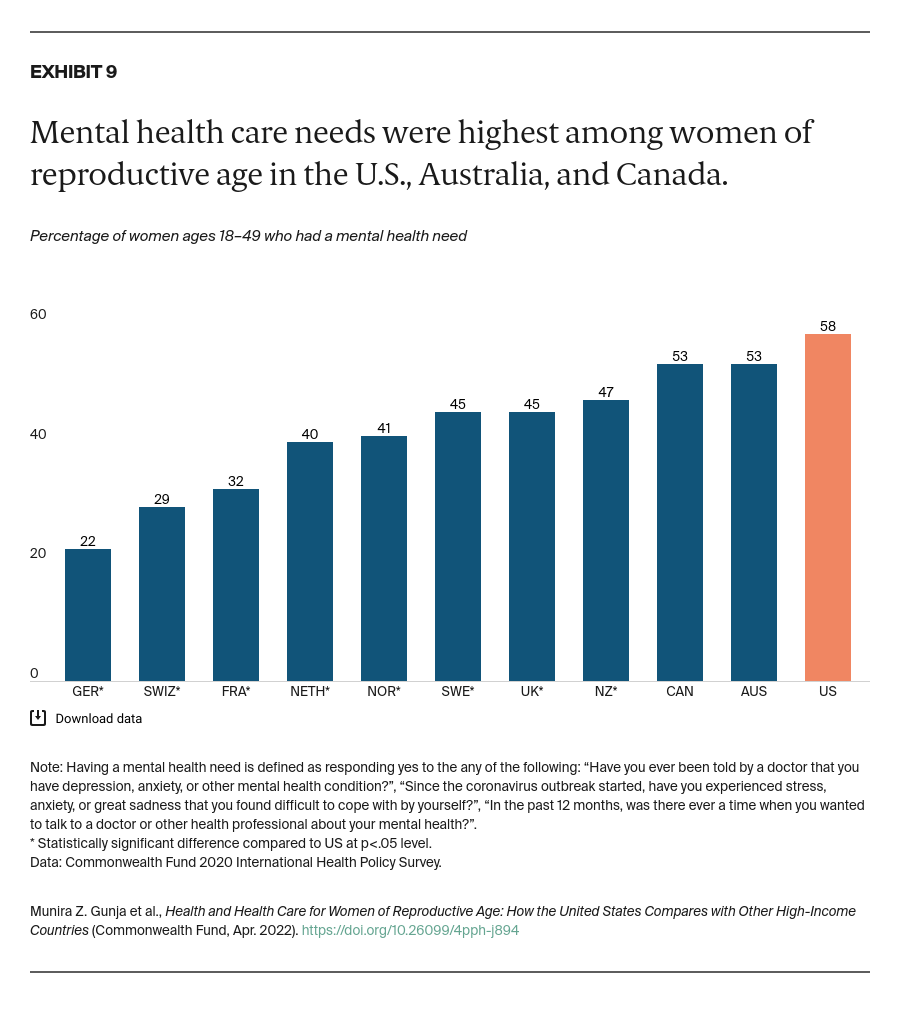
Women in each country answered a series of questions regarding their mental health at the start of the COVID-19 pandemic, when the survey was conducted. They were asked about being diagnosed with a mental health condition; experiencing stress, sadness, or anxiety that was difficult to cope with on their own; or wanting to talk to a mental health professional in the past year.
Since the pandemic began, rates of mental health conditions have risen globally.11 Our survey found that women of reproductive age in Canada, Australia, and the U.S. were the most likely to report having a mental health care need. Women in Germany were the least likely.
Discussion
Research shows that investing in women’s health results in a healthier overall population, healthier future generations, and greater social and economic benefits.12 Yet the U.S. remains the only wealthy country without universal health care, leaving about 10 million women without insurance.13
Other countries have made substantial efforts to ensure women are able to get needed primary care as well as maternal and mental health care. There are a number of steps U.S. policymakers can take to substantially improve health and wellness for women of reproductive age.
Ensure all women have access to affordable health care.
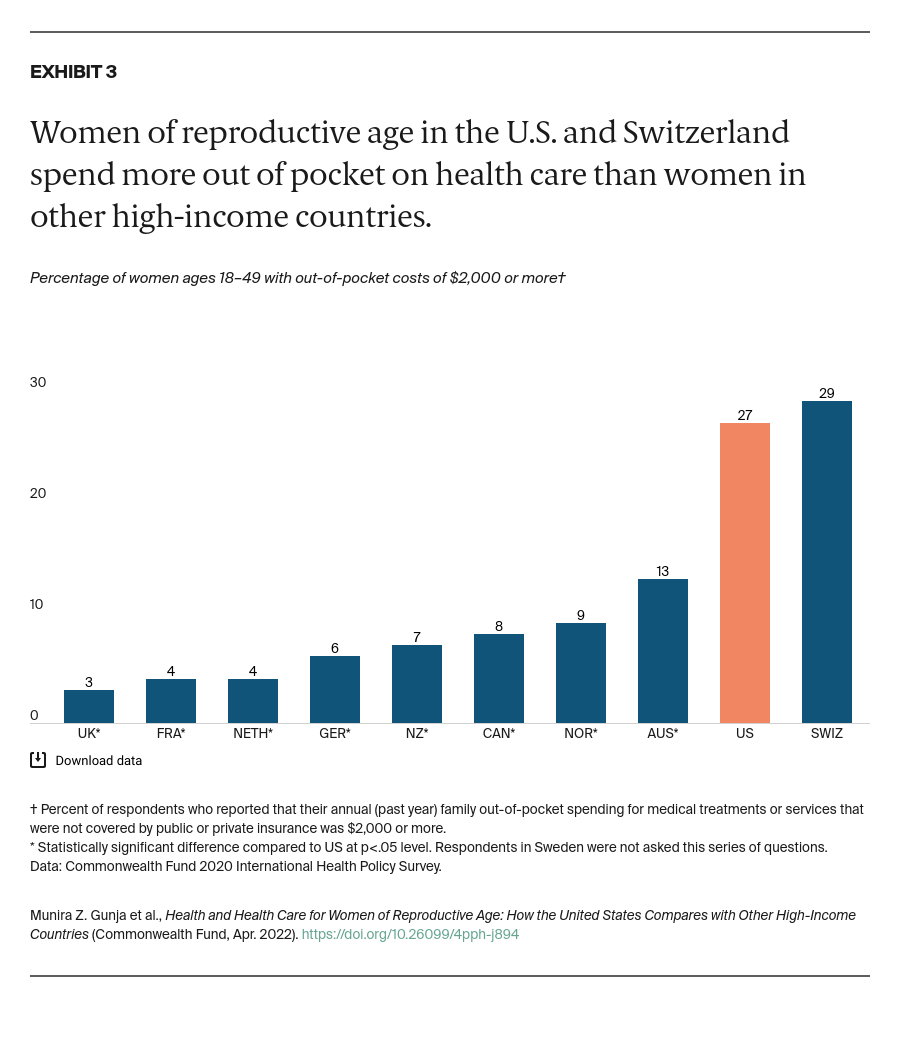
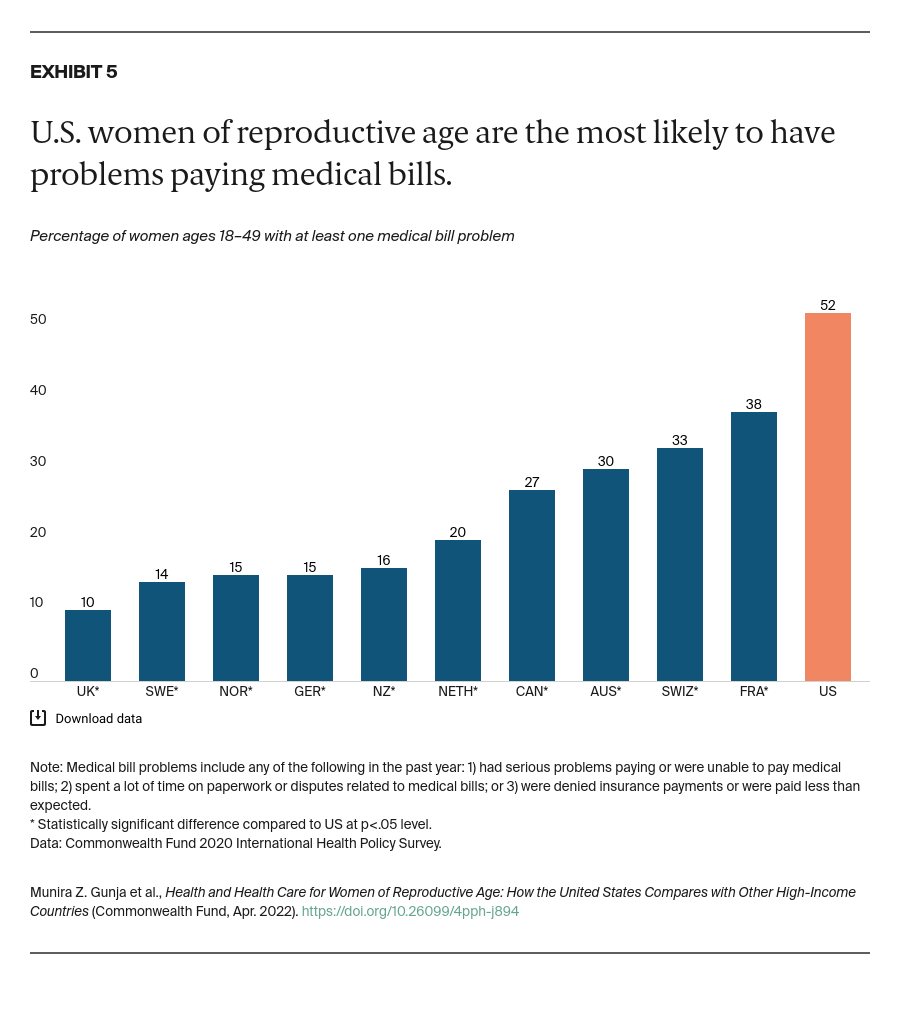
Primary care. Although the Affordable Care Act (ACA) did away with cost sharing for preventive services like wellness visits, immunizations, and screenings, U.S. women still can face high out-of-pocket costs for other care. In other countries, women do not face these high out-of-pocket costs. For example, Canada, Germany, the Netherlands, and the U.K. impose no cost sharing for primary care visits.14 U.S. policymakers could extend affordable and comprehensive primary care to all women by expanding on the ACA’s reforms, such as enhancing marketplace plan subsidies and providing coverage for those who fall in the “Medicaid coverage gap.”15
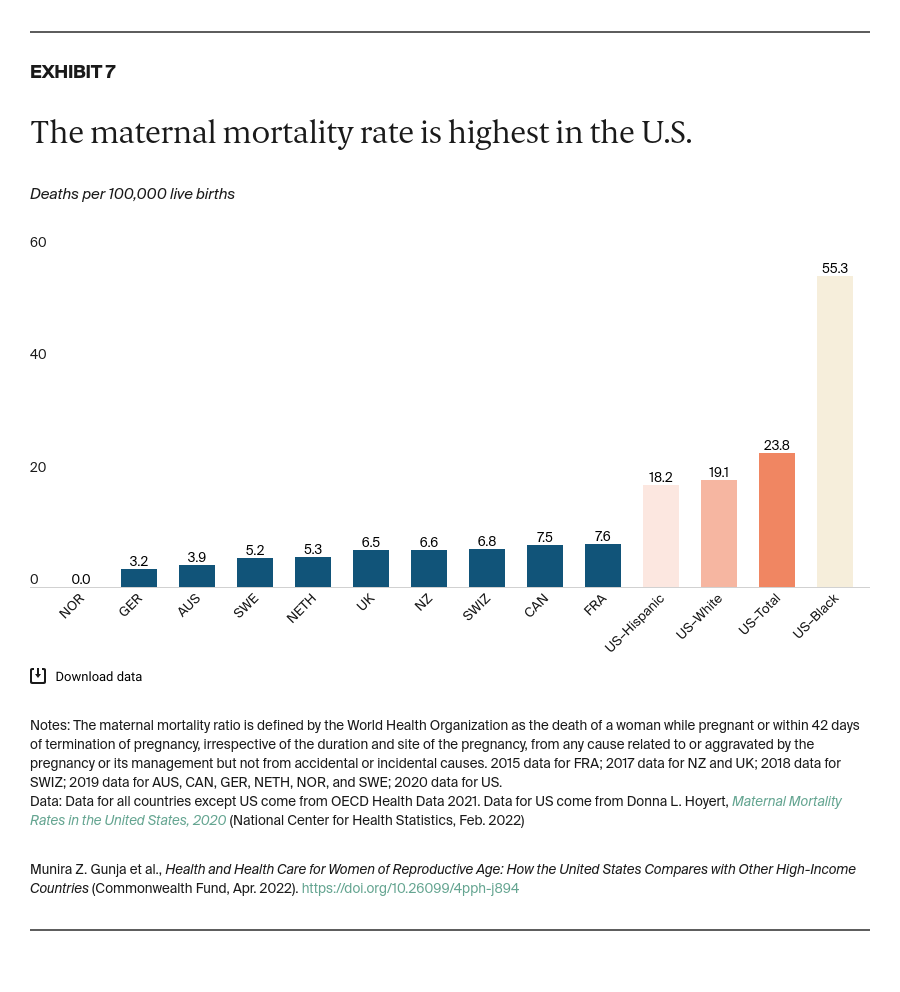
Maternal care. In the U.S., many women have high out-of-pocket payments for maternity care, even if they are insured, in the form of copays and deductibles. The types of maternity services that insurers cover are limited, too. For example, pregnancy-related Medicaid coverage lasts only 60 days postpartum. Maternal care, including postpartum care, is free in most of the countries we studied and includes home visits by a nurse.16 U.S. policymakers have an opportunity to encourage all states to extend Medicaid coverage to a minimum of 12 months postpartum, as well as to expand implementation of federal guidelines for coverage of women’s preventive services without cost-sharing to encompass all women, including those enrolled in traditional Medicaid.
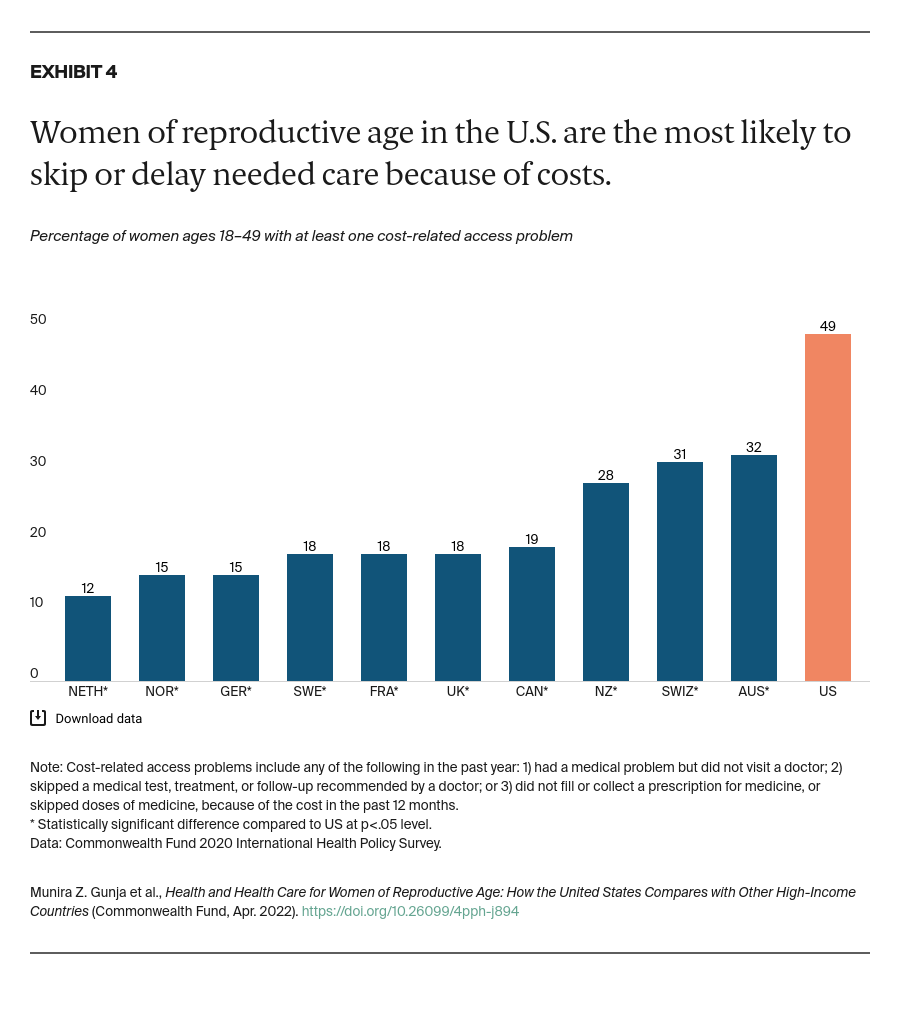
Mental health care. Despite having the highest rate of mental health care needs, women in the U.S. are more likely to report skipping needed care, including mental health care, for cost reasons than women in the other 10 countries. Other nations have made mental health care more affordable in recent years. France waives all copays for care related to long-term chronic mental illnesses.17 In response to COVID-19, Australia is covering additional subsidized therapy sessions provided by psychologists, psychiatrists, general practitioners, and other clinicians.18 At a minimum, U.S. policymakers could extend the ACA’s requirement to cover essential health benefits, including mental health care, to the large-group employer plans that cover most Americans.19
Grow and diversify the health care workforce.
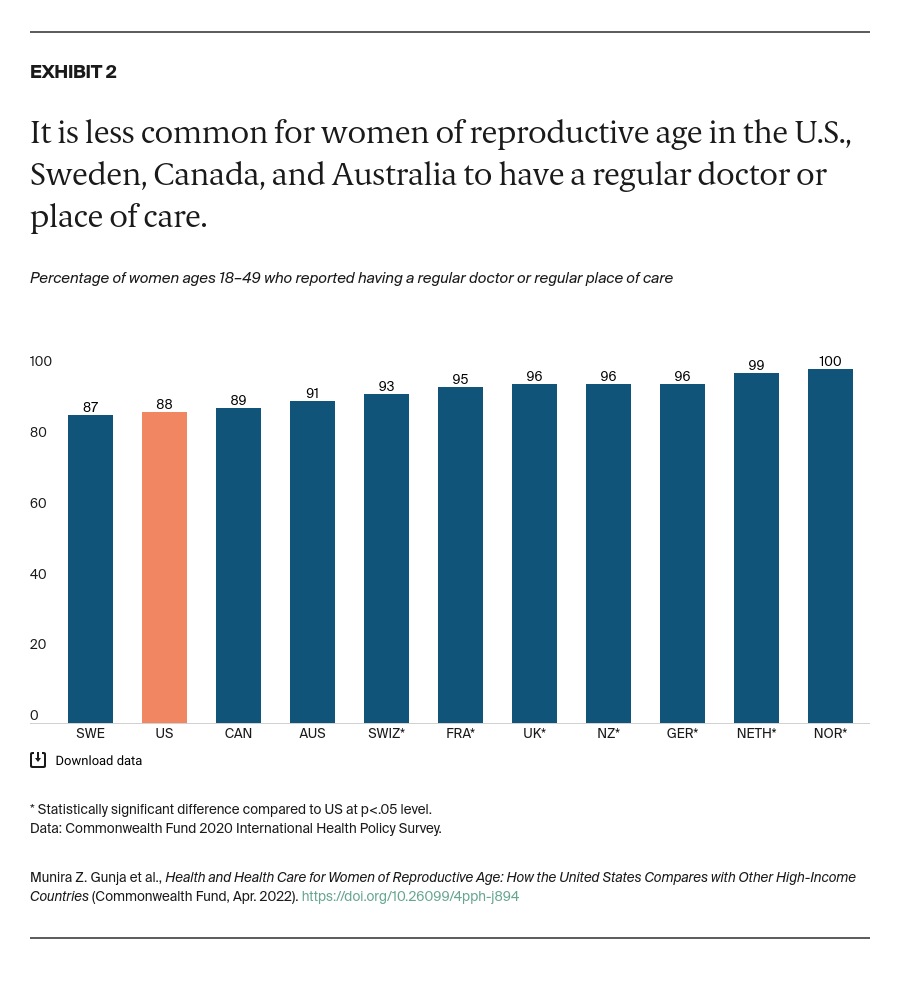
Primary care. The U.S. health care system has one of the lowest supplies of primary care clinicians — most people’s first point of contact with the health care system — of the 11 OECD countries in our survey. With a growing and aging population, the demand for physicians is likely to continue to outpace the supply.20
The U.S. also has the largest wage gap between primary care physicians and specialists and the highest tuition fees for medical students. Other countries invest more in primary care and have greater parity between wages for primary care physicians and specialists.21 The U.S. could increase the supply of primary care physicians in several ways, including subsidizing medical education to incentivize medical students to opt for primary care practice, and introducing legislation to increase the number of federally supported Medicare residency positions.22
Maternal health. In the U.S., which on a per capita basis has among the fewest maternal health providers overall and among the fewest midwives, most women see an obstetrician in a hospital.23 Top-performing health systems like those of Norway, the Netherlands, and Australia are better at preventing maternal deaths for several reasons, including the wide use of alternate models of care.24 In the U.S., expanding the maternal care workforce to include more nurses, midwives, and doulas could improve perinatal and postpartum outcomes, particularly for people experiencing significant inequities in birth outcomes.25
Greater investment in the U.S. primary health care workforce and an expansion of the medical home model to include women-centered primary health care could also have a significant impact on maternal health.26 One bill introduced in Congress, the Midwives for MOMS Act, aims to provide targeted grant funding for accredited midwifery education programs.27 Additional efforts to incentivize medical residents to work in rural or other underserved areas could increase the overall supply of maternal health providers.28
Mental health care. The short supply of mental health workers in the U.S. — 105 professionals per 100,000 people — can make it challenging for some Americans to get the help they need.29 Canada, Switzerland, and Australia have approximately twice the proportion of mental health workers. To expand its mental health workforce and integrate mental health care with primary care, the U.K. implemented its talk therapy program, Improving Access to Psychological Therapies, free of charge at clinics throughout the country.30
The Biden administration has proposed investments to increase the supply of mental health workers in underserved communities, including funding for proven behavioral health training programs and funding to expand the availability of evidence-based community mental health services.31
Conclusion
The U.S. health care system too often fails women of reproductive age. The COVID-19 pandemic has unveiled the true extent of health and racial inequities in U.S. health care and exacerbated its many weaknesses, including underinvestment in primary care and mental health.32 Across the U.S., women increasingly face threats to reproductive health care access, including abortion services, which could have a lifelong impact on physical and mental health.33 While the nation awaits the outcomes of legal challenges to state restrictions on these services, U.S. policymakers have a number of options to improve health and health care for women of reproductive age.