Abstract
- Issue: Through the budget reconciliation process, Congress could mandate that all able-bodied adults with Medicaid work at least 20 hours a week (or participate in “community engagement” activities) to retain their coverage. Congress also could lower the federal government’s Medicaid matching rate for the District of Columbia (DC), a move that would force restrictions in eligibility and possibly reductions in benefits. Prior research demonstrates work requirements do not lead to significant employment gains.
- Goal: To estimate the state-level economic, employment, and budgetary impact of a nationwide Medicaid work requirement and a reduction in DC’s federal Medicaid matching rate.
- Methods: We used the IMPLAN economic modeling system to analyze these effects, building on prior estimates from the Urban Institute.
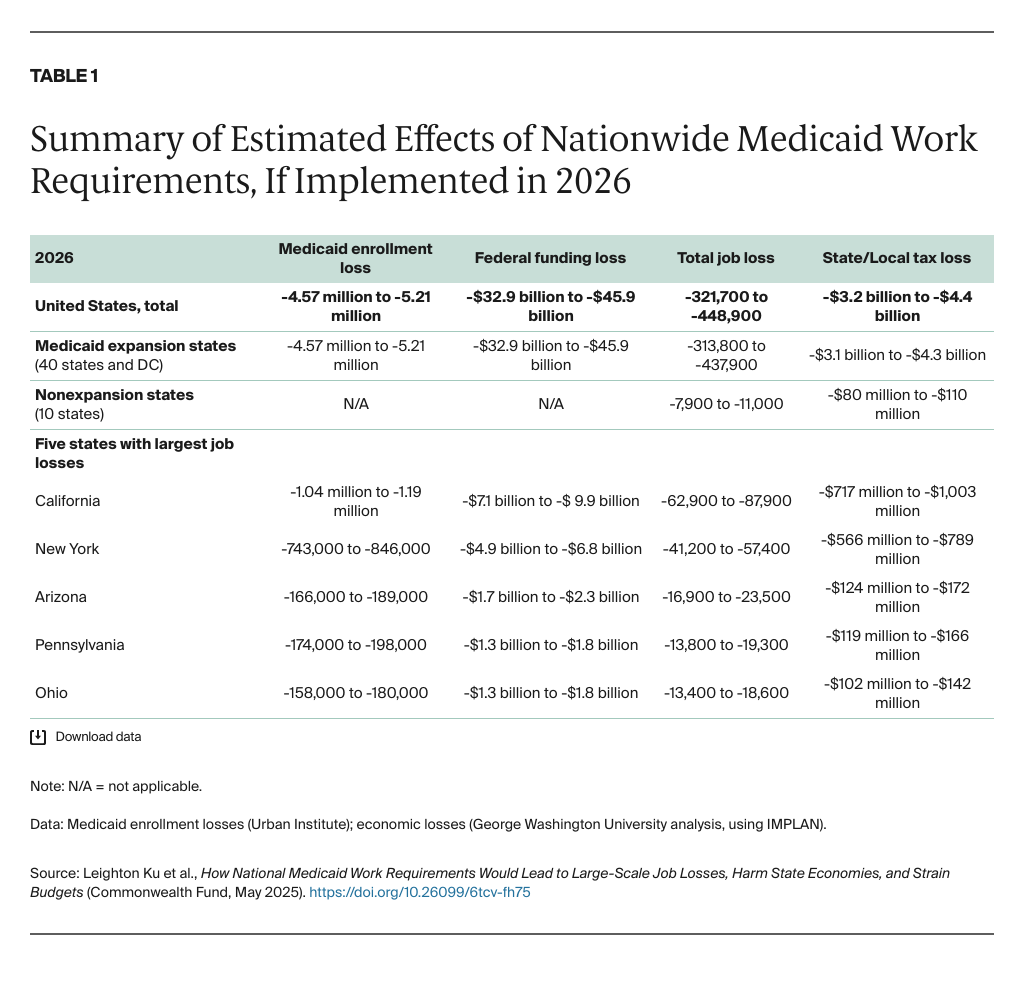
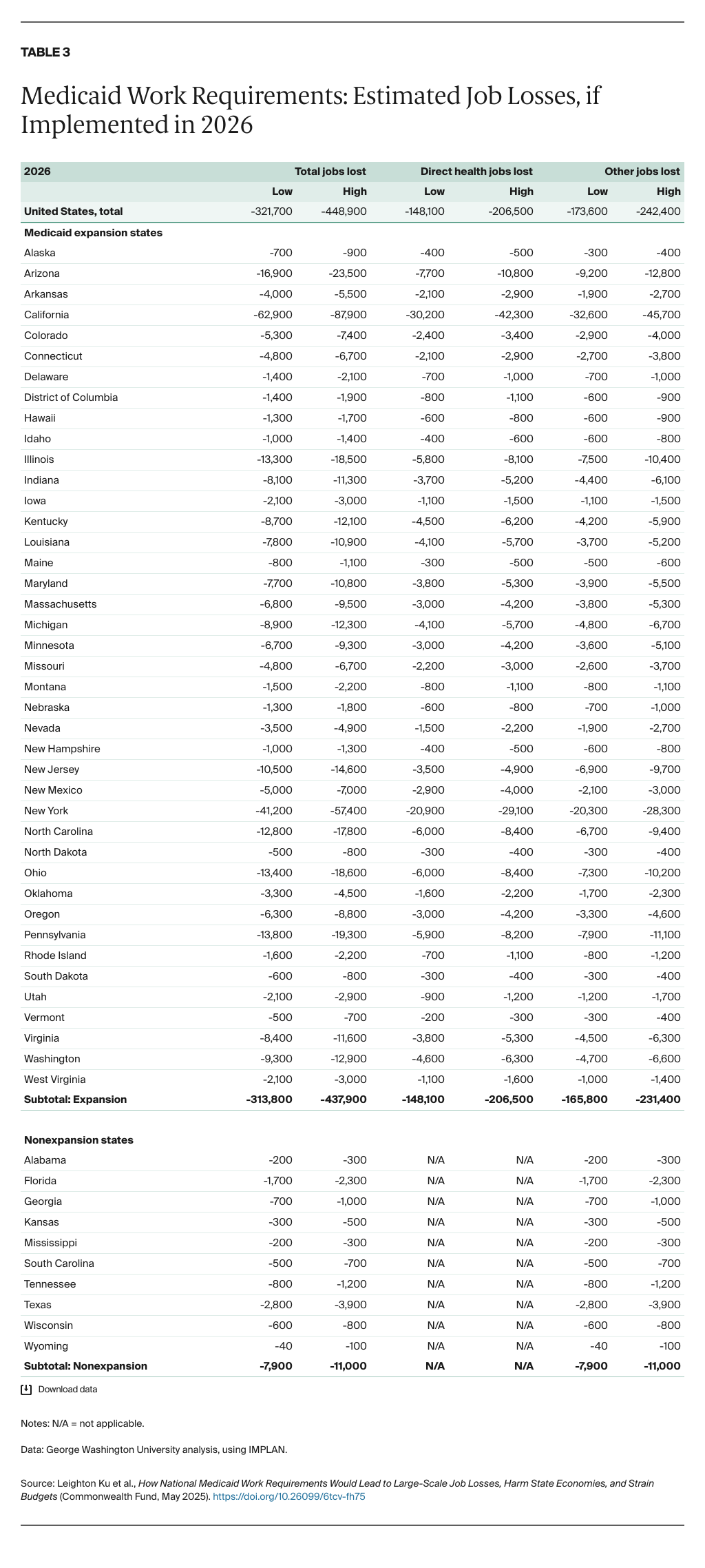
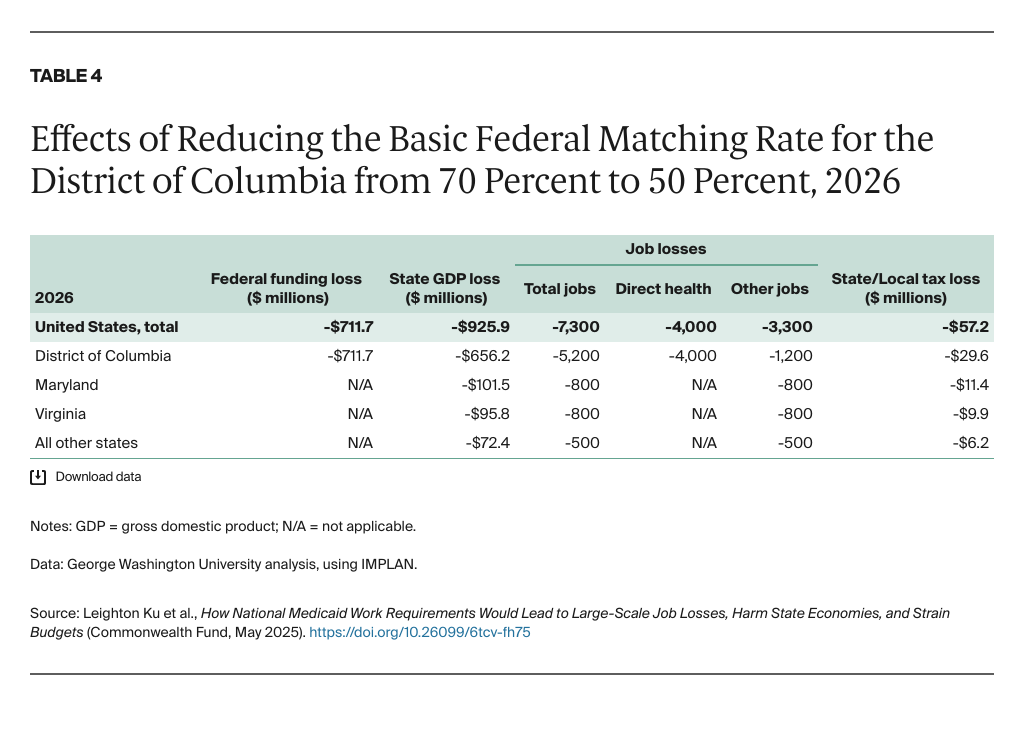
- Key Findings and Conclusions: Between 4.6 million and 5.2 million adults could lose Medicaid in 2026 if work requirements are imposed, cutting federal funding to states by $33 billion to $46 billion in the first year and $362 billion to $504 billion over a decade. States overall could see a $43 billion to $59 billion reduction in economic activity in 2026; a loss of 322,000 to 449,000 jobs; and a $3.2 billion to $4.4 billion reduction in state and local tax revenues. The DC matching rate reduction would cut $712 million in federal funding in 2026 and lead to 7,300 total jobs lost in DC and neighboring states.
Introduction
The Republican-led Congress has passed a “concurrent budget resolution” under which leaders of the House of Representatives and the Senate have agreed to identify at least $1.5 trillion in savings as part of budget reconciliation legislation to be enacted later this year.1 An earlier Commonwealth Fund brief examined the potential economic effects of cutting funding for Medicaid by $880 billion over 10 years and funding for the Supplemental Nutrition Assistance Program (SNAP) — food stamps — by $230 billion.2 In this brief, we focus on two specific proposals that could be under discussion for budget reconciliation legislation: mandatory work requirements for people with Medicaid, and a substantial reduction in the federal funding matching rate for the District of Columbia’s Medicaid program (DC Healthy Families).
A frequently discussed policy proposal is to impose mandatory work requirements on people enrolling in Medicaid.3 States would have to require certain adults with Medicaid coverage to work at least 20 hours a week — or be engaged in “community engagement” activities, such as volunteering — to retain their coverage. The details of who would be required to work, who might be exempted, or how the requirements would be structured are not yet clear. One prominent work requirements proposal, included in the Limit, Save, Grow bill from 2023,4 would cause 1.5 million Medicaid beneficiaries to lose their eligibility and result in a $109 billion cut in federal Medicaid expenditures between 2025 and 2033, according to an analysis from the nonpartisan Congressional Budget Office (CBO).5
During the first Trump administration, a number of Republican-led states sought to adopt Medicaid work requirements through demonstration projects. However, in 2019, federal courts halted approval of these projects (except Georgia’s Pathways to Coverage demonstration) after determining that the resulting enrollment loss ran contrary to the Medicaid program’s central objective — to provide health coverage.6 In December 2024, the general counsel of the U.S. Department of Health and Human Services (HHS) advised that state demonstrations were impermissible.7 Nonetheless, many states have renewed their interest in work requirements, hoping the new Trump administration might approve them.8
There have been numerous analyses of the potential benefits and hazards of work requirements.9 The consensus, based on evidence from the Arkansas and Georgia demonstrations as well as similar policies implemented nationwide for people receiving SNAP benefits, is that:
- Most adults with Medicaid either already work or should be exempt from work requirements because they are unable to work. Federal data show that 64 percent of Medicaid adults worked full or part time, 12 percent were caring for dependents, 10 percent were disabled or in poor health, and 7 percent were attending school. Just 8 percent were not working or unable to find work.10
- Many people lose their Medicaid benefits, and thus their health care coverage, after work requirements are imposed.
- Many of those losing benefits are actually employed, or should be exempt but lose their benefits anyway, owing to confusing paperwork requirements. For example, one study found that merely lacking internet access made people more susceptible to losing their benefits, owing to the difficulties this poses to meeting compliance reporting obligations.11
- Any gains in employment or income are minimal. That’s because work requirements fail to address the underlying reasons for unemployment, such as lack of proper job training, reliable transportation, or childcare support, or because too few jobs are available in their areas. CBO concluded that Medicaid work requirements would “have a negligible effect on employment status or hours worked by people who would be subject to the work requirements.”12
For our analysis of the potential effects of a mandatory Medicaid work requirements policy in budget reconciliation legislation, we drew in part from recent Urban Institute estimates of the number of Medicaid enrollees losing coverage if work requirements were imposed on able-bodied adults ages 19 to 55 who have no dependents and who are covered under the Affordable Care Act’s Medicaid eligibility expansions. Based on evidence from Arkansas and New Hampshire, the analysis estimated that 4.6 million to 5.2 million Medicaid beneficiaries would lose their coverage in 2026, or 34 percent to 39 percent of this population, after adjusting for exemptions and participation rates.13
These findings are consistent with our estimates of the impact of similar SNAP work requirements imposed nationwide. We also found that SNAP work requirements harmed Black recipients more than white recipients and that adults with disabilities, who were supposed to be exempt, also lost benefits.14
A different study looked at a broader work requirement policy targeted at people ages 19 to 64, including nonexpansion beneficiaries. It concluded that 10.1 million to 14.4 million Medicaid beneficiaries could potentially lose their coverage.15 Of course, future congressional proposals might differ from either of the policies modeled.
In this brief, we estimate the federal Medicaid funds that states would lose if work requirements were implemented in 2026, based on the Urban Institute’s estimates of coverage losses and state-level costs per enrollee. We then computed state-level changes in state gross domestic products (GDPs) and employment based on these federal funding losses. To do this, we used IMPLAN, a widely employed economic modeling system. (For more details, see “How We Conducted This Study.”)
We also estimate the impact of a budget proposal to reduce the funding that the federal government contributes to the District of Columbia’s Medicaid program. The current federal matching rate is set in statute at 70 percent; the proposal would reduce the match to 50 percent. Our analyses also show the interstate consequences of Medicaid policy changes. For example, even though the federal funding proposal directly affects DC only, the repercussions would ripple out to harm Maryland and Virginia’s economies, too.
Key Findings
Impact of Medicaid Work Requirements
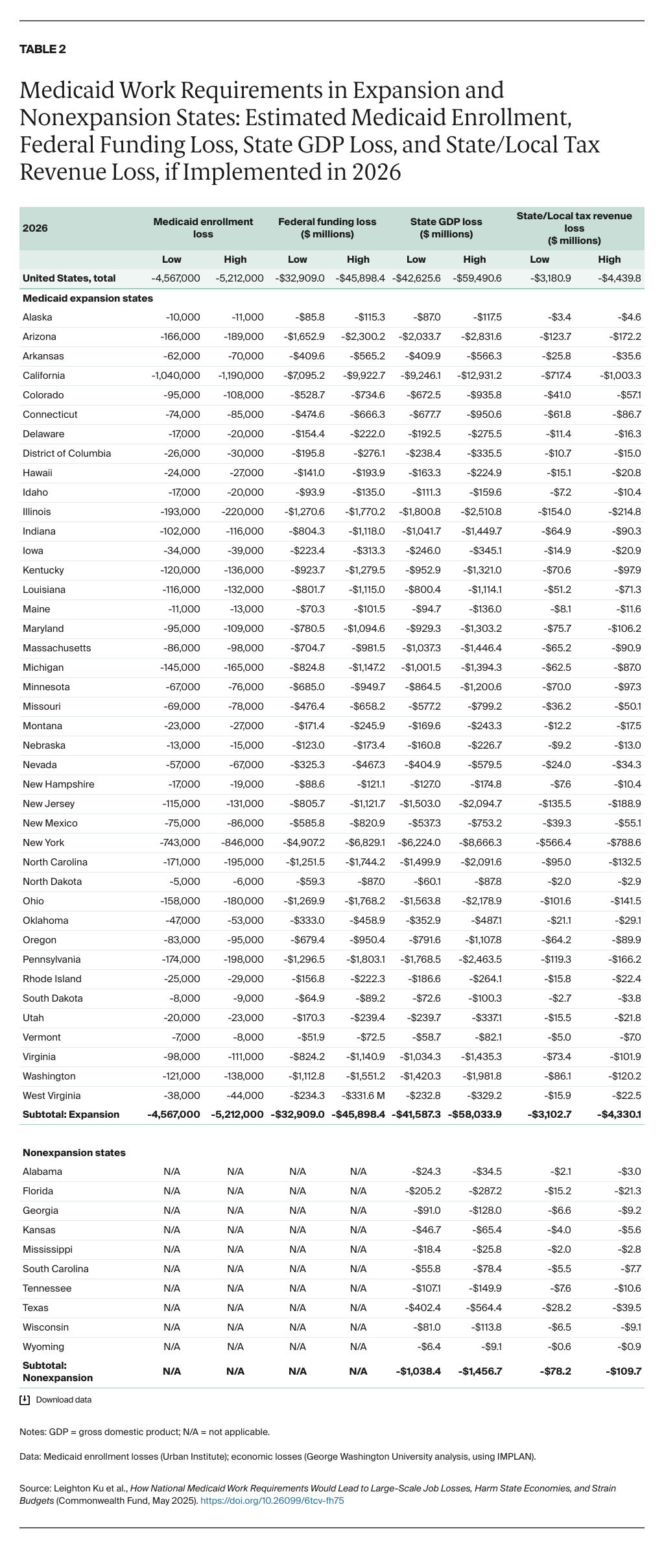
Loss of federal funding. Using the Urban Institute’s coverage estimates and state-based estimates of federal Medicaid expenditures per adult in 2026, we estimate the 40 states and DC which expanded Medicaid eligibility will lose between $32.9 billion and $45.9 billion in federal funding in 2026. The 10 states that did not expand Medicaid would not lose federal funds. These results are summarized in Table 1, with more detail about all states in Table 2 and Table 3.
Assuming implementation in 2026 and a Medicaid growth rate similar to CBO’s budget baseline,16 this is equivalent to a cumulative federal funding cutback of approximately $362 to $504 billion from 2025 to 2034 (data not shown) — the budget period used in the concurrent budget resolution.17 This is substantially higher than the $109 billion reduction over 10 years that CBO estimated in April 2023. That is likely because the Urban Institute’s estimates of coverage loss are based on more recent, better-documented evidence of coverage losses than CBO had available when it made its estimates. In addition, we used updated estimates of the costs per person, as discussed further below.18