Instead of an across-the-board payment cut, some said there should be targeted efforts. For example, CMS could set a threshold level of coding and audit plans that exceed that threshold to make sure their risk assessments are accurate; research has found variation among plans in terms of their coding levels. One person pointed out this approach could foster competition among plans. Under the current system, new market entrants are subject to a payment cut based on the coding practices of incumbent plans, which puts them at a disadvantage.
Does Risk Adjustment Worsen Inequities?
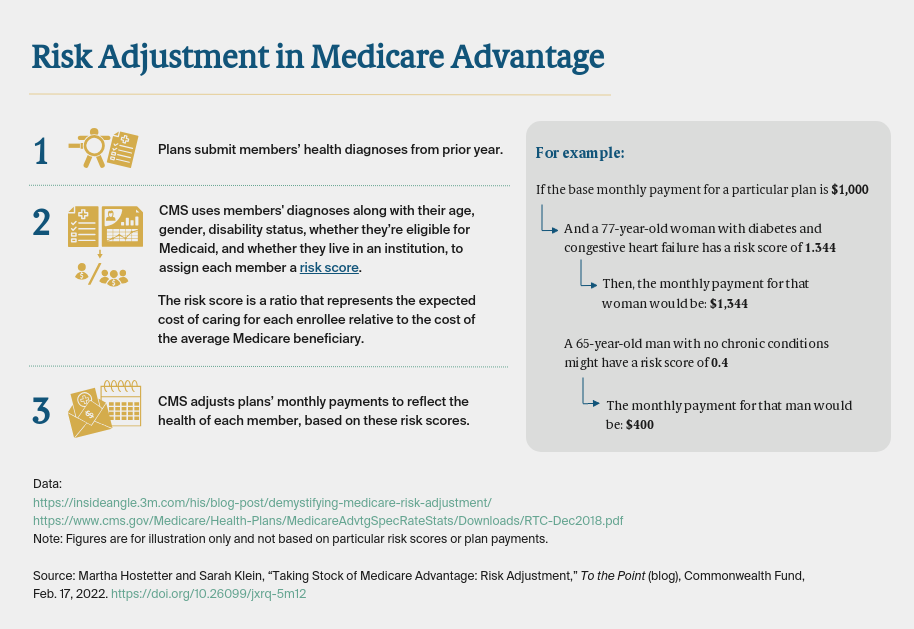
Because the current risk-adjustment model relies heavily on past medical spending to determine future payments, a few experts said it could worsen inequities in the system — for example, by underestimating the costs of caring for populations that use fewer services not because they don’t need them, but because they have poor access to medical care. These populations may include racial and ethnic minorities and rural residents living in communities with fewer providers. Without accounting for structural differences in access to care, the risk adjustment may unintentionally be exacerbating disparities.
Not everyone agreed with this: one expert argued the risk-adjustment system incentivizes plans to take on sicker patients, since they may have greater opportunity to code for their conditions, better manage their care, and earn profits.
Better Data Might Help
One way risk adjustment can be improved is by modifying the data on which the model is built.
The experts were divided on whether to make the data more or less complex. Some argued that in an age of “big data,” the model is too simple: it doesn’t account for the severity of enrollees’ medical conditions, how well they function day to day, and whether they have social supports, for example. This could mean that plans may be underpaid for high-risk enrollees and overpaid for lower-risk ones.
But others said it’s important for risk adjustment to be relatively simple and consistent from year to year. While it may be helpful for plans to identify enrollees’ unmet social needs, for example, this information may not be valid for risk adjustment given that the interactions between social circumstances and health are not well understood. One person suggested a modest tweak that could improve accuracy: using two years’ worth of medical claims, rather than one, something also recommended by members of MedPAC. A few experts suggested using different sources of data to determine risk, such as enrollees’ pharmacy use, though one person noted that such a policy could encourage overprescribing.
Several experts noted that CMS has been collecting data on Medicare Advantage enrollees’ medical encounters, documenting the clinical conditions diagnosed and the services received. The agency has begun using these “encounter data,” along with the diagnoses from health risk assessments submitted by plans, for the purposes of risk adjustment.1 Audits by MedPAC have found the encounter data submitted by plans thus far are not complete. Still, several experts said using encounter data — either along with or instead of diagnoses from health risk assessments — could eventually make risk adjustment more accurate and less prone to gaming. For example, some agreed with the MedPAC recommendation that to be counted for risk adjustment, every diagnosis in a health assessment should be associated with some actual treatment delivered.
Moving Forward
All agreed that risk adjustment is worth getting right to ensure plans are paid appropriately based on how well they keep members healthy, not how well they code. Giving plans incentives to find innovative ways to help patients, including those with more complex needs, is key to whether the program fulfills its promise.