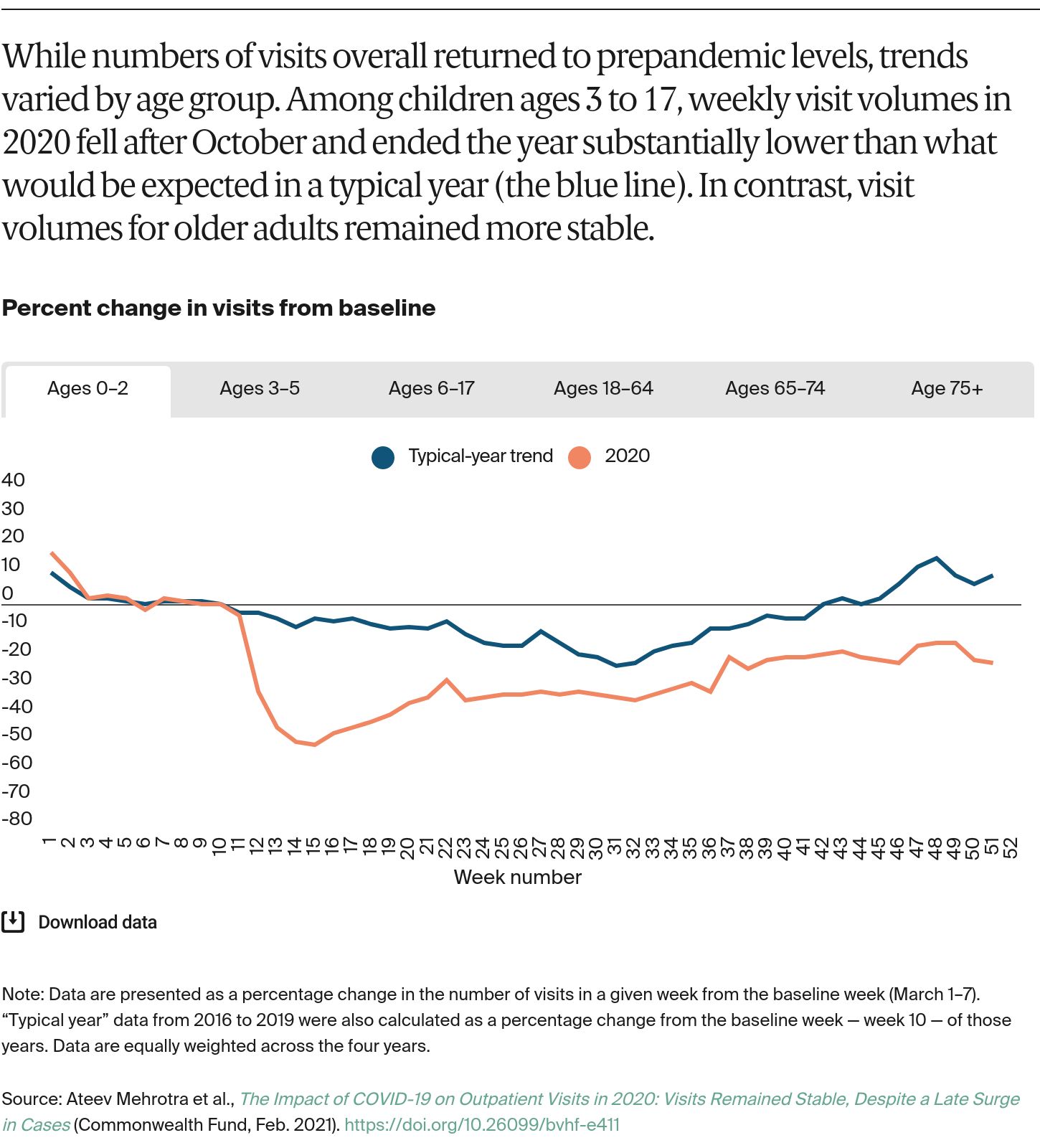
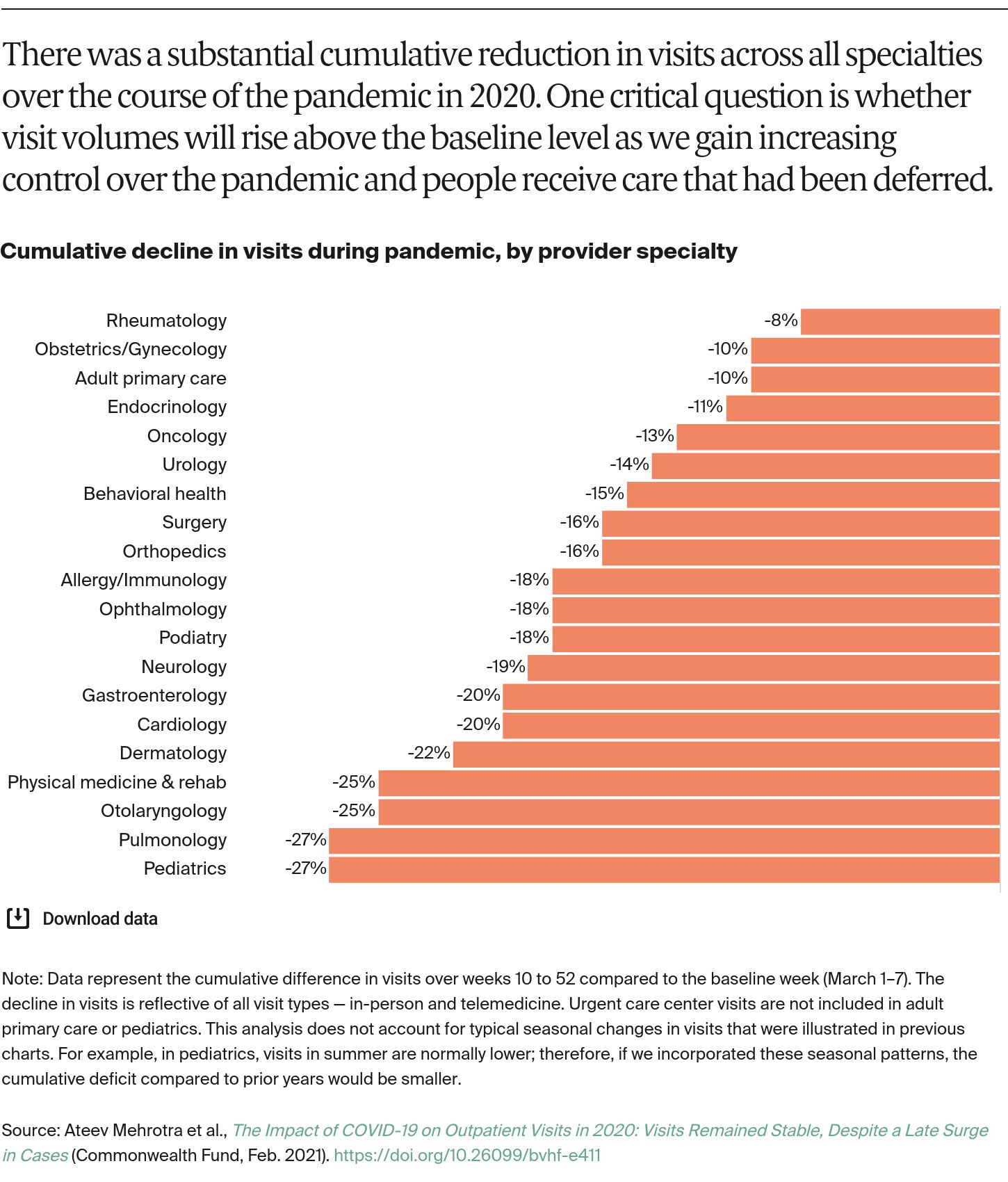
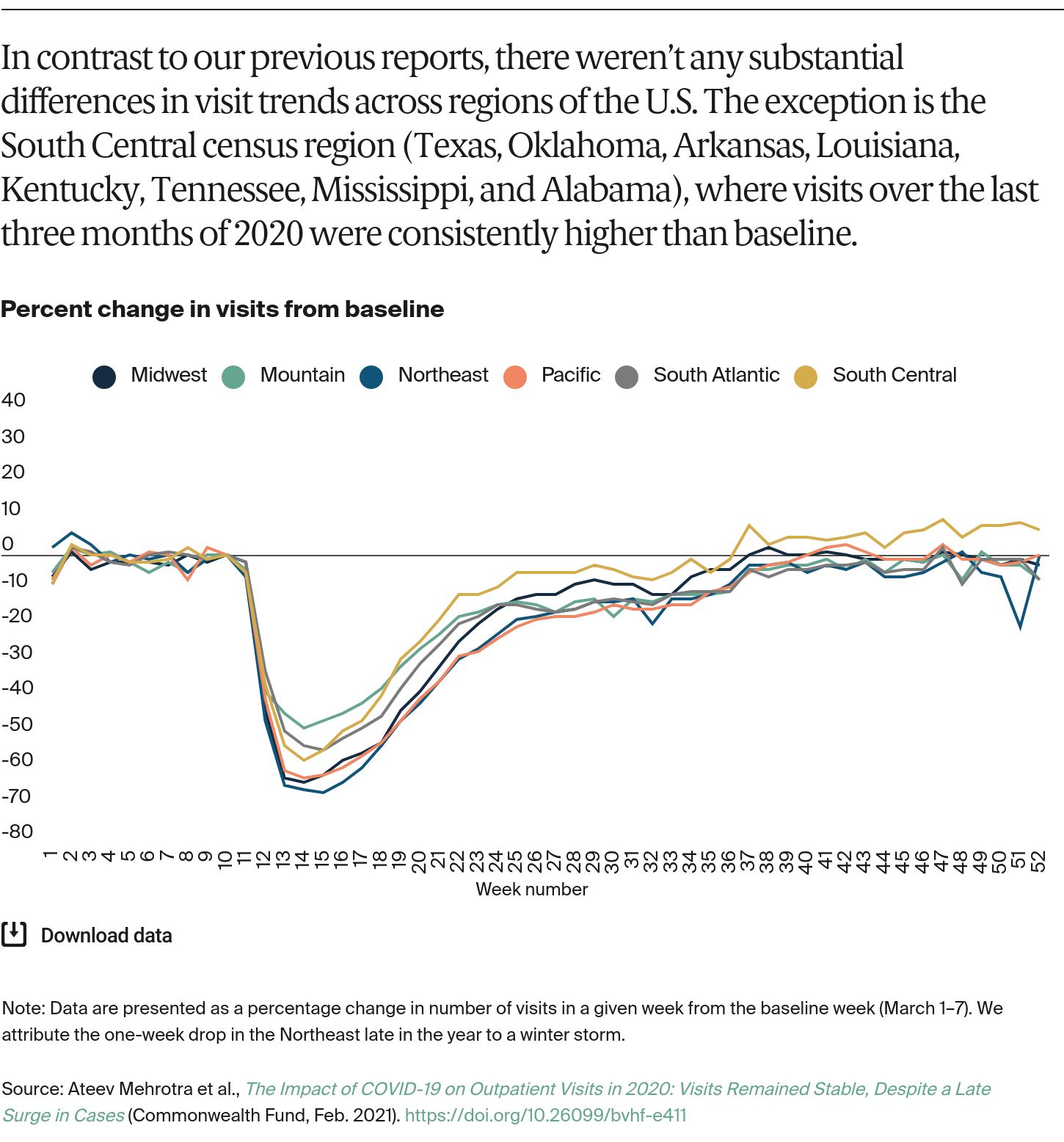
Phreesia staff, in consultation with Harvard University researchers, analyzed all data. They calculated results and shared them with the researchers in aggregate form as percentage drops from baseline. The baseline for visits was defined as the week of March 1 to 7 — a representative week among the organizations prior to effects of the pandemic. Visits on holidays were excluded, and, during holiday weeks, we adjusted visit counts to account for the fewer days during the week.
The data have limitations. As with any convenience sample of providers, the patterns we observe may not be representative of all organizations nationally or regionally. While we have tried to address situations in which organizations added or dropped practice sites, changes in the organizations (e.g., expansion of providers at a single site) could be driving some of the results described. Unscheduled same-day and walk-in visits are typically captured in the scheduling software, but it is possible some unscheduled telephone encounters were not captured if the software did not record them. Workflow and documentation practices have likely shifted during the pandemic as well. Finally, the fraction of all visits identified as telemedicine may be underestimated, since, early in the pandemic, providers were still creating processes to designate telemedicine visit types in their scheduling software.