
This case study is the third in a series profiling how primary care clinics — federally qualified health centers, independent clinics, and clinics that are part of large health systems — are meeting the needs of patients with low incomes. We are now focusing on people who may not have such complex health care needs but are at risk of developing problems because they lack the resources to stay healthy. This series will profile clinics that exhibit some or all of the following attributes:
- medical home capabilities as a foundation
- multidisciplinary teams with community health workers
- integration of primary health care with public health, social services, and behavioral health
- using data to manage and improve patient care and clinic performance
- geographic empanelment, including appropriate risk stratification and targeting
- proactive patient and family engagement to address physical, social, and cultural barriers to care, and
- leveraging of digital tools to improve health.
New Mexico stands out for its widespread deployment of community health workers, as well as for state and local approaches to financing their services.

Background
Arthur Kaufman, M.D., has been on a decades-long quest to remove barriers to care for the underserved in New Mexico. Along with his colleagues, Kaufman — the vice chancellor for community health at the University of New Mexico Health Sciences Center in Albuquerque — has been pushing to redistribute Medicaid funding, academic expertise, and other resources from the state’s more privileged institutions to poor urban and rural areas.
His strategies have included establishing a family medical residency program that places trainees in poor communities and dispatching extension agents across the state to both identify pressing health, educational, and economic challenges and mobilize resources to address them. Kaufman and his colleagues have also pursued state and local government funding, as well as payer support, to hire and train community health workers (CHWs) to engage vulnerable residents and connect them with medical and social services. This case study describes the many ways CHWs have been deployed in New Mexico to promote health and tackle social challenges including unemployment and criminal recidivism.

The University of New Mexico Health Sciences Center — through a program Arthur Kaufman, M.D., oversees — has provided technical assistance and training to organizations integrating CHWs into their operations.
Deploying CHWs in the Emergency Department
The practice of embedding CHWs into medical settings in New Mexico began in earnest more than a decade ago with a pilot between University of New Mexico Hospital (UNMH) and a Medicaid managed care organization (MCO). The pilot tested whether CHWs could engage Medicaid beneficiaries using the emergency department (ED) for problems that would be better managed by primary care providers. The CHWs provided both navigation and social supports — connecting members to medical homes, making home visits, and encouraging adherence to treatment recommendations. A study found these efforts reduced ED visits and hospital admissions as well as use of prescription drugs (including narcotics) and produced a fourfold return for the health plan that sponsored it.1
Based partly on these results, New Mexico in 2014 mandated that all Medicaid MCOs directly hire or contract with CHWs and increase their numbers by a set percentage each year, beginning in 2016. Nearly one-fifth of the more than 850 CHWs now working in the state are employed directly by MCOs.2 That number is expected to increase with a 2019 state mandate that Medicaid plans provide CHW services to at least 3 percent of their members — nearly 20,000 people. In other cases, CHWs are hired by medical practices and social service agencies, either with support from the MCOs, grant funding, or, in the state’s most populous county, by diverting some of the funds designated for indigent care at the academic medical center.
CHWs are now working in federally qualified health centers, hospital emergency departments, and a clinic that serves the uninsured, as well as social service agencies focused on housing, domestic violence, legal assistance, and workforce training and a reentry center for recently released jail detainees. In many locations where CHWs work, their services are available to all vulnerable individuals, regardless of medical condition, immigration status, or source of insurance or lack of it. In all, the state’s CHWs have screened 50,000 patients since 2005 and provided services to the roughly a third who report a social need, according to Kaufman’s estimates.

Albuquerque, New Mexico.
In recent years, CHWs’ efforts have spread well beyond the initial focus on high utilizers. “Focusing on these hot spotters — the top 1 percent, 3 percent, 5 percent — really doesn’t do much for community health,” says Kaufman. “We wanted to see if we could extend our model ‘upstream’ to reach those at rising risk and more generally to promote better health within the Medicaid enrollee community.”
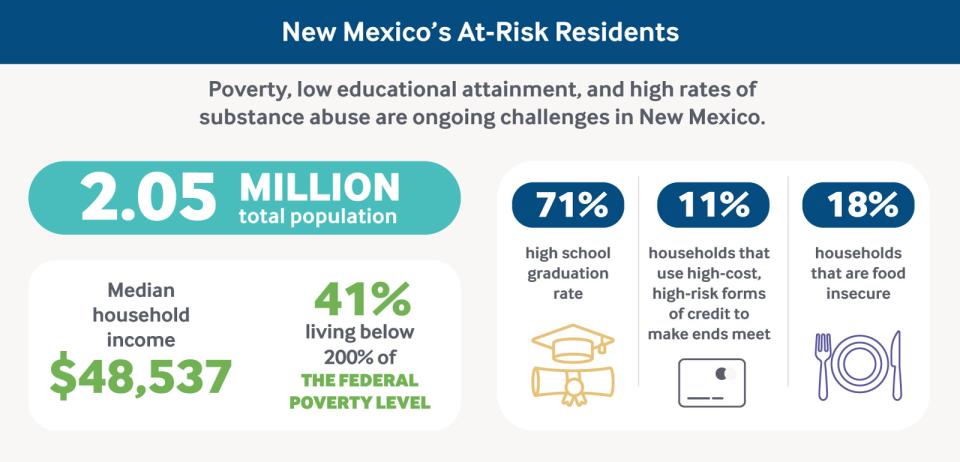
This population-based approach, while not fully realized, is borne out of dire social need. New Mexico toils near the bottom of many national rankings: It has the fourth-highest unemployment rate (4.8%), the second-highest percentage of women in poverty (one in five),and the highest number of alcohol-related deaths in the country (34 per 100,000 residents).3
Data: David C. Radley, Sara R. Collins, and Susan L. Hayes, 2019 Scorecard on State Health System Performance (Commonwealth Fund, June 2019); and Center for American Progress, “Talk Poverty: New Mexico,” 2018.
The state’s 2014 expansion of Medicaid to cover more low-income adults helped some, reducing the uninsured rate for this group from a staggering 43 percent in 2013 to 19 percent in 2017. But many residents struggle to find employment and earn a living wage in a state heavily dependent on tourism, agriculture, and mining.4
In this case study, we describe how Medicaid funding, grant support, and local tax dollars are being used to deploy CHWs in three settings:
- One Hope Centro de Vida Health Center, a primary care clinic that relies on volunteer clinicians
- First Choice South Valley Medical Center, a federally qualified health center, and
- Pathways to a Healthy Bernalillo County, a program in the state’s most populous county that aims to coordinate the work of social service agencies and reward them for success.
Helping Clinicians Understand Patients’ Financial Constraints
One Hope Centro de Vida Health Center mainly serves the International District in East Central Albuquerque. Once a thriving commercial corridor along Route 66, the neighborhood declined in the 1970s when a new freeway diverted traffic and high-density investment properties with absentee landlords displaced home ownership. Today, it has the highest rates of violent crime, domestic violence, and prostitution in the city, with poverty rates in some quarters surpassing 50 percent. It’s referred to as the International District because it is the most diverse community in New Mexico, home to Hispanics, whites, Native Americans, African Americans, and Asians. Many residents are new immigrants; some lack documentation and speak different languages, making it difficult to access health care services.
One Hope was founded in 2006 by area residents who had depended mostly on the emergency department for care and wanted to “stir up our own health care solutions,” says John Bulten, executive director of East Central Ministries Inc. (ECM), which led the effort. The nonprofit is not tied to a formal religious institution; instead, Bulten and a host of staff and volunteers live and work in the neighborhood, running an urban farm and other microbusinesses to support the clinic and other grassroots efforts to strengthen the community.
The One Hope clinic runs on a shoestring budget of $130,000 a year, raised through East Central Ministries’ microbusinesses, grants from local foundations, private donations, and patient fees. Three CHWs are its only paid staff. They manage the clinic and organize a team of volunteer physicians (many of them University of New Mexico family medicine residents and faculty), pharmacists, dentists, University of New Mexico students, and interpreters who offer services 10 days per month. The clinic serves about 100 people a month, mainly low-income, Hispanic immigrants. One Hope does not accept any insurance but instead asks patients to pay $20 per visit.
Patients often arrive with unmanaged chronic conditions, according to Lidia Regino, a CHW with 25 years of experience. Among a sample of 100 patients, more than half had diabetes or prediabetes and “most of them didn’t know they had it,” she says. Regino and other CHWs meet with all patients after their visits for a salida, or exit interview, to review the medical plan and help figure out next steps, including how to make treatment recommendations affordable. They offer advice about how to purchase prescribed drugs or get tests done at the lowest costs, for example, and negotiate discounts and payment plans for specialist care.

Lidia Regino, a CHW with 25 years of experience.
CHWs also partner with clinicians to help them understand patients’ financial constraints. “I may say, ‘Why did you ask for five labs? Out of those, which ones do you actually need and which one goes first?’” says Regino. “It’s a learning experience for the providers as well as us.” Family medicine residents from the University of New Mexico Schools of Medicine, Pharmacy, and Nursing report that the experience of working at One Hope has made them more conscious of costs and other barriers to treatment, and better able to partner with CHWs to provide thoughtful, culturally appropriate care.

Data: David C. Radley, Sara R. Collins, and Susan L. Hayes, 2019 Scorecard on State Health System Performance (Commonwealth Fund, June 2019).
One Hope has developed an innovative diabetes self-management program based on the Chronic Care Model, which combines team care, care coordination, and patient education in an effort to improve disease outcomes. One Hope’s program offers tailored supports, including one-on-one help from a CHW, frequent checkups, nutrition workshops, Zumba fitness classes, and peer support groups. The clinic is collaborating with the University of New Mexico on a $2.3 million grant from the Patient-Centered Outcomes Research Institute to compare its approach with the American Diabetes Association’s model used by the University of New Mexico’s Center for Diabetes Education. The latter relies on a certified diabetes educator and group classes. The study has recruited 452 Hispanic participants from low-income households in the Albuquerque area.
East Central Ministries also works to meet the local needs for affordable housing, healthy food, and education. The housing co-op, Casa Shalom, came into being when the group bought out a dollar-an-hour hotel used by sex workers and converted it into low-income housing. The Community Food Co-op has been in operation since 2001; members receive groceries in exchange for volunteering there. ECM also offers a free preschool and has developed a youth mentoring program and vocational training programs to help people find and keep employment.

East Central Ministries.
Sometimes patients are very reluctant to speak about what their needs are. But we definitely try to gain their trust, and we also let them know that we are part of the community, and they’re not alone, and that we can be with them in any situation.
Enhancing the Capacity of Clinics to Tackle Social Needs
First Choice South Valley Medical Center is a short drive from downtown Albuquerque across the Rio Grande, in a neighborhood that’s home to multigenerational families and new immigrants, mostly from Mexico. A vibrant community of restaurants, small businesses, urban farms, and community-based organizations, South Valley also has a high concentration of families living in poverty. Mortality rates from chronic disease and cancer are higher than in more affluent parts of Albuquerque and other parts of the state. Emergency department visits and hospitalizations from asthma, triggered by airborne pollutants, are common.5
Because the South Valley is an unincorporated region of Bernalillo County, it lacks some social services and public transportation.6 For the past decade, the South Valley Medical Center — part of the First Choice Community Healthcare (First Choice) federally qualified health center network — has been working to assess and meet patients’ needs beyond medical care as part of an effort to bolster the neighborhood’s resources and address some of the upstream causes of poor health.
Since 2014, the health center has screened patients for social needs using a locally developed, standardized survey instrument, WellRx, that asks about income, education, food, housing, transportation, utilities, safety, and substance abuse. Nearly half screen positive for at least one need during a visit, while 26 percent screen positive for between two and five. The health center has found the primary challenges are financial: 22 percent reported not having a regular source of income, while 21 percent had difficulty paying for utilities. The clinic has also found significant rates of food and housing insecurity.
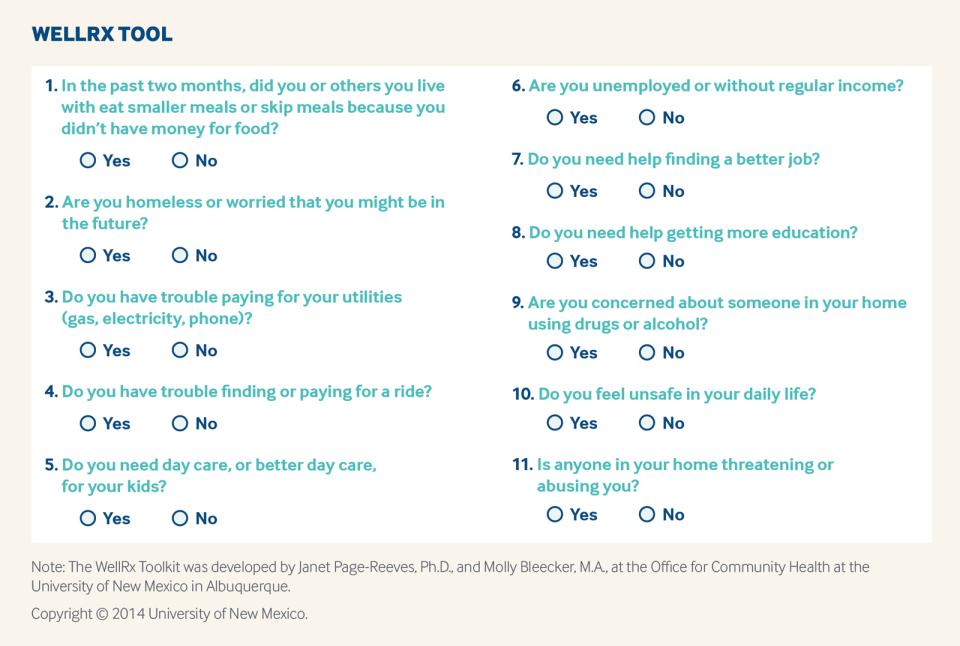
Those who screen positive for a social need (46%) are asked if they wish to see a CHW who can connect them to support available from community-based organizations with expertise addressing food insecurity, housing instability, and poverty. CHWs also are able to connect patients to the clinic’s community health educators, who offer coaching to help people understand and manage their health conditions, especially diabetes, which affects about 20 percent of South Valley Medical Center’s 10,000 patients.

Margarita Perez-Pulido (left) with fellow CHW Kelly Morantes.
CHWs have also made educational programs relevant to patients. When they weren’t getting many takers for a plant-based cooking class, for example, they helped launch a nutrition course so that operators of local day care facilities could earn nutrition certification; up to 100 people now attend each class.
Initially, the MCOs reimbursed CHW services at South Valley by paying a capitated fee ($2.19 to $5.75 per member per month) for each member assigned to a health center provider. First Choice now covers CHW costs directly. The health center has found CHW involvement on medical teams results in higher rates of cervical cancer screening (63.5% at clinics that make use of CHWs vs. 57.8% at those that do not), flu vaccination (43.5% vs. 38.5%), and breast cancer screening (49.1% vs. 48.8%).

First Choice South Valley Medical Center, a federally qualified health center.
We want to see if we can do something on our campus that will dramatically improve the health trajectory of patients that come here before they get here.
Investing in South Valley’s Future
First Choice South Valley Medical Center is located within a health commons designed to provide “one-stop shopping” for residents seeking social, behavioral, and medical services. The health commons also aims to fuel the economy by offering training and good jobs.7 Built in 2008 with $10 million in county, state, and federal funding, the main building includes the health center, which has integrated behavioral health and dental services; a state public health department clinic; and the office of the Special Supplemental Nutrition Program for Women, Infants, and Children. The wider campus includes a teen shelter for at-risk youth, a psychosocial rehabilitation facility providing job and life skills training for individuals with disabilities, and a Head Start preschool.
To move further upstream in addressing local needs, First Choice is attempting to raise $26 million with the local and federal government, national and local philanthropies, local businesses, health insurers, and health systems. If successful, this investment would enable First Choice and its partners to expand the South Valley Health Commons and create what First Choice CEO Bob DeFelice calls a wellness ecosystem. It would include a workforce development center, a facility for local farmers to package and store their produce, and a farm-to-table restaurant — helping South Valley’s small farmers expand their distribution capacity and build a local food production and service workforce. The health center is selling a portion of the land to the Health Leadership High School, a charter school that focuses on health professions.
Link to video: https://youtu.be/cvLYeS9GmJo.
Embedding CHWs in Social Service Agencies
Pathways to a Healthy Bernalillo County (Pathways) deploys CHWs in 15 different social service agencies and community-based organizations. CHWs identify and support low-income residents who have difficulty navigating the health and social service sectors because of language barriers, substance abuse problems, poor health literacy, and other challenges.
Launched in 2009, Pathways is modeled after an Ohio program that assigns responsibility for helping people reach goals (e.g., finding a medical home or health insurance) to coordinators who are paid for achieving certain milestones.8 The coordinators oversee referrals to different agencies and facilitate communication among them. The objective is to strengthen social service capacity, remove barriers to services, and create conditions so people can improve their health over time.
During the past decade, CHWs have helped some 5,800 individuals identify and work on up to three goals, selected from among 18 pathways. Some of the most frequently selected include establishing a regular “health care home” with a primary care provider, locating stable housing, and securing employment. CHWs have also helped people establish relationships with primary care providers, find health insurance coverage, and obtain assistance to pay off medical debt.
A high percentage of those seeking employment assistance from the Pathways program have a criminal record (40%), and more than half have a mental illness, requiring CHWs to draw on their community relationships to find them positions, often in car washes, hotels, and fast-food restaurants. The CHWs, referred to as navigators, also help residents create resumes, apply for jobs, and prepare for interviews. Half of those who attempted the employment pathway between 2010 and 2016 completed it (533 of 1,176) and remained employed for at least three consecutive months, according to a county-sponsored evaluation of the program. But most of the jobs pay the minimum wage, which leaves those hired precariously close to the poverty line and still dependent on some food and housing subsidies.9
The county recently opened a Resource Re-Entry Center where Pathways navigators can meet with people upon release from detention to engage them and offer them support.10
Pathways leaders use a centralized information system to confidentially track clients’ progress, allowing them to monitor outcomes and offer the CHWs advice. CHWs also meet monthly to share ideas and lessons. They have also met with leaders of various agencies — from Medicaid to the income support and motor vehicle divisions — to explain how departmental policies create barriers to access, whether intentional or not. “This has resulted in better communication with and access to leadership within these agencies,” says Daryl Smith, M.P.H., program manager of Pathways to a Healthy Bernalillo County.
Supporting Residents in Need
CHWs in the Pathways program support Bernalillo County residents with one or more of the following risk factors:
- multiple or complex unmet needs and poor health
- three or more hospital stays or emergency department visits within the previous 12 months
- homelessness with disconnection from services
- previous incarceration or recent release from jail or prison (about 22% of clients)
- experiencing hunger and averaging fewer than two full meals daily
- urban off-reservation Native Americans who are not connected to or trusting of the resources available in Bernalillo County
- undocumented and/or limited-English-proficient immigrants and refugees who encounter barriers when trying to navigate the health, social services, educational, and legal systems, and
- any of the above who are parenting young children.
The Pathways program spends an average of $1,600 per client, which is paid for through an agreement between the county and University of New Mexico Hospital, which reallocates $1.2 million in local property taxes designated for indigent care at the hospital.11 Typical milestones for payment are client enrollment, engagement of the client in a particular pathway (such as establishing a medical home or obtaining medications for at least three months), and completion of the chosen pathway. Two pathways are reimbursed at a higher rate, reflecting both the increased difficulty and impact of completion: employment and housing.
A strength of the Pathways program is its focus on achieving sustainable outcomes. Typically, a pathway is not considered complete until three to six months after a service like supportive housing has been arranged and the client’s housing remains stable on follow-up. From 2009 to 2017, clients completed 61 percent of the 11,755 pathways initiated. Three of four clients who answered a survey reported their health had improved since participating in Pathways. Nearly as many said they had a better understanding of how to utilize health and social services, while two-thirds said their ability to advocate for themselves had improved.
Still, Pathways has struggled to engage those recently released from detention. Of the roughly 400 people who have been referred to Pathway organizations, only 89 (22%) have become clients. “Once they exit the facility, we are learning that many do not follow up on their referrals to the community sites,” Smith says.
Reaching Remote Parts of the State
Community health workers are also helping residents in rural and frontier parts of the state, where access to health care is limited. CHWs working at a federally qualified health center in Hidalgo County, a remote area separated from Albuquerque by the Gila National Forest, coordinate travel to specialist appointments in Albuquerque, more than a four-hour drive away, and link patients to local food pantries, housing supports, and other services.
CHWs also try to strengthen social ties. One helped a patient with severe anxiety who had trouble sleeping and said she couldn’t afford a blanket weighted with pellets, which had been suggested by her therapist to relieve stress. The CHW located a local quilters guild that made the blanket themselves. “When I handed it to the client, she started crying,” says Edith Lee, L.M.S.W. “The support of the community did more for her than anything I could have said.”
In remote regions of New Mexico home to Navajo and other Native American groups, community health representatives help tribal members access services, provide education, and advocate for their needs.
The referenced media source is missing and needs to be re-embedded.
Challenges
Many of New Mexico’s CHWs come from the low-income communities they serve and call on their shared experience to build relationships with patients. They’ve also used their knowledge to help providers fine-tune their approaches, encouraging them to attend to patients’ financial and social challenges and eliciting information to guide treatment plans. To build on these efforts and fulfill the goal of promoting better population health, New Mexico’s health care providers and policymakers will need to confront several challenges.
Establishing a Sustainable Funding Model to Pay for CHW Services
Finding resources to hire a sufficient number of CHWs to meet demand in a state where 40 percent of the population lives below 200 percent of the federal poverty level is a significant challenge. New Mexico’s mechanism — mandating their use by Medicaid MCOs and in one county, redirecting funds intended for indigent care at a public hospital to social service agencies — is a start but has yet to reach all those who would benefit.
Other states have broadened scope-of-practice laws for CHWs to enable Medicaid reimbursement, often for targeted case management. States have also used Medicaid waivers and state plan amendments to fund CHWs’ work with discrete populations, including patients with chronic conditions receiving care in health homes. An alternate approach is to create billing codes for particular CHW services, as Indiana and Minnesota have done for health education and promotion.
States could also pursue pay-for-success models, which make payment for services contingent on achievement of measurable outcomes. For example, such arrangements could be used to contract with corrections agencies that could reward CHWs if their efforts help reduce expenses linked to recidivism.
Some combination of these financing strategies may be necessary to support CHWs over the long term. “Stability requires diversity of funding,” says Carl Rush, principal of Community Resources, a consultancy that provides policy and training assistance to CHW programs nationally.
Creating a Mechanism for Tracking the Return on Investment in CHWs
Convincing state and local agencies outside of the health sector to support CHW services may require more explicit evidence of the return on investment. Much of the early evidence to support CHW use in New Mexico came from the pilot program involving Medicaid beneficiaries who were relying on emergency departments for care.12 Getting a clear picture of the impact of less intensive interventions has been complicated by how difficult it is to get claims data from managed care plans and aggregate them with information from the diverse array of organizations that employ CHWs. The Pathways program includes an evaluation, but many of its cost savings estimates are based on research into CHW interventions and medical home implementations elsewhere that show declines in emergency department and hospital use, as well as reduced use of public services like jails. To quantify the impact of such programs, states may need to mandate the timely sharing of claims data.
Promoting Better Population Health — Not Just Reducing Medical Costs
In response to New Mexico’s mandate that Medicaid managed care plans provide CHW services to 3 percent of beneficiaries, plans have hired more CHWs. Albuquerque-based Presbyterian Health Plan, for instance, increased the number of CHWs it employs from nine to 26. Presbyterian’s CHWs have reached out to high-risk patients including those with hepatitis C, pregnant women who miss prenatal appointments, and those with poorly managed diabetes. They also provide services to those with lower medical risks but unmet social needs.
Promoting better health among Medicaid beneficiaries overall is a key challenge — and one CHWs alone cannot overcome. Efforts such as those being trialed in Albuquerque’s South Valley to strengthen communities by building stronger schools and creating better career pathways are important complements to their work, as are policies that promote educational opportunities and economic development in poor areas.
Acknowledgments
The authors gratefully acknowledge the following individuals who generously shared information and insights. Community Resources: Carl Rush. First Choice South Valley Medical Center: Will Kaufman, Michelle LaPorte, Kelly Morantes, and Margarita Perez-Pulido. Hidalgo Medical Services: Edith Lee, Dan Otero, and Marsha Rippetoe. New Mexico Human Services Department: Megan Pfeffer. O’Donnell Economics and Strategy: Kelly O’Donnell. One Hope Centro de Vida Health Center: John Bulten and Lidia Regino. Presbyterian Health Plan: Cynthia Al-Aghbary. Resource Re-Entry Center: Claudia Timmons. University of New Mexico Health Sciences Center: Arthur Kaufman, Marnie Nixon, Carolina Nkouga, Toyese Oyeyemi, Laura Parajon, Francisco Ronquillo, and Daryl Smith. Southwest Center for Health Innovation: Charlie Alfero, Alicia Herrick, and Holly H. Hudgins.
Commonwealth Fund case studies examine health care organizations that have achieved high performance in a particular area, have undertaken promising innovations, or exemplify attributes that can foster high performance. It is hoped that other institutions will be able to draw lessons from these cases to inform their own efforts to become high performers. Please note that descriptions of products and services are based on publicly available information or data provided by the featured case study institution(s) and should not be construed as endorsement by the Commonwealth Fund.