Are SNPs Meeting Beneficiaries’ Diverse Needs?
Most of the experts viewed SNPs as a good platform for tailoring care to people’s needs, given the plans’ latitude in developing care models and incentives to manage medical risk. For example, an I-SNP can hire nurse practitioners to visit beneficiaries in nursing homes to help keep them stable and avoid medical complications.
But experts also agreed not enough is known about whether and how SNPs are customizing care. Each SNP must create a Model of Care document detailing the population it serves, plans for meeting their needs, provider networks, and how it will measure and improve quality. The National Committee for Quality Assurance must approve these documents, but little is known about how they translate into practice.
More should be done to assess the impact of SNPs on beneficiaries’ health, experts said. For example, quality measures could be fine-tuned to detect differences in treatment and outcomes among, say, younger beneficiaries with disabilities and frail older adults. It doesn’t help that the Centers for Medicare and Medicaid Services (CMS) allow Medicare Advantage carriers to combine the quality scores of plans of different types (e.g., SNPs and non-SNPs) to establish the star ratings that Medicare beneficiaries rely on to select plans. Experts suggested it would be more useful to rate the performance of each type of special needs plan separately.
Are SNPs Addressing Members’ Nonmedical Needs?
In 2018, Congress gave Medicare Advantage plans enhanced flexibility to offer nonmedical benefits that address the social determinants of health, such as food insecurity. This year, more plans are offering services like pest control and home-delivered meals. Some experts welcome this trend to test whether providing nonmedical services can improve health and thereby reduce health care costs.
SNPs are somewhat more likely than other Medicare Advantage plans to offer nonmedical benefits. SNPs can afford to because the rebate payments they receive from CMS when they bid below regional spending benchmarks tend to be higher than rebates for other Medicare Advantage plans. This is because the rebates are increased to account for members’ medical risks. More information is needed to assess whether these extra benefits are reaching those most in need, some said.
Experts called for studies — with incentives or mandates from CMS to participate — to explore which services help which SNP enrollees. Do home-delivered meals seem to reduce hospitalizations among those with congestive heart failure, for example? Having information on whether and how nonmedical services affect health could inform policy for the Medicare program and beyond. Experts agreed CMS’ proposed rule requiring D-SNPs to ask beneficiaries about their housing stability, food security, and access to transportation as part of their health risk assessments is a positive step toward understanding how social circumstances affect beneficiaries’ health.
Do D-SNPs Promote Integrated Care?
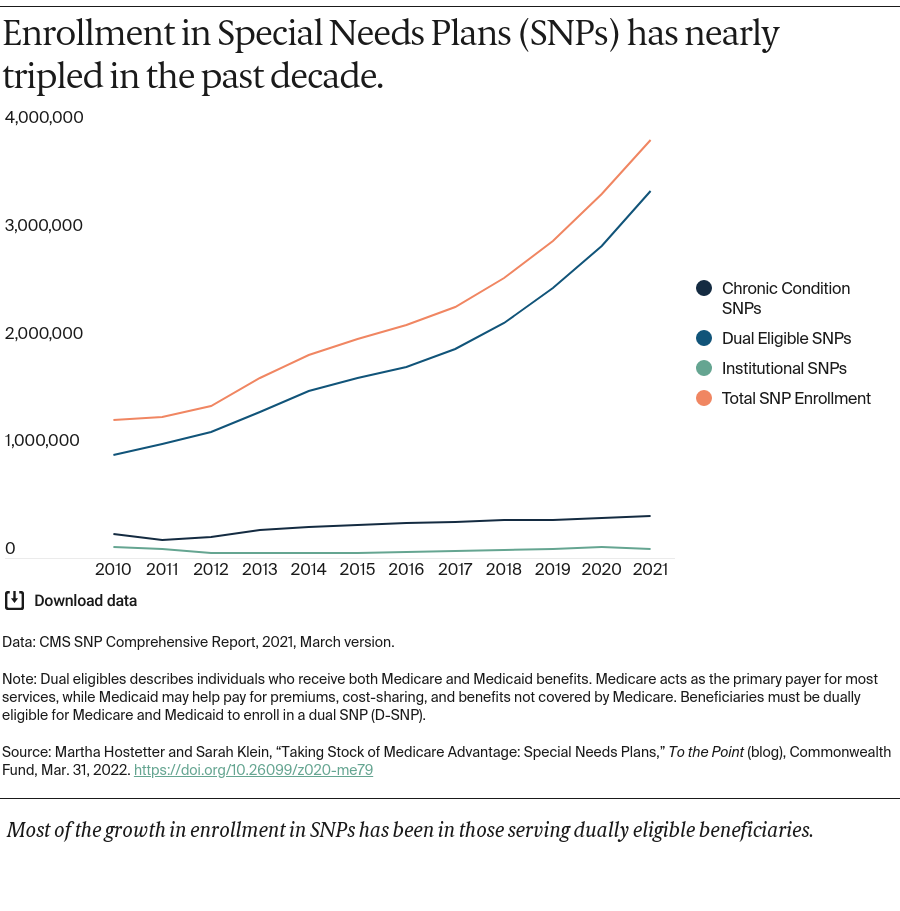
Dually eligible beneficiaries may receive fragmented care because of the challenges of dealing with two different programs. Beneficiaries may, for example, struggle to find providers who accept both Medicare and Medicaid. Some beneficiaries require coordination between their in-home supports (usually paid for by Medicaid) and their medical care (usually paid by Medicare), but when the programs are administered separately, that rarely happens. In the financial alignment initiative, CMS partnered with states to test ways to align Medicare and Medicaid programs. With this demonstration now winding down, some policymakers are looking to D-SNPs to carry on this work.
D-SNPs are required to contract with the states in which they operate to outline how they will coordinate members’ Medicare and Medicaid benefits. But most experts viewed the requirements as minimal, noting that only a handful of states mandate greater integration. They called on states to adopt proposals put forth by the Medicaid and CHIP Payment and Access Commission and the Medicare Payment Advisory Commission. For example, all states could:
- partner with D-SNPs to align their communication materials, benefit networks, and vendors for services like durable medical equipment.
- prevent D-SNPs from enrolling “partial duals,” or Medicare beneficiaries who receive some financial assistance from their state Medicaid programs to pay out-of-pocket costs in Medicare but don’t qualify for other Medicaid benefits. This would enable plans to offer a uniform set of benefits and keep their focus on populations that would benefit from greater integration of Medicare and Medicaid services.
- partner with D-SNPs to develop supplemental benefit packages that complement those in Medicaid.
In states that rely on Medicaid managed care:
- Require D-SNP insurers to also offer Medicaid managed care plans and align enrollment so that people eligible for Medicare and Medicaid benefits receive them from a plan capable of coordinating them.
Some experts would go further, for example by preventing Medicare Advantage plans other than D-SNPs from enrolling people who are dually eligible. They note that many of the selling points on which Medicare Advantage plans market themselves, such as low or no premiums, are already part of the benefits that dually eligible beneficiaries are entitled to under Medicaid.
Experts observed that because most state governments don’t have expertise in Medicare, they will need support to promote integrated care. Some suggested they may also need incentives. Otherwise, states that invest resources in promoting integration that improves patients’ care and avoids hospitalizations would see the savings accrue to D-SNPs, not states. This is because for those dually eligible, Medicare is the primary payer for hospital and physician services while Medicaid covers long-term care.
Moving Forward
Experts agreed that D-SNPs and other special needs plans have the potential to improve care for some of the highest-need beneficiaries. But to leverage their potential, policy changes are needed to shed light on how well they are functioning and to promote high-value, well-coordinated care.