An Enticing Offer: How Some Rural Communities Are Winning the Competition for New Clinicians
Lincoln Health Community Hospital in Hugo, Colo., on October 23, 2024. As America’s aging population demands greater access to care, several states are making efforts to recruit and retain clinicians in rural areas. Photo: Aaron Ontiveroz/Denver Post via Getty Images
Lincoln Health Community Hospital in Hugo, Colo., on October 23, 2024. As America’s aging population demands greater access to care, several states are making efforts to recruit and retain clinicians in rural areas. Photo: Aaron Ontiveroz/Denver Post via Getty Images
Toplines
Rural communities rely more heavily than urban communities on primary care doctors, who are in increasingly short supply
As America’s aging population demands greater access to care, several states are making efforts to recruit and retain clinicians in rural areas
Toplines
Rural communities rely more heavily than urban communities on primary care doctors, who are in increasingly short supply
As America’s aging population demands greater access to care, several states are making efforts to recruit and retain clinicians in rural areas
The article is part of a partnership between the Commonwealth Fund and the Bassett Research Institute in Cooperstown, N.Y., to explore innovative approaches to the health care challenges facing rural communities across the United States.
At least one-third of the physician workforce in the United States is expected to retire over the next decade, just as demand for care among older Americans soars. While all areas of medicine will be affected, two important specialties — primary care1 and psychiatry — will be particularly hard hit. Together, they account for more than 40 percent of physicians nearing retirement age. Without a significant influx of nurse practitioners and physician assistants, there won’t be enough new physicians entering the workforce to meet demand.
If the impending shortages become a hardship for city dwellers, they’ll be even more problematic for residents of rural areas, who have long struggled with limited access to all types of providers. Workforce experts are predicting that by 2030, rural communities will have only one-third as many physicians per capita as urban areas (9.4 vs. 29.6 physicians per 10,000 population). Shifting workforce demographics are a critical factor: urban doctors are typically younger than rural ones and have more years of work ahead. The disparity also reflects the nation’s entrenched practice of training medical students and residents in cities where they establish social and professional ties that can be hard to uproot.
To succeed at recruiting and retaining clinicians in an ever more competitive market, some communities are making the case that rural practice can restore what’s been lost in modern medicine, with its emphasis on documentation, short medical visits, and bureaucratic oversight. The perks aren’t limited to having greater autonomy or exerting influence over hospital management and public health. It’s also the chance to develop the types of relationships with patients that drew many doctors to medicine in the first place. To counter concerns that new hires may feel professionally isolated in a small community, some rural employers are creating new ways for them to stay connected to their peers through training and teaching opportunities. This piece showcases several potentially replicable strategies for attracting doctors to rural areas.
No one made me practice in a rural community for 20 years. I did that by choice because it’s some of the most rewarding medicine that there is. You become a pillar in the community and have to know what you’re doing because access to specialty care is often limited.
Sarah Chouinard, MD
Chief medical officer of Nashville-based Main Street Health, which helps patients navigate the health care system and offers support services to rural physicians
Leveraging Relationships to Promote Retention
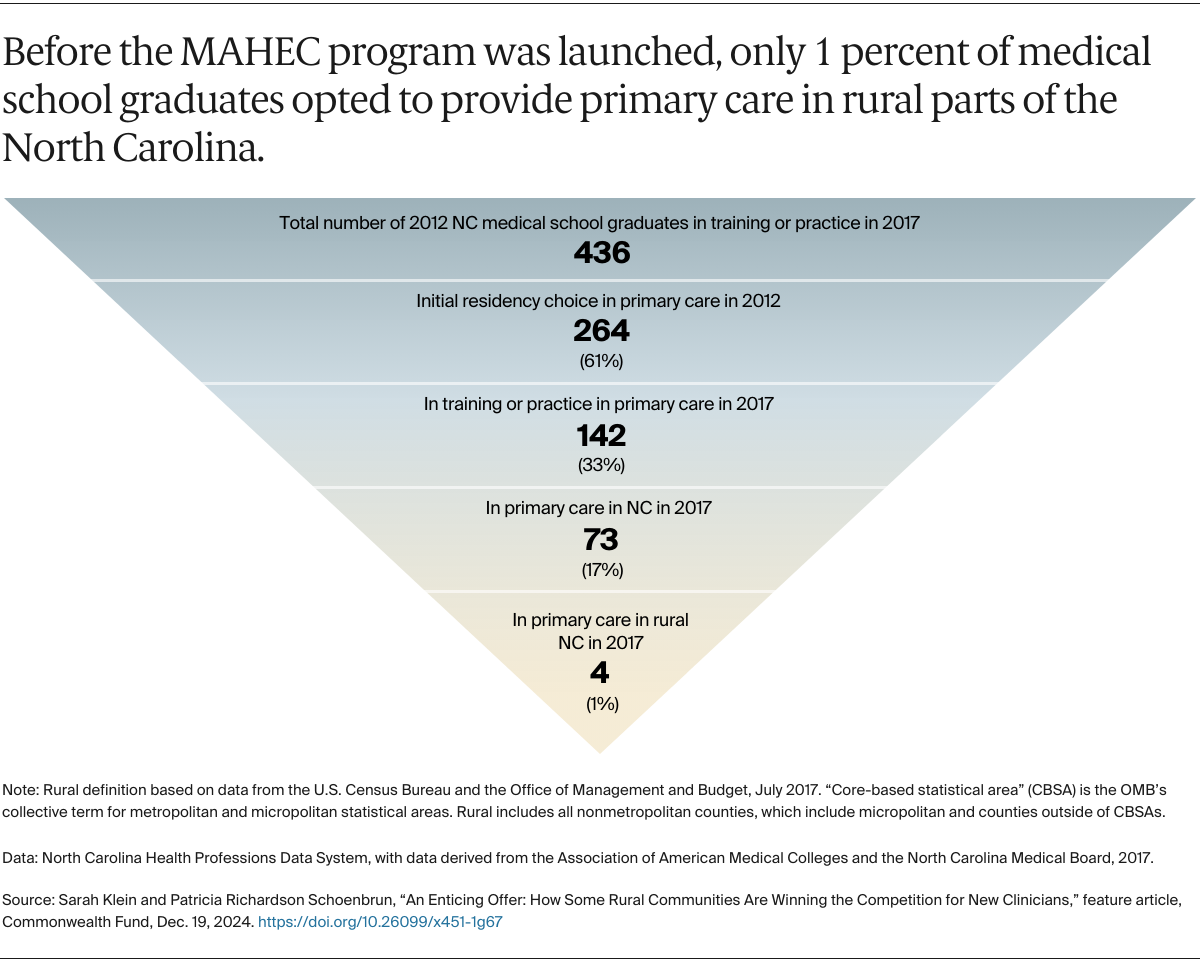
North Carolina is made up of hundreds of small towns clustered in and around scenic mountain ranges, with a full third of the state’s population living in communities of fewer than 10,000 residents. Increasing access to primary care in these remote areas — some of which were hard to reach even before Hurricane Helene wiped out roads, electricity, and cell service — has long been a state priority. The state’s strategy for filling workforce gaps is built on a large body of evidence that medical students and residents who have grown up in or spend time in rural areas are significantly more likely to practice there. The state funds nine area health education centers, which are tasked with recruiting, training, and retaining a workforce to meet the needs of rural and other underserved communities. These centers manage more than two dozen residency programs that bring trainees from academic medical centers, like the Duke University School of Medicine and the University of North Carolina School of Medicine, into small communities. They also create opportunities for precollege students to learn about health care careers.
Among these centers, the Mountain Area Health Education Center (MAHEC) in Asheville, N.C., has developed a particularly robust approach to serving the state’s 16 westernmost counties. It built its training program by anticipating the challenges people with an interest in rural medicine will face and offering them supports at each step along the way, primarily through mentors and preceptors who can counter the dominant narrative that becoming a high-earning specialist in an urban center is the path to professional satisfaction. Benjamin Gilmer, MD, the medical director of MAHEC’s Rural Health Initiative and a primary care physician in Fletcher, N.C., a town of 8,106, says MAHEC’s “alpha to omega” approach begins with persuading promising students in rural communities that they have what it takes to become a doctor. It culminates in a unique fellowship that serves as a bridge between residency training and the first year of practice in a rural area.
Part of the secret sauce is exposing students to really amazing rural preceptors — the type of doctors others aspire to be. If you can’t do that, the game is lost.
Benjamin Gilmer, MD
Medical director of Mountain Area Health Education Center’s Rural Health Initiative
The fellowship allows new doctors to retain the best aspects of residency — access to mentorship, training, and a cohort of peers — while they adjust to the challenges of caring for patients who often have more chronic disease and fewer financial resources. Fellows entering the program negotiate a full-time salary with their employer — typically around $200,000 a year for a primary care physician working for a local hospital or clinic. MAHEC then assumes 20 percent of the cost for one year, enabling the fellows to devote a full day each week to personal and professional development. The seven fellows in each year’s cohort come together for in-person retreats and monthly trainings, which include sharing the results of projects they’ve taken on with the extra time. Gilmer says many have launched new programs that bring much-needed services to their communities, including clinical pharmacy consults for patients with chronic disease, medication-assisted treatment for opioid use disorder, and hepatitis C treatments.
Current fellows, past graduates, and medical residents were among the first responders after the recent hurricane. They staffed makeshift clinics that have helped to ensure people displaced from water-damaged nursing homes and hospitals have access to critical supplies and services, including oxygen, dialysis, and medications for opioid use disorder. Bryan Hodge, DO, MAHEC’s chief academic officer, says their commitment to the area is a testament to place-based training programs. “We’re demonstrating it’s possible to meet community needs and educate a workforce at the same time,” he says.
While the program isn’t cheap — it costs around $315,000 annually — it gets results. Of the 31 fellows who completed the program since it was launched in 2017, 90 percent have remained in western North Carolina. “The benchmark for rural retention is about 25 percent,” Gilmer says. Rural health systems gain staff who are continually updating their skills; they’re also building a cadre of clinicians willing to serve as preceptors for future medical students and residents. MAHEC plans to expand the number of fellows from seven to 10 in the coming years with funding from a local philanthropy. “We think it has potential as a national model,” Gilmer says.
Benjamin Gilmer, MD and Olivia Caron, PharmD, from MAHEC helped staff a makeshift clinic in Swannanoa, N.C., that served more than 700 patients impacted by Hurricane Helene.
Responding to New Hires’ Concerns
It was the prospect of practicing with independence that drew Kimberly Becher, MD, to Clay, W.Va., an Appalachian town with a population of 330. Becher arrived in 2014, a year before the town’s only grocery store closed. She’d gone to medical school and residency two hours away at Marshall University in Huntington, W.Va., a medical school that encourages trainees to rotate through rural communities and immerse themselves in local culture.
Kimberly Becher, MD, Chief medical officer, Community Care of West Virginia
Becher opted to join Community Care of West Virginia, a federally qualified health center that now has 18 clinics and 50 school-based health sites in the central part of the state, because she liked its leaders’ willingness to experiment with new care models and their commitment to reducing health disparities between urban and rural areas, including high rates of thyroid cancer. “There just wasn’t a fear of trying new things, and that was what was most important to me,” Becher shared.
This flexibility was part of Community Care’s hiring strategy. Back in 2012, the health center was struggling to recruit physiciansto rural West Virginia because of the mounting opioid crisis. Some worried about being swept up in prosecutions related to opioid prescribing. To address their concerns, the health center developed a multidisciplinary pain management program that screened patients for addiction risk and offered those affected a range of supports, including behavioral health services. Patients were required to sign compacts agreeing to urine drug screens and random pill counts to ensure opioid painkillers were not being diverted. Potential hires took note.
The health center supports rural providers and community programs by leveraging funding from the 340b Drug Pricing Program. Established by Congress in 1992, it allows safety-net providers to purchase pharmaceuticals at discounted rates while billing insurance at market rates, using the proceeds to fund essential services. In this way, Community Care has been able to pay for community health workers and navigators, who help clinicians address the many issues that rural residents living in poverty face.
Even though Becher grew up in a small town, the deprivation she witnessed in exam rooms startled her — patients struggling with homelessness and hunger, problems that were exacerbated when the town’s only grocery store closed. While patients’ struggles are sometimes hard to hear, she says the transparency makes her more effective as a doctor. “You understand why that person is the way they are. You understand what their support system is and isn’t and you’re able to close loops better,” she explains. “There’s just tons of professional goodness that comes out of that.”
That up-close view presented challenges for Becher during the pandemic when some patients rejected her advice about masking and vaccinations. The resulting frustration she felt took a physical toll on her heart, forcing her to cut back hours while she learned more constructive ways to channel her stress. This experience shaped her approach when she later took on the role of chief medical officer, a job that puts her in charge of recruiting and retaining other clinicians. When a recent candidate nervously asked about vacation time, saying work–life balance was important to him, Becher reassured him: “I said, ‘You’re not going to upset me by saying that. No one is going to be a better advocate for you as a provider than me.’”
While the health sector has experienced a period of massive turnover since 2018, Community Care has retained 93 percent of its physicians and advanced practice providers.
People underestimate the impact they can have in a rural community.
Kimberly Becher, MD
Chief medical officer for Community Care of West Virginia
Leaning into Hometown Hospitality
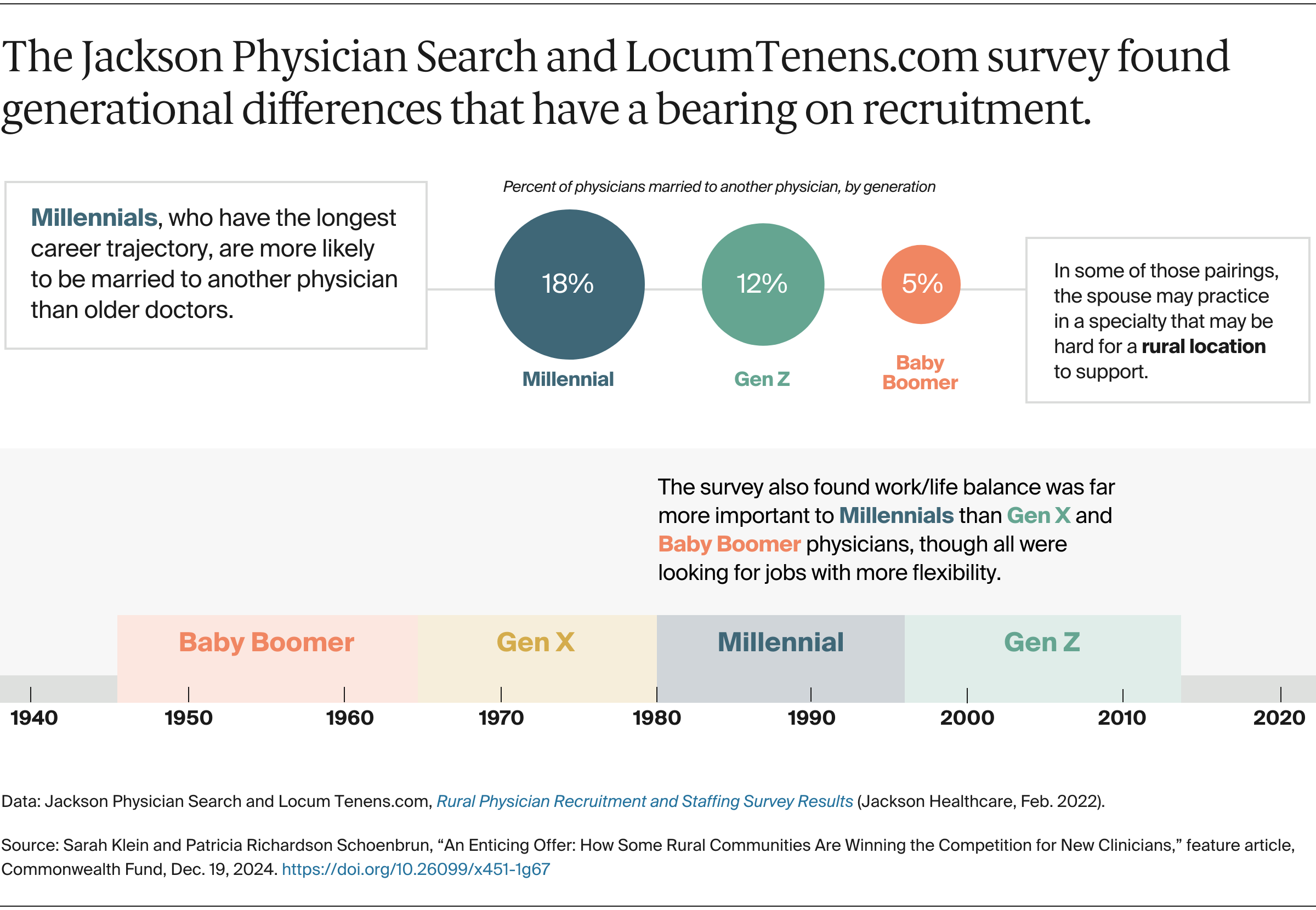
Recognizing the impact physician retirements will have in rural communities, Jackson Physician Search, a national recruiting firm headquartered in Alpharetta, Ga., joined the temporary staffing firm LocumTenens.com in surveying 1,500 U.S. physicians and advanced practice providers to gauge their interest in rural practice. The firm found physicians who were already working in rural markets were more fulfilled than their urban and suburban counterparts (27% vs. 20% and 21%) and that a significant share of urban and suburban doctors (90%) were willing to consider practicing in a rural area, especially if it meant higher compensation or a better work–life balance.
To win them over, Neal Waters, a regional vice president, advises his clients at rural hospitals and clinics to play to their strengths, which include pivoting more quickly in tailoring a job to a recruit’s interests. “They are maneuvering a speed boat as opposed to a cruise ship,” he explained. This flexibility recently paid off at one rural hospital in Iowa that was able to recruit three family medicine physicians in a single month. All three were interested in obstetrics but lacked formalized training to deliver babies by cesarean section. In response, the hospital asked its ob/gyn to serve as their mentor, an arrangement he enthusiastically agreed to.
Neal Waters, Regional vice president, Jackson Physician Search
Waters also encourages employers to be attentive to things that matter to job candidates’ families: “One of the biggest reasons for turnover in rural communities is that people never felt included or integrated into the community. They say, ‘The job was great, but my wife or my husband, or my kids never made friends or weren’t happy.’”
Instead of leaving it to potential hires to find housing and explore the area, his clients develop meticulously tailored itineraries that include introductions to local book clubs and high school swim coaches. One hospital board member even invited a prospect’s family to stay at his house during a site visit and offered to babysit their children while the family toured the area.
Promoting Residency Programs in Rural Communities
While these efforts have resulted in new hires for rural hospitals and clinics, it will likely take more seismic changes in medical training to close the workforce gap between urban and rural markets. Only 2 percent of Medicare-funded residency training occurs in rural communities. The federal Health Resources and Services Administration has sought to rectify the imbalance by providing funding to launch residency programs in rural hospitals and community clinics in underserved areas. These programs and rotations are crucial for developing the competencies needed to flourish in rural practice, including the delicate balance of managing privacy concerns when caring for neighbors.
The irony is that, in many respects, rural communities may be a superior training ground for some specialties, such as family medicine, as training there often involves following patients across multiple care settings without relying on specialist support. This versatility is part of the reason many academic medical centers turned to rural doctors to launch family medicine residency programs in the early 1970s. Subsequent research has shown that family medicine physicians trained in rural areas reported having a wide scope of practice compared to their urban counterparts and a greater sense of self-efficacy.
Gundersen Health System in La Crosse, Wis., which manages six critical access hospitals in a tristate region, designed its general surgery residency program with rural communities in mind. General surgeons are critically needed in rural areas to respond to emergencies, including car accidents, and to deliver services like colonoscopies, C-sections, and cancer resections for people who are unable or unwilling to travel to urban centers for care. “I don’t think people appreciate how important staying in your own community is for our rural patients, particularly for people who don’t want to leave their farm unattended or be far from their family or pastor when they are sick,” says Stephen Shapiro, MD, a general surgeon and president of Gundersen Medical Foundation, which provides funding support for the program.
As one of just 18 general surgery residencies with a rural focus, the program prepares trainees for the diverse array of surgical procedures they will perform in rural areas. According to program director Melissa K. Johnson, MD, two-thirds of the program’s graduates directly enter general surgery practice immediately after residency, rather than pursuing subspecialty fellowship training — in stark contrast to urban programs, where only 20 percent choose this path. One-third work in communities with fewer than 50,000 people.
In addition to expanding access to care, these programs have an important role to play in sustaining rural hospitals; general surgeons alone account for as much as 40 percent of a hospital’s revenue. “The loss of a surgeon is very predictive of the loss of a hospital,” says Robert L. Phillips, Jr., MD, MSPH, executive director of the Center for Professionalism and Value, an affiliate of the American Board of Family Medicine. The center is completing a study of how the presence — or loss — of a family physician–general surgeon dyad impacts health outcomes and hospital closures in rural communities. Phillips says such dyads can meet a wide range of community needs, including increasing access to maternity care, but are disappearing at a faster rate than they are being replaced because of retirements and other factors. To reverse this trend, rural programs that train these specialties together could strengthen both rural health care and the financial sustainability of rural hospitals.
Keeping a Closer Eye on Changing Market Conditions
Hospital closures, mergers and acquisitions, and the entry of private equity–backed companies in rural communities may also reshape the employment landscape. Companies like Main Street Health are deploying navigators to help clinicians practicing in small communities so they can succeed operating under value-based contracts. But it’s unclear if changes in the ownership of practices and hospitals more broadly will make it harder to find people to oversee rural training.
“If you are paid by production, it may be hard to devote time to developing a new generation of clinicians,” says C. Holly Andrilla, MS, deputy director of the WWAMI Rural Health Research Center at the University of Washington.
Leaning In to Promising Approaches
One common denominator of the programs featured here is their ability to identify and address vulnerabilities in the workforce pipeline. Many solutions focus on building a sense of community that may be more appealing than money to some job candidates. They are also finding cost-effective ways to help geographically dispersed staff feel connected. When Randy Longenecker, MD, ran a residency program in rural Ohio, he organized weekly gatherings that brought trainees together with other staff to discuss the unique features of rural practice. “We’d talk about how to manage living in a community where your neighbor is also your kid’s soccer coach and you also delivered their baby,” he says.
Melody Le Tran-Reina, MD, who directs the Rural Program in Medical Education at University of California, Davis, School of Medicine, adopted a similar approach for medical students who reported not feeling welcome in rural communities when they did clerkships. “Having a small cohort of like-minded peers and having access to mentors and faculty helps to create a sense of community. It really helps students process these experiences,” she says.
These innovative programs show what’s possible when relationships and community connections are prioritized. The Mountain Area Health Education Center’s Gilmer would like to see even greater support for students who want to work in rural areas. “To move the needle, we need medical schools to prioritize admissions of people who are committed to rural practice.” The evidence suggests he’s right: by providing the right combination of professional opportunity, peer support, and community integration, rural employers can successfully compete for the next generation of clinicians.
Editorial Advisory Board
Melinda Abrams, MS, Commonwealth Fund
Katrina Armstrong, MD, Columbia University Vagelos College of Physicians and Surgeons
Lynn Barr, MPH, Barr-Campbell Family Foundation
Melissa Lackey, MSN, Texas A&M Rural and Community Health Institute
Harold Miller, Center for Healthcare Quality & Payment Reform
Alan Morgan, MPA, National Rural Health Association
John Supplitt, MPA, MBA, American Hospital Association
Henry Weil, MD, Bassett Healthcare Network
NOTES
The primary care designation includes the specialties of internal medicine, family practice, pediatrics, and obstetrics/gynecology. ↩
Sarah Klein and Patricia Richardson Schoenbrun, “An Enticing Offer: How Some Rural Communities Are Winning the Competition for New Clinicians,” feature article, Commonwealth Fund, Dec. 19, 2024. https://doi.org/10.26099/x451-1g67