Introduction
Medicare beneficiaries receive their Medicare-covered benefits through either traditional Medicare (TM) or private insurance plans known as Medicare Advantage (MA) plans. In 2024, more than half of Medicare beneficiaries were enrolled in MA plans. One feature driving enrollment in MA plans1 is that they typically provide supplemental benefits not covered by TM.2 These can include vision, hearing, dental, fitness, and over-the-counter medication coverage, as well as other benefits.
Because MA plans are allowed to tailor benefit packages, there can be significant differences in the types of benefits covered and the scope of coverage. For example, some MA plans offer only preventive dental services, such as X-rays and cleanings, and others offer more comprehensive dental benefits, such as periodontal care or restorative care. Most supplemental benefits are required to be “primarily health related” — for example, adult day care, bathroom safety devices, nonemergency medical transportation, or therapeutic massage.3 For chronically ill enrollees, however, MA plans can offer other benefits, such as pet food, pest control, grocery shopping, air purifiers, and in-home living support services.
Supplemental benefits are largely financed by rebates that the Centers for Medicare and Medicaid Services (CMS) pays to the plans. Rebate payments are a percentage of the difference between the plan’s per member per month (PMPM) bid to offer Medicare benefits and the maximum PMPM payment that CMS sets annually as the county-level benchmark. Plans with higher quality ratings receive a larger share of the difference.
Over the past decade, annual payments have increased dramatically, from $12.0 billion in 2014 to $60.5 billion in 2023.4 Every year, MA plans submit information about the supplemental benefits they will offer for the upcoming plan year, but there are only limited data on beneficiaries’ utilization of these benefits.5 Accurate data on the value and use of supplemental benefits could inform policy discussions and the federal government’s oversight of these benefits.
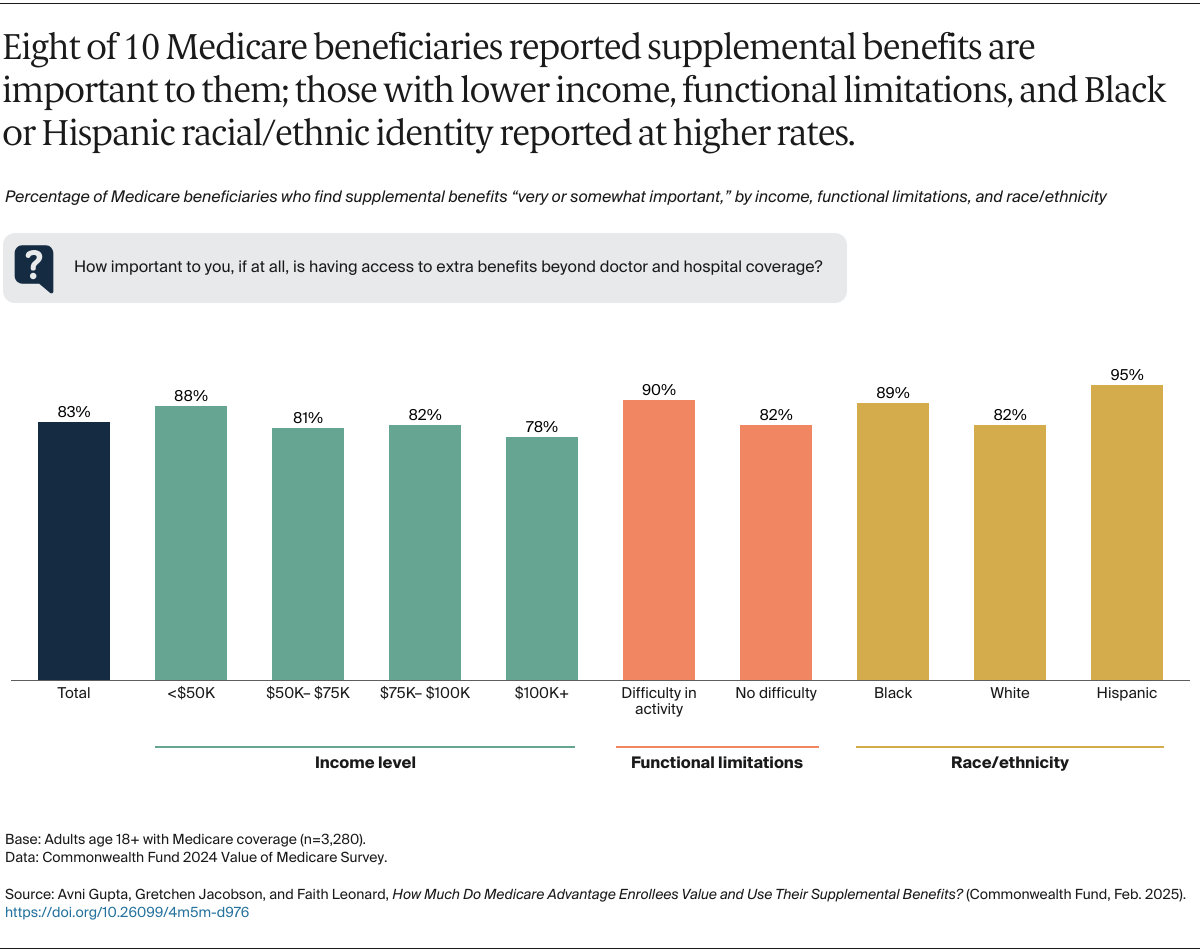
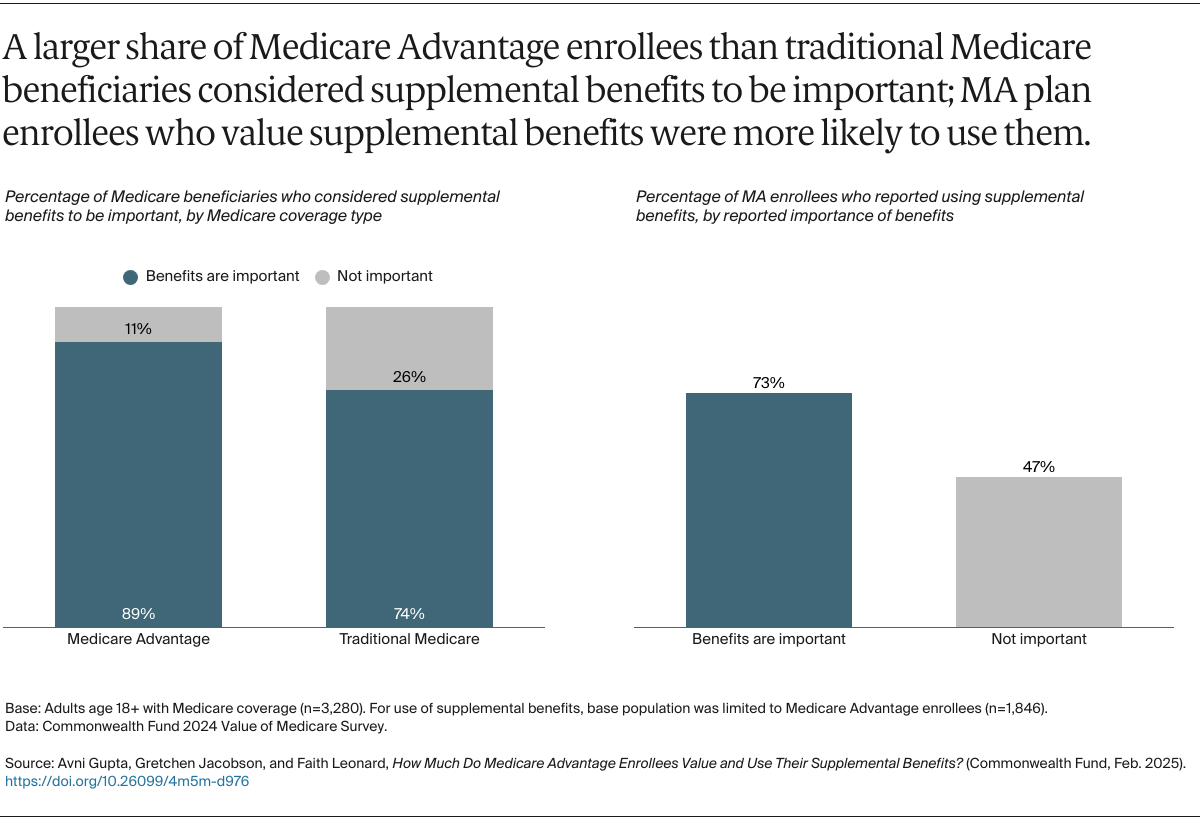
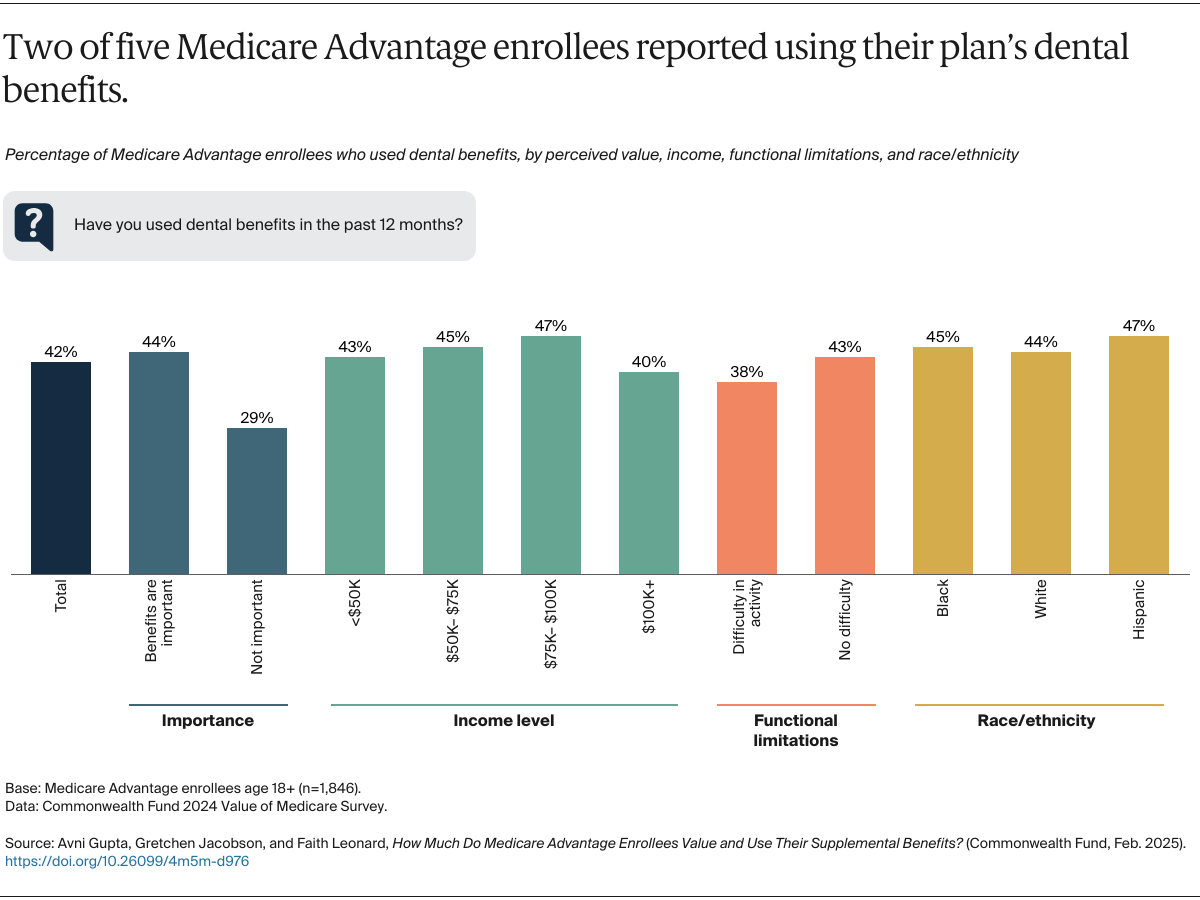
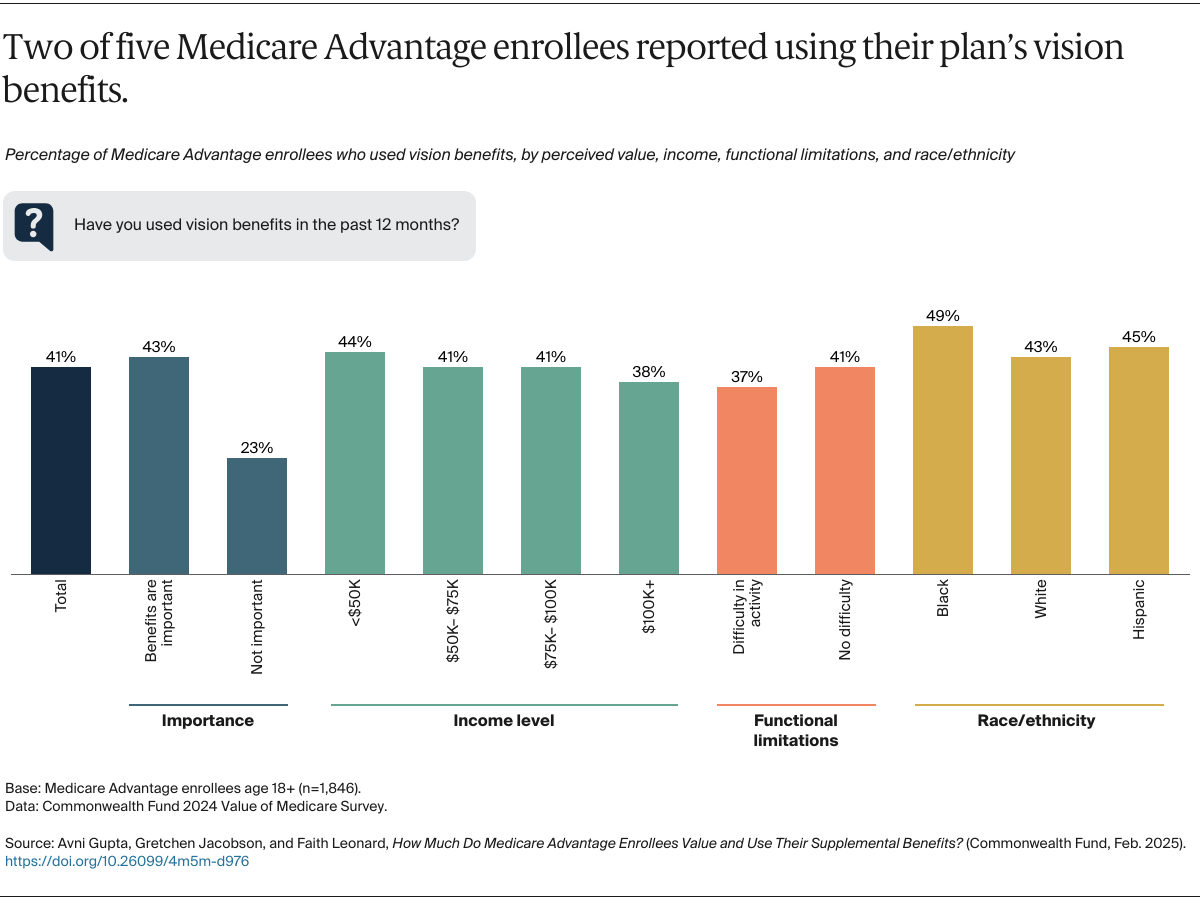
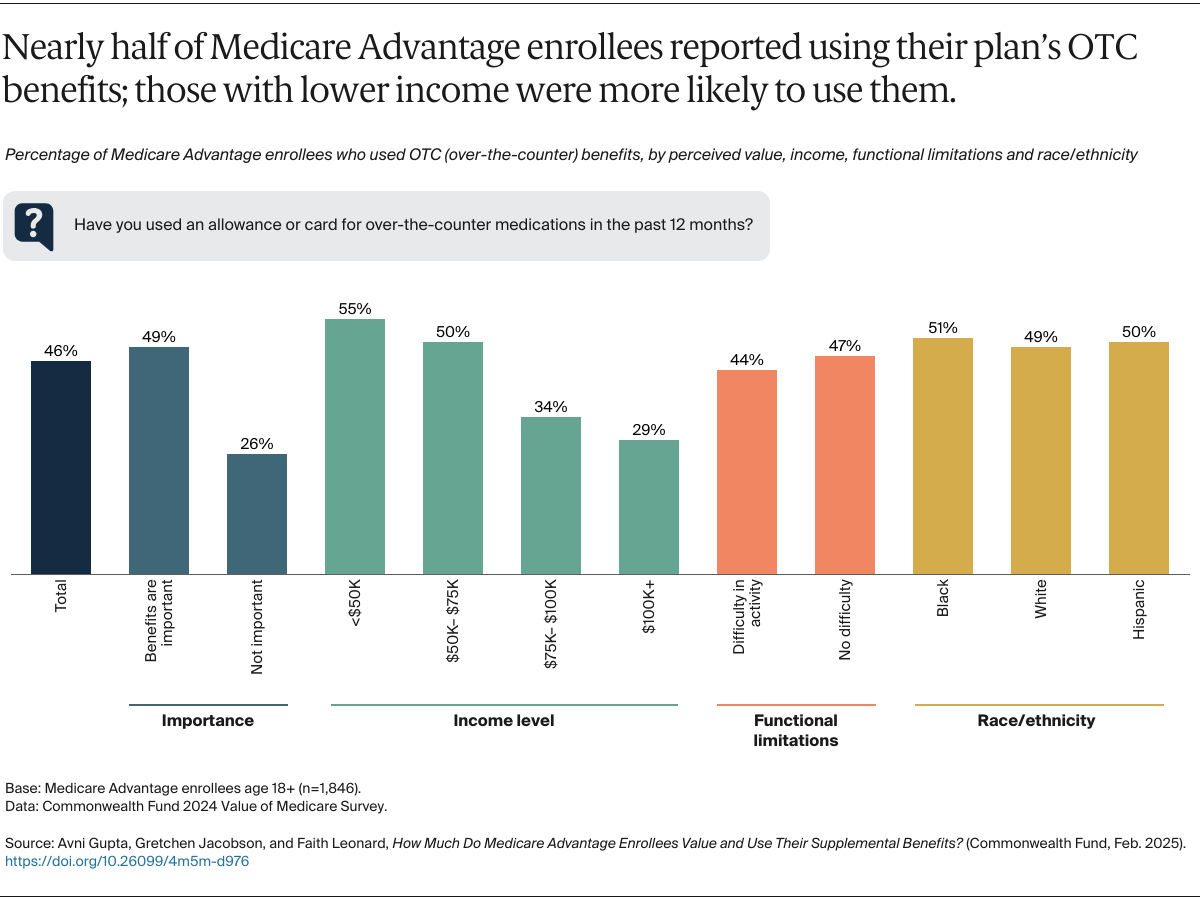
In an earlier analysis of the Commonwealth Fund 2024 Value of Medicare Survey, we found that seven in 10 MA beneficiaries reported using some of their supplemental benefits, with varying rates of use by different types of benefits.6 In this brief, we examine the same survey findings to understand how beneficiaries perceive the value of different supplemental benefits and whether that perception is associated with their relative use of these benefits. We analyze the responses by beneficiaries’ annual income level, race/ethnicity, functional limitations, or health-related difficulties in caring for themselves (such as eating or bathing). (See “How We Conducted This Survey” for more details.)