
Introduction
Soon after completing their prison sentences for drug violations, Diane R. and Melissa H. moved into a rundown apartment in an old Massachusetts manufacturing town. There, they went back to using heroin, despite life-threatening illnesses—end-stage liver disease for Diane and HIV for Melissa. Because both women were dually eligible for Medicare and Medicaid benefits, they were able to enroll in an experimental program that allows health insurance plans to combine the capitated payments they receive from both programs to pay for a wider array of services, including substance abuse treatment. The goal of the program, called One Care: MassHealth plus Medicare, is to see whether providing comprehensive, well-coordinated care can improve outcomes and lower costs for patients like Diane and Michelle who have complex needs.
One Care: MassHealth plus Medicare
Commonwealth Care Alliance (CCA), the Boston-based Medicare Advantage plan and care delivery network to which Diane and Melissa were assigned, is a participant in the One Care demonstration. CCA has had more than a decade of experience providing integrated care to “dual eligibles” age 65 and older as part of the Massachusetts’ Senior Care Options (SCO) program. (The older members are part of CCA’s Special Needs Plan, while dual eligibles under age 65 are enrolled in a Medicare–Medicaid Plan.)
The One Care program, a partnership of Massachusetts’ Medicaid agency and the Centers for Medicare and Medicaid Services, is the first demonstration to focus exclusively on “dual eligibles” under age 65—a vulnerable group with a variety of often overlooked care needs. Participating health plans receive capitated Medicare and Medicaid payments, which are used to provide enrollees with the medical, behavioral health, dental care, and long-term services and supports they require. Plans must also work with community-based organizations and external coordinators for long-term services and supports.
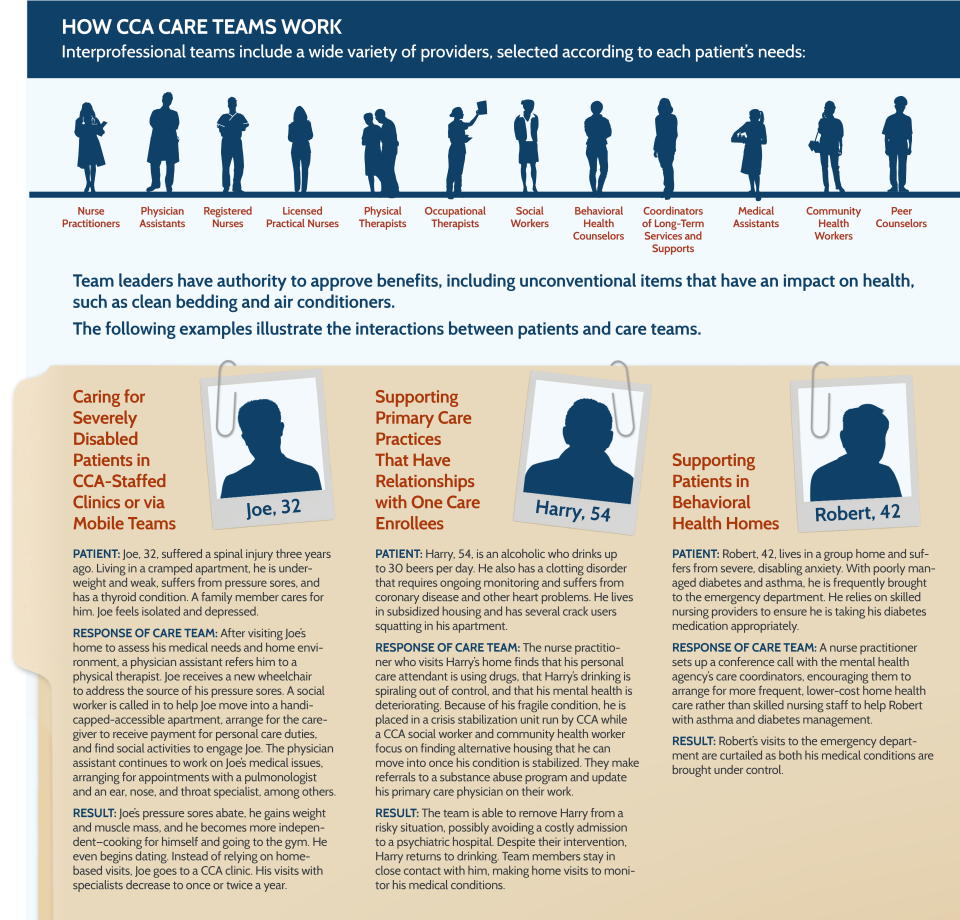
At the core of CCA’s One Care model are interprofessional care teams comprising nurse practitioners, physician assistants, social workers, community health workers, and other professionals. These teams work with complex patients to identify their unmet medical, behavioral health, and social service needs and then deploy resources as needed, using the flexible benefits that team members have authority to approve. When this approach was tried with elderly patients, it led to significant declines in nursing home admissions and a drop in hospital admissions.1
The nonelderly patients CCA seeks to help through One Care are more challenging to connect with and care for, making similar reductions in utilization harder to achieve. This is one of the reasons CCA’s efforts are being closely watched by policymakers and other health care organizations. “I think everybody is hoping that CCA, using the model that has been developed, [can] actually do the work of bringing it to scale,” says Jeff Scavron, M.D., a CCA board member and a physician at a nonprofit community health center that participates in the program.
Commonwealth Care Alliance's Target Population
Under the One Care demonstration, CCA provides coverage to 11,134 dual eligibles under age 65 in Massachusetts—81 percent of the state’s residents who have opted to participate or been automatically enrolled in the program.2,3 Roughly 80 percent of CCA’s One Care members have multiple chronic health conditions, behavioral health problems, or functional limitations because of physical and developmental disabilities. Some have been rendered virtually homebound from muscular dystrophy or cerebral palsy. Some are homeless or cycling in and out of correctional facilities as a result of severe mental illness or substance abuse. Still others struggle in poverty to cope with multiple chronic conditions.
Commonwealth Care Alliance’s One Care Enrollees
- 81% have two or more chronic conditions
- 80% have serious mental illnesses, such as schizophrenia, bipolar disorder, or severe depression, and/or substance abuse problems
Source: Commonwealth Care Alliance.
Approximately 30 percent of CCA’s One Care enrollees account for 70 percent of expenses. Among these high-risk enrollees are patients with serious mental illnesses or substance abuse problems; people with four or more chronic illnesses, including life-threatening ones such as HIV, heart failure, or chronic obstructive pulmonary disease; and homebound individuals with catastrophic conditions like Lou Gehrig’s disease or quadriplegia that require long-term services and supports.
Key Program Features
Interdisciplinary Care Delivered Where Patients Need It
Many of CCA’s One Care members have difficulty establishing and maintaining relationships with primary care providers. Those with physical and cognitive disabilities, for instance, often struggle to make and keep appointments with the multiple specialists they require, while those with serious mental illnesses and substance abuse problems may not seek care at all (according to CCA staff, no-show rates for primary care and psychiatry appointments in this population are as high as 60 percent to 70 percent). Rather than asking these patients to adapt to the existing health care system, CCA assembles care teams around them. The teams go where they are needed—to patients’ homes, primary care practices, and community settings—to identify gaps in care and increase access to services.
In the case of Diane and Melissa, a CCA nurse practitioner visited their home and quickly arranged for palliative care and skilled nursing services when she realized Diane was nearing the end of her life. Not long after, Diane suffered a stroke. Following a short hospitalization, however, she was able to return home, where she preferred to spend her remaining days.
In the months after, Melissa relapsed. The team was able to arrange for substance abuse treatment for her under Care One’s expanded benefit. When Melissa reported chest pains, they also arranged for her to see a specialist, who discovered occlusion in a coronary artery. “There aren’t a whole lot of patients like this who are that acute, but the few who are require very, very intensive intervention,” says Laura Black, N.P., a clinical director at CCA.
Some of the teams provide direct care within four CCA-run primary care practices, which offer home- and clinic-based care to members with the most significant physical, behavioral health, and social needs. For patients who have well-established relationships with community-based primary care practices, the teams play a more limited role, helping to build bridges between primary care providers, specialists, and the hospitals, nursing homes, and skilled nursing facilities that serve One Care patients. Other teams may partner with mental health agencies, which are the primary source of care for patients with behavioral health problems, as well as other human service agencies. These agencies are delegated by CCA to provide case management services, including coordination of physical and behavioral health care, with training from CCA’s care team members.
“Our goal is to identify where strong relationships exist between members and providers and to reinforce rather than supplant them,” says Toyin Ajayi, M.D., CCA’s chief medical officer.
Shoring Up Behavioral Health Services
Soon after enrolling patients, CCA found a high prevalence of behavioral health problems in new members and significant gaps in the availability of outpatient services to meet their needs. This led to high rates of hospitalization and emergency department use.
In some locations, outpatient providers have been unwilling to see One Care enrollees or have set visit limits, says Peggy Johnson, M.D., CCA’s chief of psychiatry. CCA also has had difficulty finding facilities that can provide detox or step-down services to support sobriety. To address these gaps, CCA has created two crisis stabilization units (CSUs) that provide short-term acute psychiatric care, including detox services. They also have partnered with Bay Cove Health Services, a nonprofit social service agency, to provide treatment and care transition services. The average length of stay in the units is 10 days, during which staff assess patients’ medical, behavioral health, and social support needs and establish or reestablish patients’ connections to primary care providers.4
One of the CSUs, Marie’s Place, a home in Brighton, Massachusetts, accommodates up to 14 patients who are experiencing crises but do not need to be hospitalized in locked wards. Marie’s Place shares many features of inpatient units, such as an on-duty psychiatric nurse practitioner; licensed clinicians, such as a social worker to run support groups; and mental health counselors, who assess patients’ needs on site. Psychiatrists are also available for consultation and support. CCA has established a second 12-bed CSU, The Carney, by leasing space at a community hospital. Care in the CSUs averages $630 per day compared with $1,100 per day for inpatient stays.5
Coordination of Long-Term Services and Supports
As part of the demonstration, One Care enrollees have the option of getting help from a long-term services and supports coordinator from a community organization, such as the Boston Center for Independent Living. The coordinators serve as advocates for enrollees, help identify needed services and resources, and help develop and monitor the care plan. “They are real assets to our team,” Ajayi says.
Financing
To provide comprehensive care for roughly 10,000 One Care enrollees, CCA received $385.7 million from Medicaid and Medicare in 2015 and $256.9 million for the 15 months ending December 2014.6 The state’s Medicaid contribution ranges from roughly $120 per member per month for relatively healthy patients to $9,000 or more for patients with extended stays at long-term care facilities (see Appendix A).7 The base rate for Medicare Part A/B capitation payments ranges from $770 to $960 per member per month.8 On average, per member per month spending amounted to $2,641 in 2015 and $2,205 in the 15 months prior.9
Results
A study of 4,500 of CCA’s One Care enrollees found that, after 12 months of enrollment, they had 7.5 percent fewer hospital admissions and 6.4 percent fewer emergency department visits than in the 12 months prior to enrollment. They also made greater use of long-term services and supports. The majority (82%) of enrollees said they were satisfied with the program.10 A preliminary analysis also found that the crisis stabilization units, in particular, contributed to lower admissions.11 The early findings may change as enrollees gain more experience with the program.
Meeting the needs of patients with substance abuse disorder, building out and enhancing provider networks, managing care transitions—all of this requires intensive upfront capital investment, which states need to be aware of and support.
Despite these improvements, CCA lost $34.9 million on revenue of $256.9 million in the first 15 months of the program, a loss that was reduced to $18.4 million by a risk corridor program intended to mitigate insurers’ extreme gains or losses. The health plan came close to breaking even for 2015, with a projected loss of $416,000 on revenue of $385.7 million, and expects to achieve savings in 2017.12,13
CCA leaders say the risk-adjustment techniques initially used by both Medicaid and Medicare to set capitated payment levels were a factor in the early loss because they vastly underestimated the number of enrollees with behavioral health needs and the scope of their problems. For example, some patients with schizophrenia were deemed average risks by Medicare. Moreover, many enrollees had been underserved in the fee-for-service system, creating pent-up demand for medical care, behavioral health services, and social supports, says Christopher Palmieri, CCA’s CEO and president.
This was a problem for all the plans participating in the One Care program, says Daniel Tsai, assistant secretary for MassHealth and the state’s Medicaid director. “We saw folks who we thought were one level of need but once they got on to a One Care plan, including Commonwealth Care Alliance, and had an actual assessment, they turned out to be much more complex,” he says.
Member assessments, combined with better documentation and more accurate coding, enabled CCA to reclassify roughly 25 percent of its One Care enrollees into higher-risk categories. The Centers for Medicare and Medicaid Services (CMS) and MassHealth also increased reimbursement rates and made modifications to risk-sharing agreements that resulted in CMS and MassHealth assuming greater responsibility for losses.14
Insights and Lessons Learned
With underserved populations, better care coordination may lead to higher spending in the short run. It is often assumed the fee-for-service payment leads to greater use of services while capitation models encourage providers to do less. But for dual eligibles who have been poorly served by traditional delivery models, better coordination and oversight often lead to the discovery of unmet needs and potentially greater use of services following enrollment in comprehensive care programs such as One Care, as Melissa’s case revealed. CCA found spending on newly enrolled members was higher than expected initially; it took about 18 to 20 months to return to historical levels as the plan optimized their care. These higher initial costs may be offset in the long run by the savings from more judicious use of long-term services and supports, the avoidance of high-cost institutional care (including inpatient psychiatric facilities), and better management of chronic disease and care transitions. However, these take time and money to achieve.
“This requires intensive upfront capital investment, which states need to be aware of and support,”Ajayi says. “Expecting savings in the very beginning and baking in rate reductions clearly is problematic.”
Patient assessments help ensure that plans have the resources they need but can be difficult to execute. Incomplete data about enrollees’ clinical problems and social challenges makes risk adjustment and rating difficult. While assessments can help, CCA found they are a challenge to complete because of members’ transitory lives. “Telephone contacts are virtually futile,” reaching only 20 percent, Black says, and going directly to enrollees’ homes isn’t as fruitful as one would expect. “The addresses are wrong more often than not. And when you do find someone, there’s a lot of historic distrust.”
In addition to in-person outreach, CCA staff look at pharmacy claims to locate current home addresses should they need them later. These claims also yield the names of their providers, which can be useful for improving care coordination or communication with patients’ providers and for outreach.
CCA staff also locate individuals by sending teams to meet patients in the hospital when their admissions are flagged in the electronic health record system. In other cases, they ask the health plan’s member services department to refer enrollees to care management services when they are looking for help with transportation or other supports.
Active enrollment facilitates patient engagement but may be slower to scale. In the early months of the program, roughly half of CCA’s One Care members were automatically enrolled in the program but allowed to opt out (passive enrollment), while the other half opted in (active enrollment). Both approaches have trade-offs: automatic enrollment allows the state to recruit a sizeable number of patients, but many can be difficult to locate, assess, and treat—putting the plans at financial risk for enrollees they could not find.15 In contrast, enrollees who actively choose to enroll in the program are easier to locate and more accepting of the model and its care coordination component. But this method requires significant outreach, which can slow program implementation.16
Partnering with advocacy groups helps to engage patients. CCA works closely with organizations that enrollees already trust, not only to refine its care model but also to help publicize the program and its benefits. Tsai says such partnerships have been useful in countering resistance to the program from some providers of long-term services and supports who feared a more integrated approach would reduce demand for their services.
Next Steps
Going forward, Commonwealth Care Alliance continues to look for cost-effective ways to improve outcomes for enrollees and reduce service gaps. It has engaged local pharmacists to provide medication management services for One Care enrollees and has created a pilot program to leverage the skills of community-based paramedics to reduce emergency department use. The pilot was sparked by a review that found more than half of emergency department visits of CCA members could have been managed at home or another care setting.
As part of the pilot, paramedics employed by a local ambulance company are dispatched to patients’ homes between 6 p.m. and 2 a.m. to provide urgent care, including intravenous therapy, antibiotic administration, and lab tests.17 The paramedics have access to patients’ electronic medical records and confer with CCA’s doctors and nurses by phone. “Patients, particularly those who have a behavioral health diagnosis, love it. They feel they are seen more quickly and they don’t feel anxious and disempowered as they do in the emergency department, where people don’t know their medical history,” Ajayi says. According to member reports, in 85 percent of cases the visit from a paramedic averted an emergency department visit.
Meanwhile, Massachusetts is looking to expand the One Care program. As of June 2016, state officials had enrolled roughly 13 percent of eligible residents, and they expect to enroll more now that risk-adjustment problems have been resolved. The state also has extended the demonstration through 2018. “It’s good policy, it’s good care, [and] it’s good coordination,” Tsai says. “We know it’s the direction we want to head in, and we’re trying to work with the community to figure out what’s the fastest but most responsible way of doing that.”


