Marlene Kennedy (left) and her daughter Deb Kennedy leave the Emerald Nursing & Rehab facility in Cozad, Neb., on December 3, 2019, after visiting Marlene’s husband of 64 years (and Deb’s dad), Earl Kennedy. The closure of a nursing home in Broken Bow, Neb., forced Earl, an 88-year-old with Parkinson’s disease, to move to another facility an hour away. Rural seniors have less access to health care and long-term services and supports than other older adults. Photo: Michael S. Williamson/Washington Post via Getty Images
Marlene Kennedy (left) and her daughter Deb Kennedy leave the Emerald Nursing & Rehab facility in Cozad, Neb., on December 3, 2019, after visiting Marlene’s husband of 64 years (and Deb’s dad), Earl Kennedy. The closure of a nursing home in Broken Bow, Neb., forced Earl, an 88-year-old with Parkinson’s disease, to move to another facility an hour away. Rural seniors have less access to health care and long-term services and supports than other older adults. Photo: Michael S. Williamson/Washington Post via Getty Images
Toplines
To increase the number of health care providers and long-term services for older adults in rural communities, advocates should partner with older adults and build on local assets
Rural communities would also benefit from regulatory and payment changes, new resources, and technical assistance to bolster their efforts to better support older adults
Toplines
To increase the number of health care providers and long-term services for older adults in rural communities, advocates should partner with older adults and build on local assets
Rural communities would also benefit from regulatory and payment changes, new resources, and technical assistance to bolster their efforts to better support older adults
The article is part of a partnership between the Commonwealth Fund and the Bassett Research Institute in Cooperstown, N.Y., to explore innovative approaches to the health care challenges facing rural communities across the United States.
Introduction
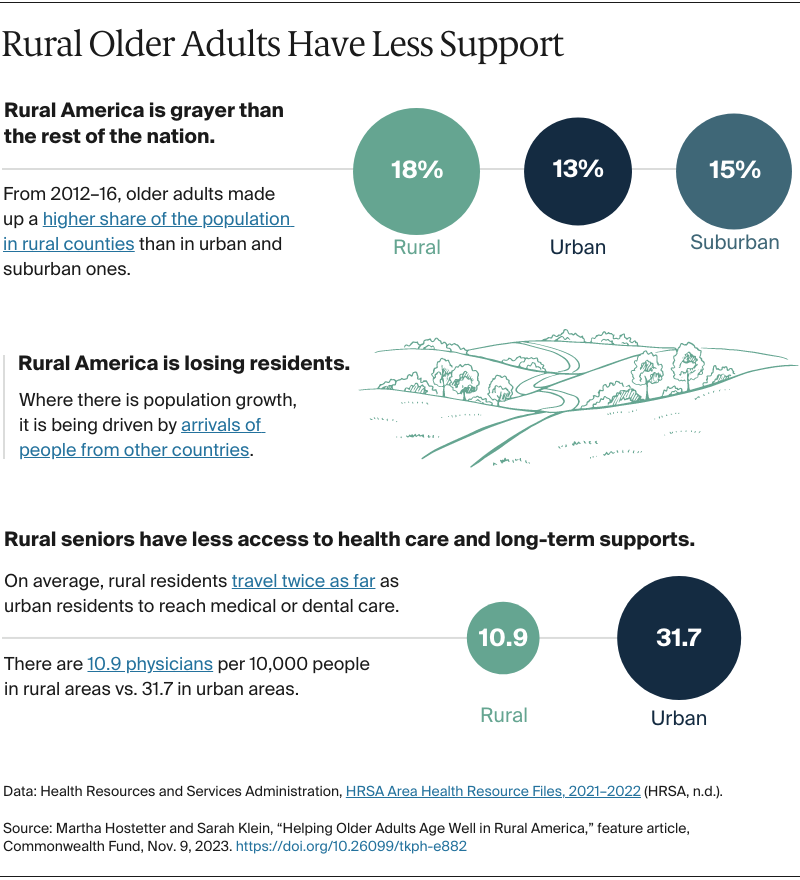
Many rural older adults have lived their whole lives in the same small towns, some in the same homes. Others are more recent arrivals, including the aging parents of immigrants who’ve come to work in agriculture, energy, or other industries. Like older adults across the country, rural seniors tend to want to age in their communities, amid familiar people and places. But with fewer health care providers, fewer professional caregivers, and fewer young people than in urban areas, rural communities struggle to care for aging residents.
“It’s the number-one challenge rural communities are facing,” says David Trost, CEO of a senior housing services provider in Billings, Montana. “The folks who are staying are old. And the folks who are leaving are young, and so there’s fewer people to serve the old.” These challenges are exacerbated by the fact that rural older adults tend to have higher needs; compared with urban and suburban older adults, they are more likely to live in poverty and more likely to have chronic illnesses.
In this report, we showcase health care and long-term care providers working to strengthen services for rural older adults. Some focus on making hospitals and other care providers “age-friendly,” while others try to make it easier for rural seniors to access medical care and social supports. Given that many rural providers are facing financial shortfalls and workforce shortages, we also consider what payment and policy changes might be needed to sustain and spread efforts to help older adults age well in rural America.
Mobilizing Local Assets
In rural communities, where the nearest hospital, clinic, or nursing home can be miles away, health and human service organizations often fill gaps. Lutheran Services in America — a national network of 300 health and human services providers that offer senior housing, caregiver support, transportation, nutrition, and other supports — recently launched the Rural Aging Action Network. Participants have come together in Minnesota, Montana, North Dakota, and South Dakota to better understand and respond to the needs of older adults in their communities, including towns of fewer than 700 people.
Many of the older adults they’ve heard from are used to relying on themselves; when they do need help, they reach out to neighbors and members of their faith communities. But they worry about what will happen when these sources of support become too old or frail themselves.
Assessments of older adults by members of the Rural Aging Action Network found:
In addition to health care, older adults reported unmet needs for affordable food and transportation.
Older adults also needed help paying utility bills, coping with extreme weather conditions, and accessing technology.
Many older adults who were immigrants to their communitiesalsoneeded legal and translation services.
Lived Voices: Aging in Rural America — Stories of Independence, Community Connections, and Vibrant Lives
Data: Lutheran Services in America, LeadingAge LTSS Center @UMass Boston. Video courtesy of Lutheran Services in America.
St. John’s United, a member of the Rural Aging Action Network, provides senior housing in and around Billings, Montana. In 2019, St. John’s launched At Home services for clients living in their own homes. This monthly subscription service is offered on a sliding scale and provides seniors with rides to medical appointments, help with household tasks, social outings, and other supports.
St. John’s is pursuing partnerships to make At Home services more broadly available, including one with Sidney Health Center, a critical access hospital four hours’ drive from Billings. Critical access hospitals are facilities with 25 or fewer beds located more than 35 miles from another hospital. In 2022, 60 percent of respondents to Sidney Health’s community health needs assessment were age 55 or older, and wanting to age in place emerged as a chief concern.
Using a $270,000 grant from Sidney Health, St. John’s staff will screen patients 70 and up who visit the emergency department (ED) more than twice in a year but aren’t admitted. The goal is to understand what’s driving older adults to the ED: Do they need help managing their chronic conditions? Are they socially isolated or depressed? St. John’s staff will then try to connect them to services. “By partnering with St. John’s, we can identify unmet needs and build out services like transportation and nutrition to complement services we already have, like visiting nurses and care coordination,” says Jen Doty, Sidney Health Center CEO.
“We can be a matchmaker,” says St. John’s United CEO David Trost. “Sometimes people don’t know what they need, or they’re afraid to ask for help.” St. John’s will track whether ED visits and hospital readmissions are lower among seniors who receive home-based services. If so, this work could save money for Sidney Health and other rural hospitals, which often admit older patients who come to the ED because they lack the support needed to recover at home. Doing so can lead to financial penalties under Medicare’s Hospital Readmissions Reduction Program, which reduces payments to hospitals with excess readmissions.
The referenced media source is missing and needs to be re-embedded.
Reier Thompson, CEO, Missouri Slope
Missouri Slope, a nonprofit providing elder housing and services in and around Bismarck, North Dakota, is another member of the network. It has brought together senior centers, health care organizations, home health agencies, transportation companies, and others to identify local resources. For example, leaders are enlisting high school students to help older adults with technology and asking people who regularly commute from small towns into Bismarck to offer rides to older adults. The organization is also planning new services, such as delivering meals to seniors’ homes or deploying staff who live in rural areas to check on older adults. “It’s that hub-and-spoke concept,” says Reier Thompson, its CEO. “We need to activate people who are already in these communities in new ways, whether it as an employee or as a volunteer.”
If older adults are having to travel for health care or other services, pretty soon it just becomes too overwhelming. They just move to Bismarck. Then those communities lose their population and their people, their stories, their history. And economically, too, it’s a big impact on the community. If we can continue to help them stay at home, stay well longer, we can help these communities thrive.
Reier Thompson
CEO, Missouri Slope
Helping Rural Older Adults Age in Place
Rural seniors who want to age in their own homes often struggle to find professional caregivers, making them more likely than their urban and suburban counterparts to depend on family or end up in skilled nursing facilities. Even the latter can be hard to find: because of financial shortfalls and staff shortages, some 440 rural nursing homes have closed or merged with others in the past decade.
In Kansas, the nonprofit Midland Care operates four Programs of All-Inclusive Care for the Elderly (PACEs), which serve 500 Kansans who require nursing home–level care across 12 counties. PACEs pool capitated Medicare and Medicaid funds to provide medical and long-term services, including checkups, rehabilitation services, home visits, day centers, meals, and wraparound supports that enable elderly people to preserve their independence and avoid entering nursing homes. A 2021 report found that beneficiaries enrolled in PACE were less likely to visit EDs or be hospitalized than those enrolled in Medicare Advantage plans.
While Midland’s PACEs are popular with residents of Topeka, Kansas City, and the college towns of Lawrence and Emporia, leaders have struggled to bring the program to sparsely populated rural areas. “Most of the counties in Kansas aren’t served by PACE because there isn’t enough population density to serve beneficiaries within one hour of driving distance from a PACE center, as required by the program,” says Shawn Sullivan, Midland’s CEO. And without sufficient volume, a PACE organization can’t sufficiently spread the financial risk inherent in taking on capitated payments.
We’re providing transportation from their home to the day center. They’re getting a lot of personal care assistance, meals, therapy, and going to see their physicians or nurse practitioners. There’s a real shortage of these services in rural areas.
Shawn Sullivan
CEO of Midland Care
Midland Care operates four Programs of All-Inclusive Care for the Elderly in Kansas. Photo courtesy of Midland Care.
Nationally, only 24 of 151 PACEs are rural. Advocates say that, if given greater flexibility, PACE organizations could serve many more rural adults, and leaders in the field are working with policymakers to discuss ways to make PACE more feasible in rural states. Advocates are requesting a pilot to test changes to PACE rules to bolster rural participation, including allowing Medicare beneficiaries who don’t qualify for Medicaid to participate.
Advocates would also like to see rural PACEs given flexibility to partner with critical access hospitals, senior centers, area agencies on aging, and others. Kansas has 84 critical access hospitals, some of which could serve as day centers for PACE participants, Sullivan suggests, while health care providers already working in rural areas could serve part time on clinical teams.
Jeff Colyer, M.D., the former governor of Kansas and the chair of the National Advisory Committee on Rural Health and Human Services, believes PACEs can knit together partnerships among rural health and social service providers. “In a couple of years, about 30 percent of Kansas counties are going to have more than a third of their population over age 65,” he says. “With PACE, you can start to do some creative things,” he says, pointing to greater use of technology, including remote patient monitoring and virtual visits, and the use of mobile clinics.
Becoming “Age Friendly”
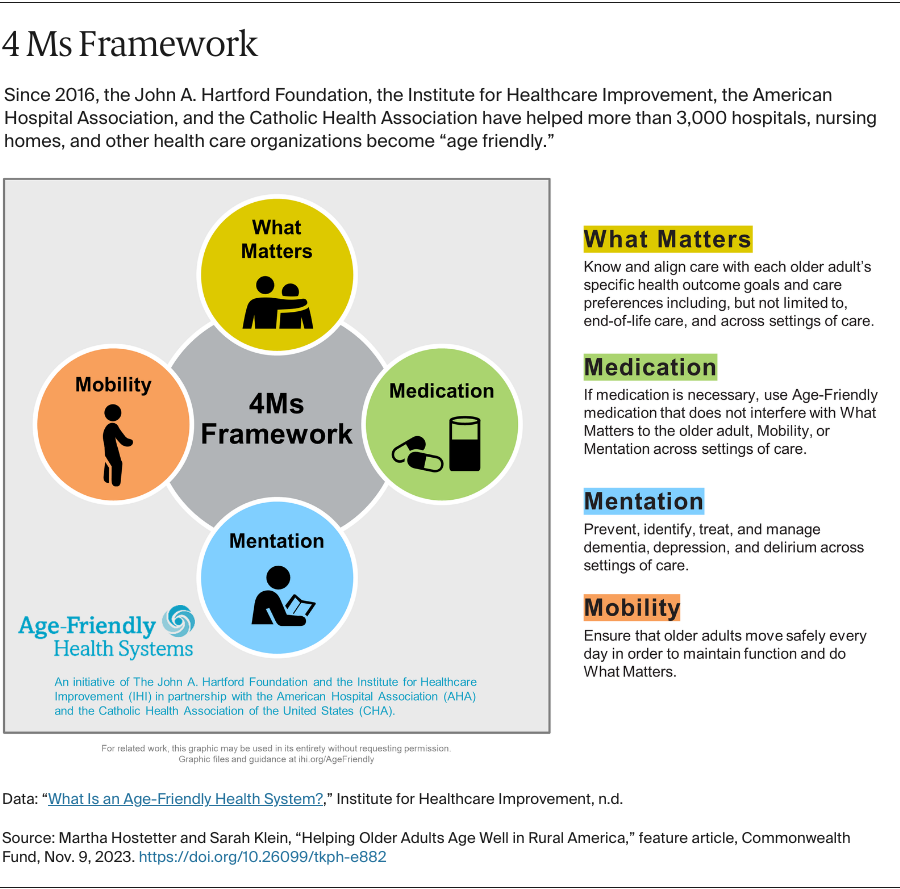
In Nebraska, two-thirds of hospitals are considered critical access hospitals, and adults over age 65 are the fastest-growing population. Since 2019, the Nebraska Hospital Association has been convening hospitals to help them adopt the age-friendly framework, a widely used approach that focuses on what matters to older adults, their medication, mentation, and mobility.
Participating hospitals share data, set improvement goals, and track progress in addressing common problems, like falls or prescribing medications that can be harmful for older adults. One effort focuses on delirium. “We thought of delirium as only happening to the sickest of the sick in intensive care units,” says Margaret Woeppel, R.N., vice president for workforce, quality, and data at the hospital association. “But we’re finding that delirium is much more common and can lead to confusion, anxiety, and other negative outcomes. It affects how you do in the hospital, how you recover, and whether you will go home or not.”
A geriatric-certified pharmacist from one of the hospitals shared ways to avoid medications that put people at risk for delirium, and participants brainstormed ideas for helping people struggling to sleep, which can fuel the problem. Nurses and pharmacists at one hospital created a sleep kit that includes nonpharmacological sleep aids, and the hospital association is helping hospitals adapt their electronic medical record systems to make screening for delirium and delirium risk mandatory.
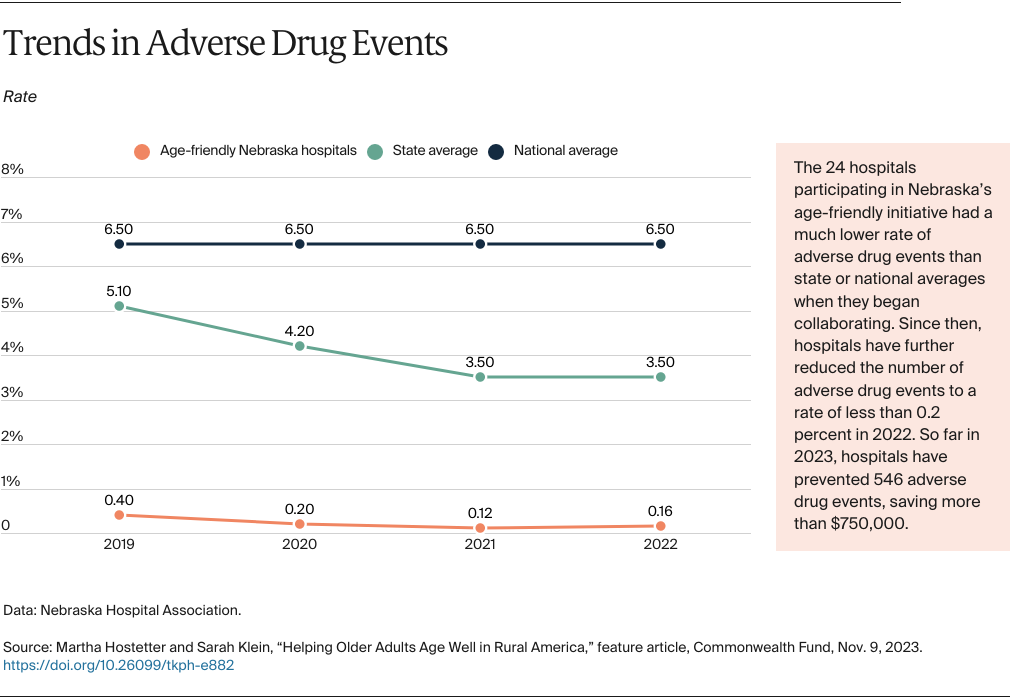
So far, of Nebraska’s 92 hospitals, 22 — nearly all of them designated as critical-access — have been certified “age friendly,” along with 22 clinics. This means these providers have demonstrated changes in their practices and performance. In addition, the 24 hospitals participating in Nebraska’s age-friendly initiative have reduced readmission rates by 4.6 percent since 2020, according to the association.
Leaders are extending this approach to skilled nursing facilities, assisted living facilities, home health agencies, pharmacies, and others. One hospital partnered with a community pharmacy to help pharmacists recognize options for deprescribing. The goal is to make Nebraska an age-friendly state. “Rural is at an advantage because we’re small and you can influence rapid change,” says Woeppel. “You know who the players are.”
Bringing Primary Care to People’s Homes
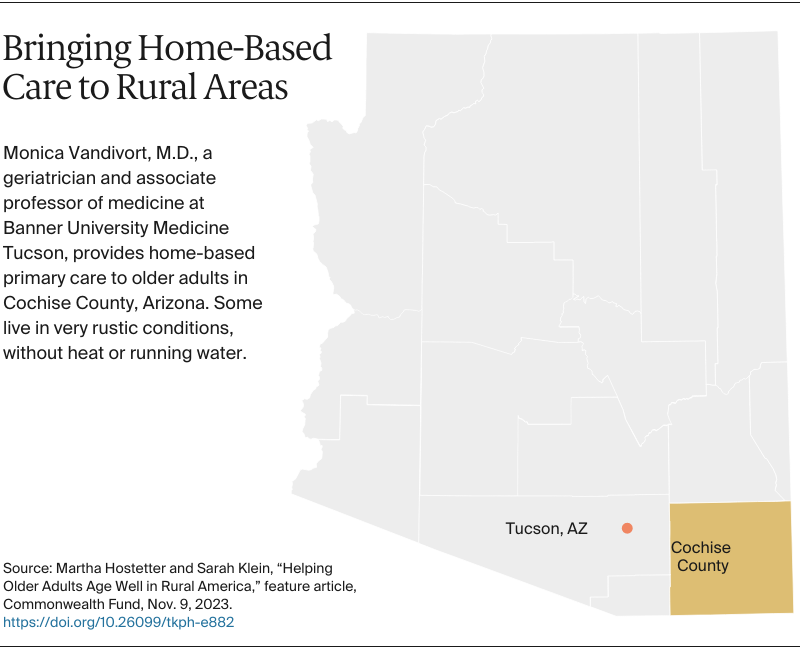
Monica Vandivort, M.D., a geriatrician and associate professor of medicine at Banner University Medicine Tucson, drives miles to visit her patients across Cochise County, Arizona, a high desert region along the border with Mexico that’s 6,219 square miles but has only 125,000 residents. Vandivort’s car is packed with a cooler of medications, IV fluids, a nebulizer, wound care supplies, and other equipment. She makes eight to 10 home visits a week to older adults who have chronic health conditions and functional limitations, such as trouble walking or eating. When someone misses an appointment at her clinic in the small town of Sierra Vista, she might go to them. “One woman canceled her appointment because she was too sick to come in that day,” says Vandivort. “That’s crazy. When she's sick is when she should see me.”
Participants in Medicare’s long-running Independence at Home Demonstration have shown that having multidisciplinary care teams make regular home visits to beneficiaries with chronic conditions and functional limitations reduces per-beneficiary spending, mainly by avoiding complications. But home-based primary care programs are rare in rural settings. Given the low volume of patients, staffing and providing round-the-clock coverage can be challenging.
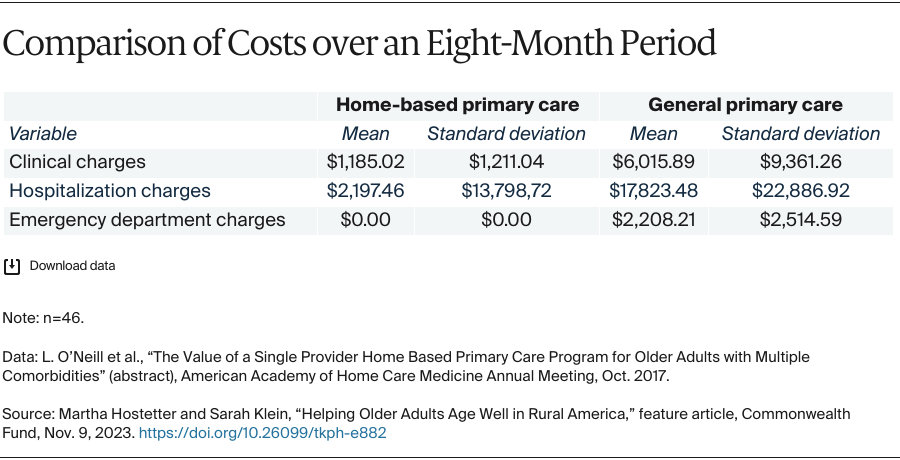
Researchers at the University of Arizona studied Vandivort’s solo approach, with an eye toward understanding whether it works as well as team-based approaches. They compared the total medical costs for patients Vandivort treated in their homes over eight months to the total costs for similar patients who received the usual clinic-based care. They found Vandivort’s patients incurred significantly lower costs for clinic visits, hospitalizations, and ED care, suggesting this solo practitioner model could be viable in other rural areas.
Vandivort, like other house call providers, doesn’t earn Medicare reimbursement for the time it takes her to drive to patients’ homes, but she’s able to balance her schedule and earn her salary from Banner by also seeing patients in assisted living and skilled nursing facilities.
Still, she says, she could extend her reach by partnering with paramedics. “If I diagnosed a patient with pneumonia, a paramedic could then visit to continue daily antibiotic injections, perform cardiopulmonary reassessments, and train patients on breathing treatments,” she says. Rural community paramedicine programs in Maine, Minnesota, Wisconsin, and elsewhere have shown they can improve health outcomes by deploying paramedics to help people manage their conditions.
In 2017, with grant funding from Arizona’s Area Health Education Center, Vandivort piloted a program to foster collaboration among paramedics working for the Sierra Vista fire department and staff at local primary care clinics. She educated participants on geriatric conditions such as chronic heart failure, cellulitis, and diabetes and encouraged primary care providers to refer patients who might benefit from paramedic visits. The subsequent visits reduced 30-day rehospitalization rates among participants from 19 percent to 8 percent, according to Vandivort and her colleagues.
They’re tough people and they choose to live like that. We make sure they’re safe, they have protection from the elements. Living alone like this has some risks for older people. You try to lessen those but you can’t take all risk away.
Monica Vandivort, M.D.
Geriatrician and associate professor of medicine, Banner University Medicine Tucson
Funding beyond grants would be needed to sustain this partnership. Arizona does reimburse community paramedicine services for Medicaid beneficiaries through the Mobile Integrated Health Care and Treat and Refer programs, both of which allow EMTs or paramedics to evaluate, treat, and refer patients without taking them to hospitals. But some requirements, such as the need for a formal quality improvement process, can be hard to implement among paramedics employed by small rural fire departments. And the programs would not cover patients insured by Medicare or other payers.
In addition, in Arizona and some other states, paramedics are only allowed to take medical direction from emergency department clinicians. Some states, including New York, have amended those laws to facilitate community paramedicine programs involving hospitals, home health providers, and primary care physicians.
Designing a Rural Hybrid Care Model
When the nurse practitioner Susan Owen worked at a clinic specializing in diabetes management in Grand Rapids, Michigan, she saw patients from as far away as the Upper Peninsula, six or more hours’ drive away. Last year, Owen joined the startup Homeward Health to try to make care more accessible to rural patients.
Founded in 2022, Homeward Health is implementing a hybrid care model that allows clinical teams to serve seniors who need help managing their health and/or aren’t connected to primary care. In Western Michigan and Minnesota, team members make home visits while also offering same-day telehealth appointments and walk-in and scheduled visits in mobile RVs that travel from town to town.
Many members have said that without Homeward, they won’t get any medical care.
Jeff Anderson
Physician assistant, Homeward Health
Launched in Western Michigan and Minnesota, Homeward Health is serving patients in their homes and via telehealth and mobile clinics. The mobile clinics in retrofitted RVs are stationed in Rite Aid parking lots. Photo courtesy of Homeward Health.
Jeff Anderson, a physician assistant, joined Homeward when he moved back to Michigan after a career in the military, including stints as a medic in remote locations. “I learned to consider all the things that play a role in health, including people’s living conditions and their diet,” he says. Anderson meets with local organizations to identify resources he can tap for his patients, whether they need home modifications, Meals on Wheels, or other supports.
The referenced media source is missing and needs to be re-embedded.
Jeff Anderson, physician assistant for Homeward Health
During a typical home visit, a medical assistant or registered nurse checks patients’ vital signs, home safety, and social needs and, if needed, calls in an advanced practice provider or a physician for advice. “Before I’m meeting a patient for the first time, I’ve read their history, I know the medications,” says Anderson. “But I start by asking about their concerns and what’s important to them. When patients realize this isn’t a typical rushed primary care visit, they may be more comfortable sharing.”
As well as seeing traditional Medicare patients, Homeward partners with Medicare Advantage plans as a full-risk medical provider, meaning it is accountable for the total cost of care for its members. The company stands to benefit if it can help patients avoid hospitalizations or ED visits by better managing chronic issues. To make its hybrid model efficient, Homeward utilizes data scientists to figure out how to deploy staff and where to place mobile clinics.
Lessons for Policy and Practice
As these examples illustrate, there are many opportunities to help rural older adults age well in their communities. Learning from them and making changes to policy and practice could spread promising approaches.
To identify problems and create solutions, advocates should partner with older adults. The Rural Aging Action Network, the age-friendly campaign, and other initiatives are grounded in efforts to understand what matters to older adults. “We’ve seen so many older adults really take to — instead of being asked, ‘How can we help you’ — asking ‘How can you help us?’” says Ashley Washington, M.P.H., senior director of aging initiatives at Lutheran Services of America. “We’re inviting them to be codesigners and partners in this process. They are many times the experts of the communities.”
The National Indian Council on Aging, an advocacy group for American Indian and Alaska Native older adults, offers another model. Its voting and board members are exclusively American Indian or Alaska Native older adults, and their work is grounded in traditions of viewing elders as teachers who can pass on their wisdom to younger generations.
Rural providers need resources and technical assistance. Many rural providers don’t have dedicated quality improvement staff, making it hard for them to implement new approaches. To spread the age-friendly framework, the John A. Hartford Foundation recently awarded a planning grant to the National Rural Health Association to provide technical support and resources for rural communities to improve care for older adults. The association is also developing an age-friendly training curriculum for community health workers, which will be piloted in Texas and then disseminated nationally.
Regulatory changes could enable collaboration.In some cases, antitrust legislation or other rules designed to promote competition can prevent rural providers from working together, which is crucial to sustaining services in rural areas. Advocates say, for example, that adjustments to federal PACE regulations would enable rural hospitals, senior housing providers, area agencies on aging, and others to partner to offer the program in rural communities.
Regulatory and payment changes could also bring home health services to more rural areas. Home health agencies often lack capacity to serve rural patients because of long driving distances, low Medicaid rates, low volume, and workforce shortages. “A state licensing agency can declare a home health shortage area that then allows nurses from rural health clinics to visit homebound patients,” says Pat Justis, M.A., executive director of rural health and health systems quality assurance at the Washington State Department of Health. “But this is rarely used.” Critical access hospitals, too, are disincentivized from operating home health agencies because of their cost-based reimbursement, which excludes the overhead costs of providing home health services in their cost reports for Medicare or Medicaid.
Creative approaches are needed to address workforce shortages. Loan forgiveness programs and training opportunities haven’t substantially grown the number of health care providers in rural communities. Members of the Rural Aging Action Network are trying to mobilize local residents, including volunteers and professionals, but there are limits to this approach, according to Trost of Montana: “We’re trying to tap into the good will of a community. But the good will is just about tapped out.”
To grow the number of paid caregivers, Trost would like to see Montana Medicaid pay family members to care for their elderly relatives. During the COVID-19 public health emergency, 39 states adopted this policy and some states plan to retain it long term. Trost says an organization like his could train caregivers, handle payroll, and offer other supports to help build the pipeline for this crucial workforce. The Administration for Community Living, a federal agency, has also published a national strategy outlining ways in which the federal government and states can support family caregivers. These include hiring caregivers through Medicaid or Medicare Advantage plans and taking steps to identify and meet their health and social needs.
Homeward Health is betting its hybrid care model will help the company recruit clinicians to work in rural areas, including those who are leaving traditional health care jobs out of frustration that their caseloads leave little time to spend with patients.
Health care payers and health systems should invest in what’s been shown to work. Health plans and health care providers involved in value-based payment arrangements stand to benefit from approaches such as home-based primary care or community paramedicine that can improve health outcomes and reduce the costs of caring for older adults. But to make these models workable in rural areas, different policies may be required.
Mindy Fain, M.D., codirector of the University of Arizona Center on Aging, points to drive time as a major pain point. “We need funding for transportation for a provider to get in the car and go 60 miles for one patient visit,” she says. “The value is there — that a home visit can prevent a potentially avoidable ED visit or hospitalization and improve patients’ health and satisfaction with their care.” Fain would also like to see Medicare Advantage plans required to offer home-based primary care to patients who struggle to come into clinics.
EDITORIAL ADVISORY BOARD
Special thanks to the Editorial Advisory Board for their help with this article.
Melinda Abrams, M.S., Commonwealth Fund
Katrina Armstrong, M.D., Columbia University Vagelos College of Physicians and Surgeons
Lynn Barr, M.P.H., Barr-Campbell Family Foundation
Melissa Lackey, M.S.N., Texas A&M Rural and Community Health Institute
Harold Miller, Center for Healthcare Quality & Payment Reform
Alan Morgan, M.P.A., National Rural Health Association
John Supplitt, M.P.A., M.B.A., American Hospital Association
Henry Weil, M.D., Bassett Healthcare Network
Publication Details
Date
Contact
Martha Hostetter, Consulting Writer and Editor, Pear Tree Communications
Martha Hostetter and Sarah Klein, “Helping Older Adults Age Well in Rural America,” feature article, Commonwealth Fund, Nov. 9, 2023. https://doi.org/10.26099/tkph-e882