Introduction
Whether it’s stubbornness, an aversion to appearing weak or vulnerable, or other reasons, men go to the doctor far less than women do.1 While behavioral and cultural norms may have a lot to do with the care-seeking habits of American men, the fact remains that the United States is the only high-income country that does not ensure all its residents have access to affordable health care. Roughly 16 million U.S. men are without health insurance, and affordability is the reason that people most often cite for why they do not enroll in a health plan.2 Do income level and financial stress help explain why men do not get needed care and experience worse health outcomes?
Using data from the Commonwealth Fund’s 2020 International Health Policy Survey and the Organisation for Economic Co-operation and Development (OECD), we compare health care accessibility, affordability, and health status for adult men in 11 high-income countries. We also examine measures of income and income-related stress, where the data allow, to understand the role income insecurity might play in American men’s relatively low use of health care. (See “How We Conducted This Study” for further details on our methods.)
Highlights
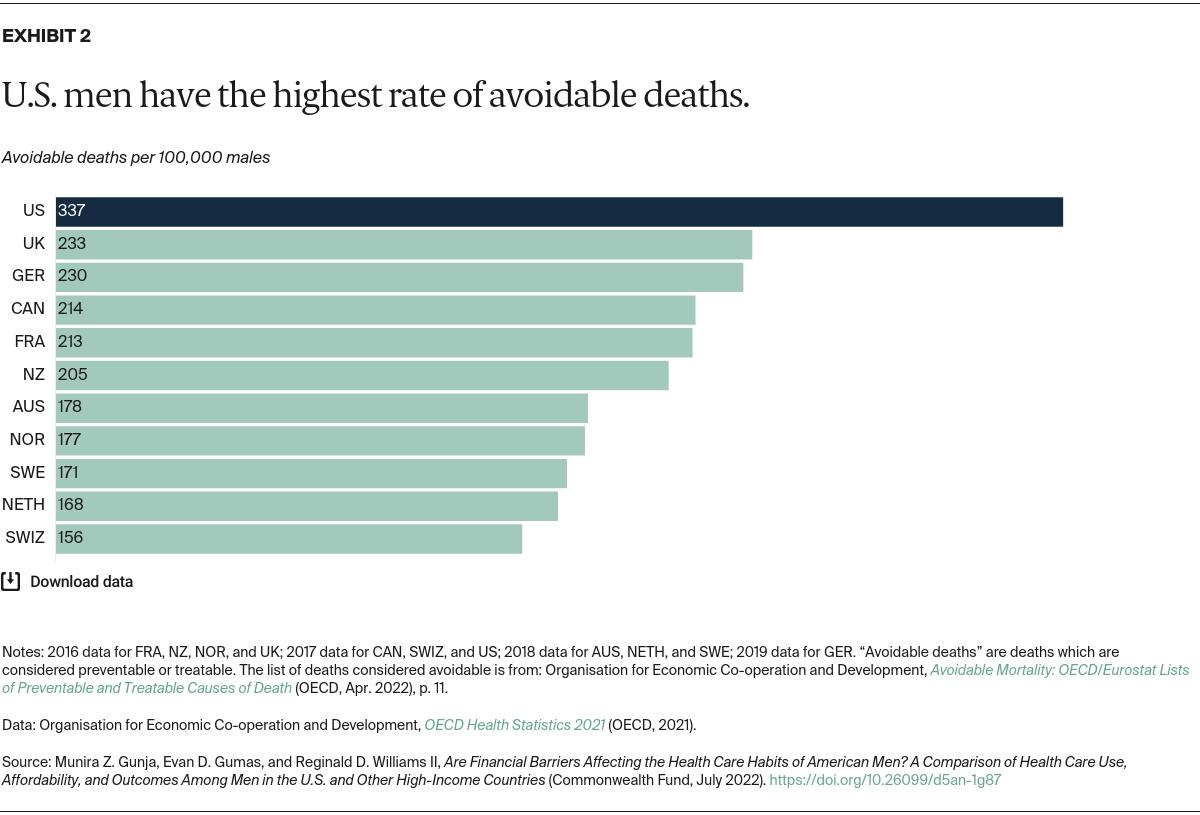
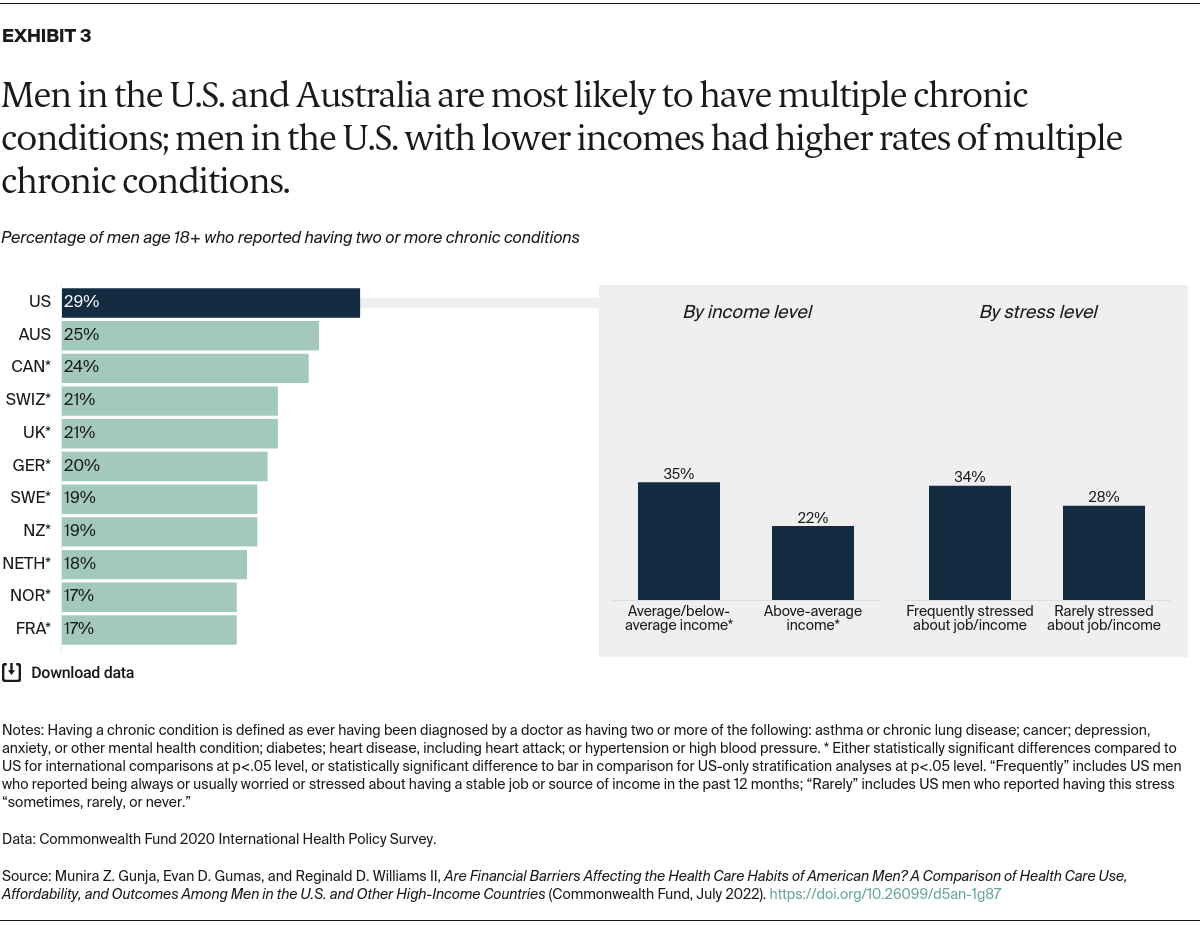
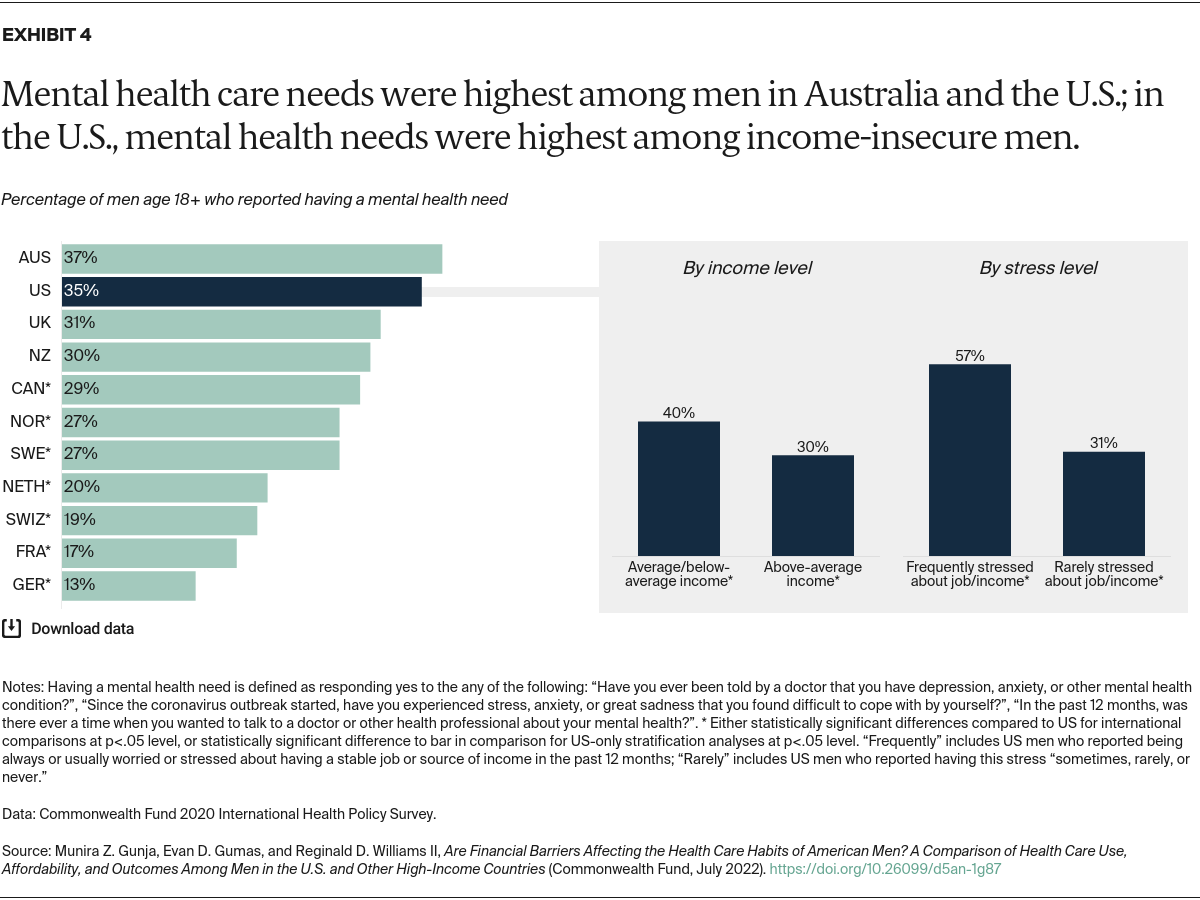
- Looking across the 11 high-income countries in our study, rates of avoidable deaths, chronic conditions, and mental health needs for U.S. men are among the highest in our analysis.
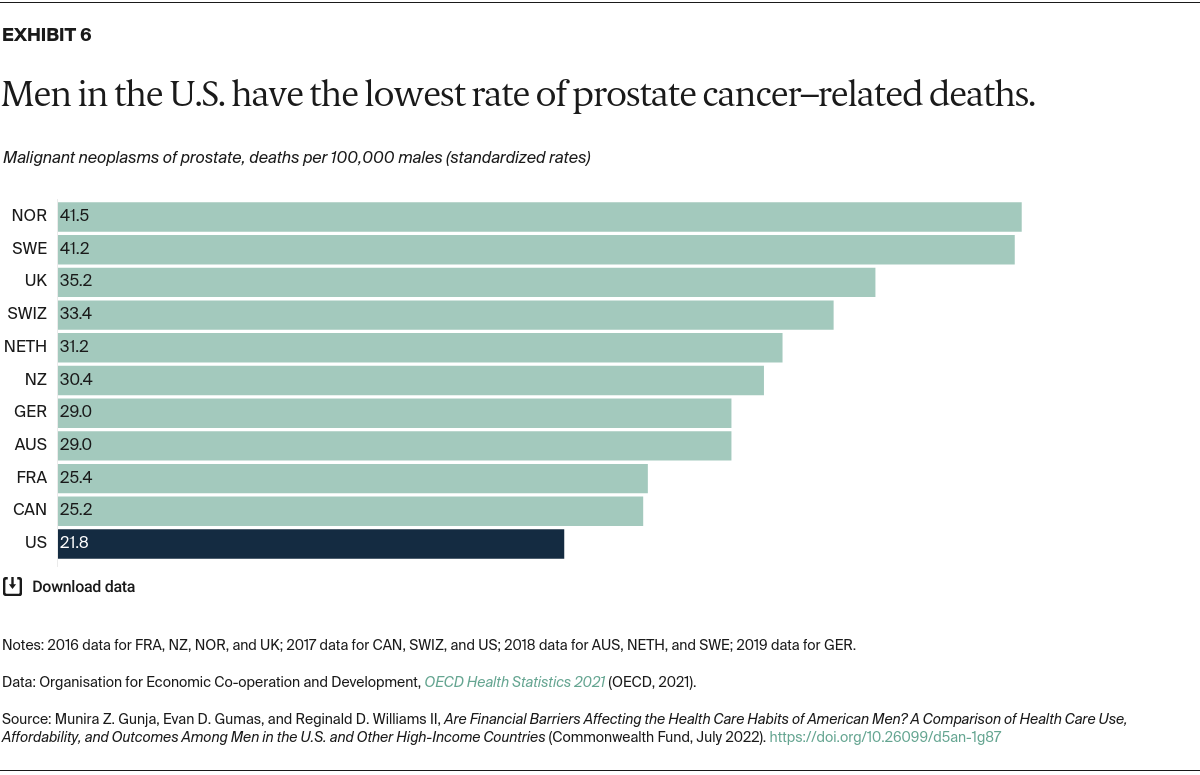
- Men in the U.S. have the lowest rate of prostate cancer–related deaths.
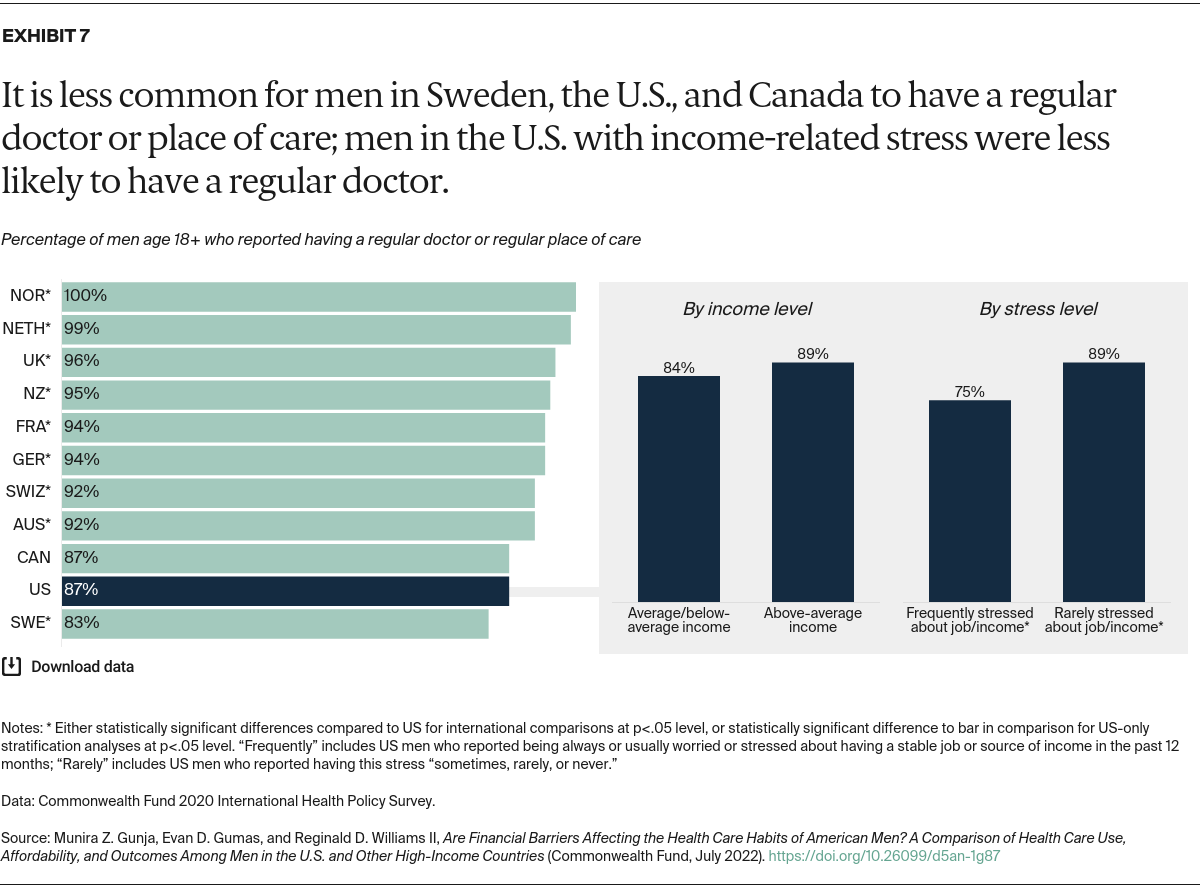
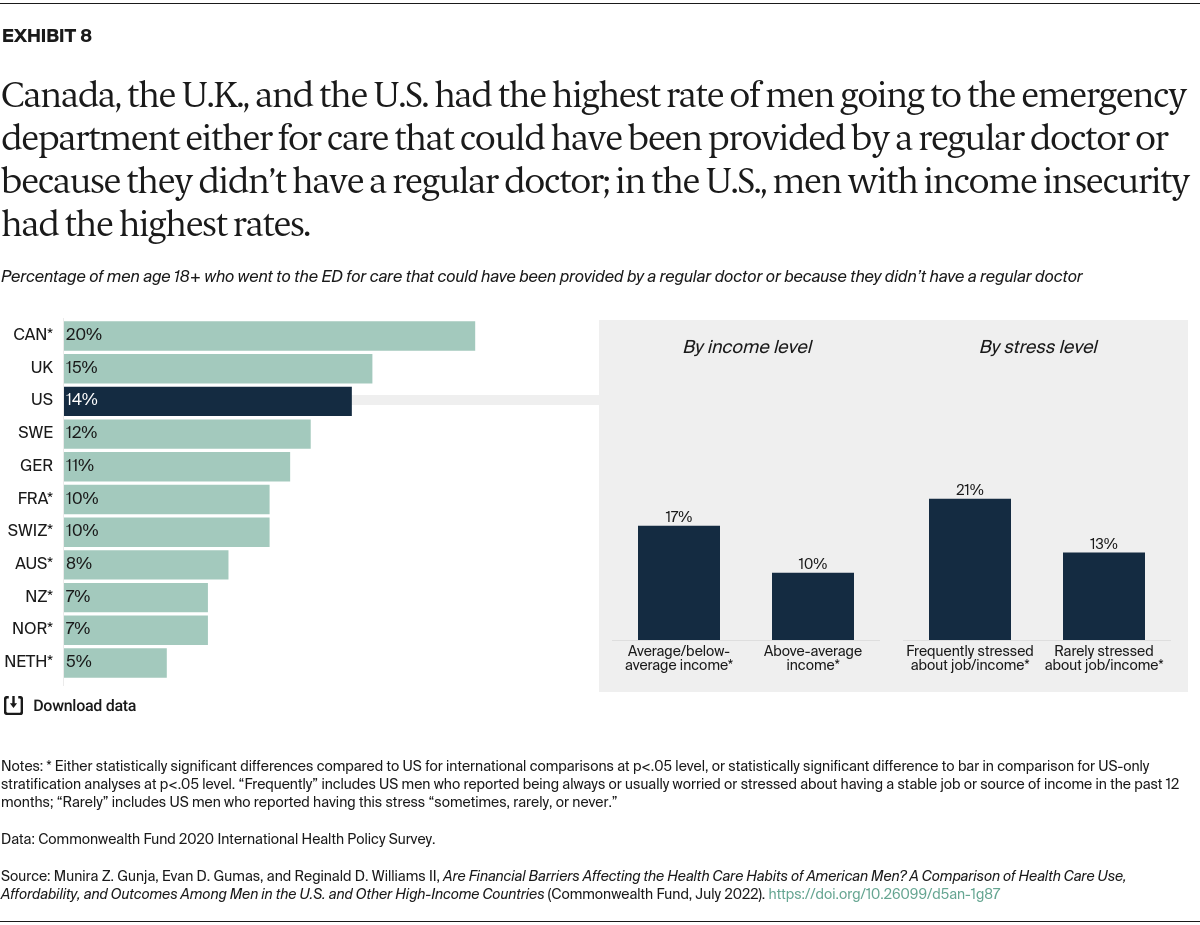
- Men in Canada, the United States, and Sweden are the least likely to have a regular doctor and have among the highest rates of emergency department use for conditions that could have been treated in a doctor’s office.
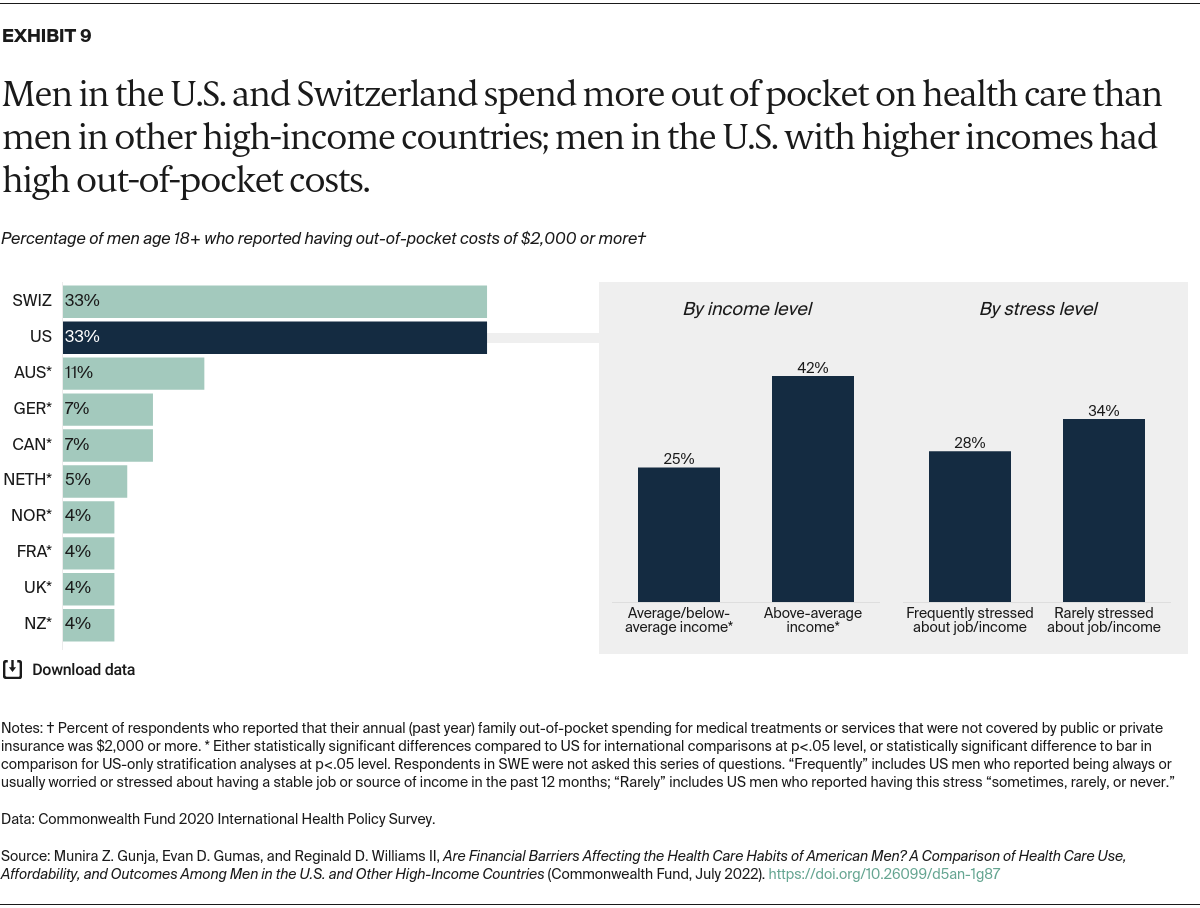
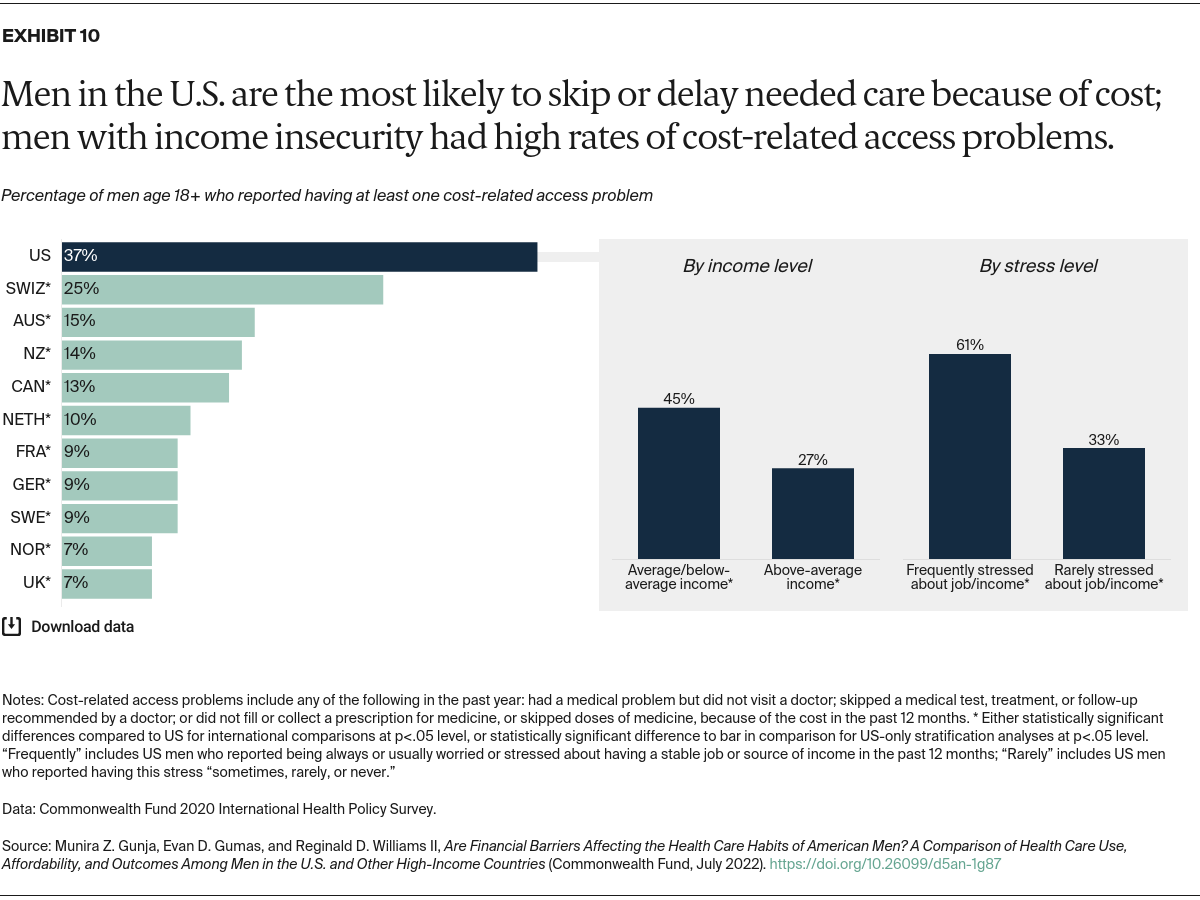
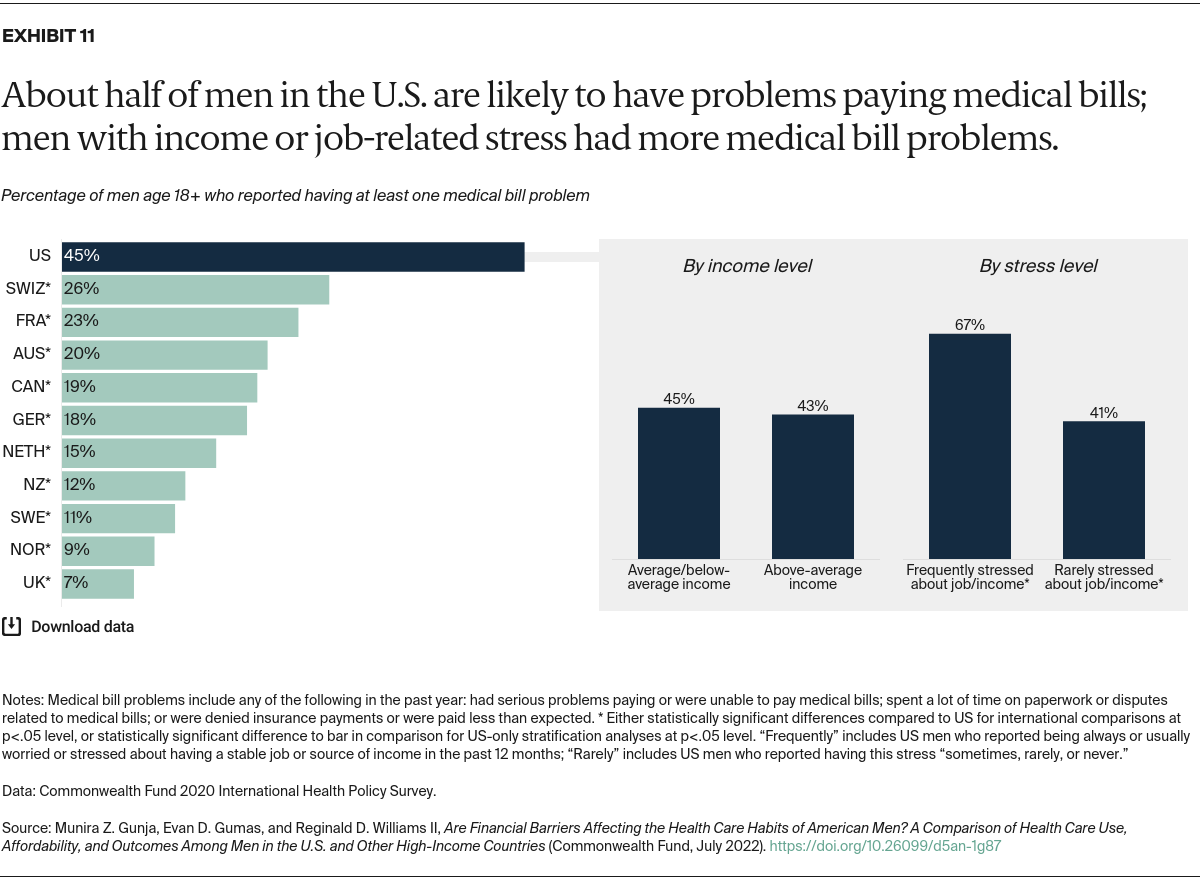
- Men in the U.S. and Switzerland skip needed care because of costs and incur medical bills at the highest rates.
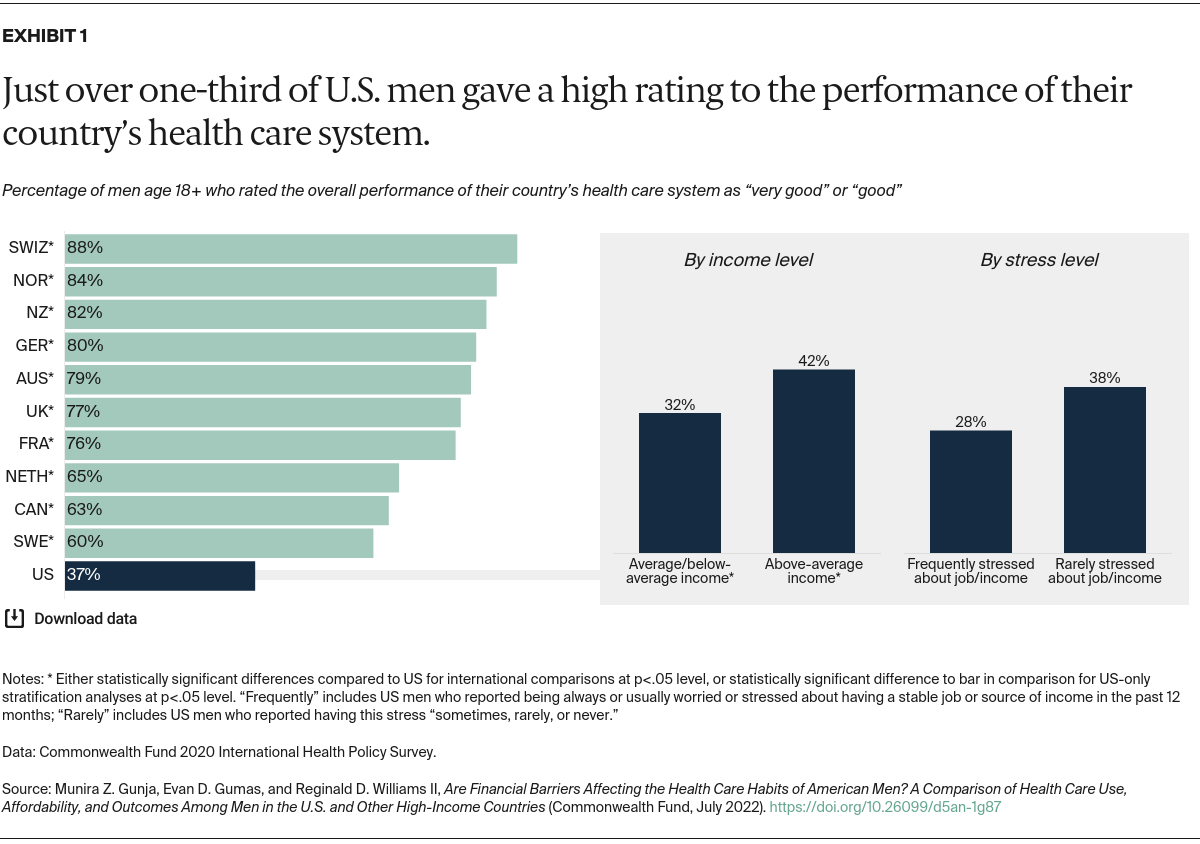
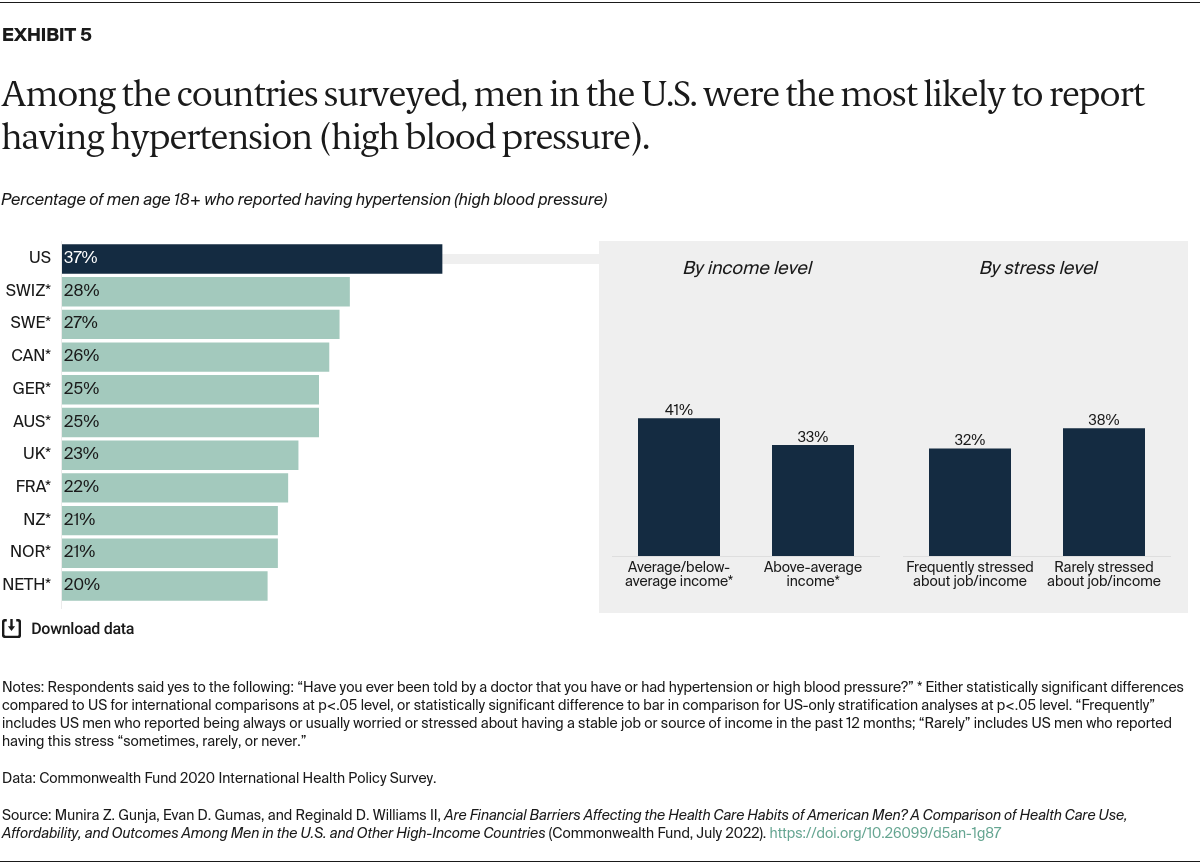
- In the U.S., men with lower income or frequent financial stress are less likely to get preventive care, more likely to have problems affording their care, and more likely to have physical and mental health conditions.